Muppet came back in a good mood and wishes to present an easy case. Radiographs belong to a 73-year-old male smoker with a moderate cough. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Findings: PA chest shows a mediastinal mass protruding at the level of the aorto-pulmonary window (Fig 1A, arrow). The mass is also evident in the lateral view (Fig 1B, arrow).
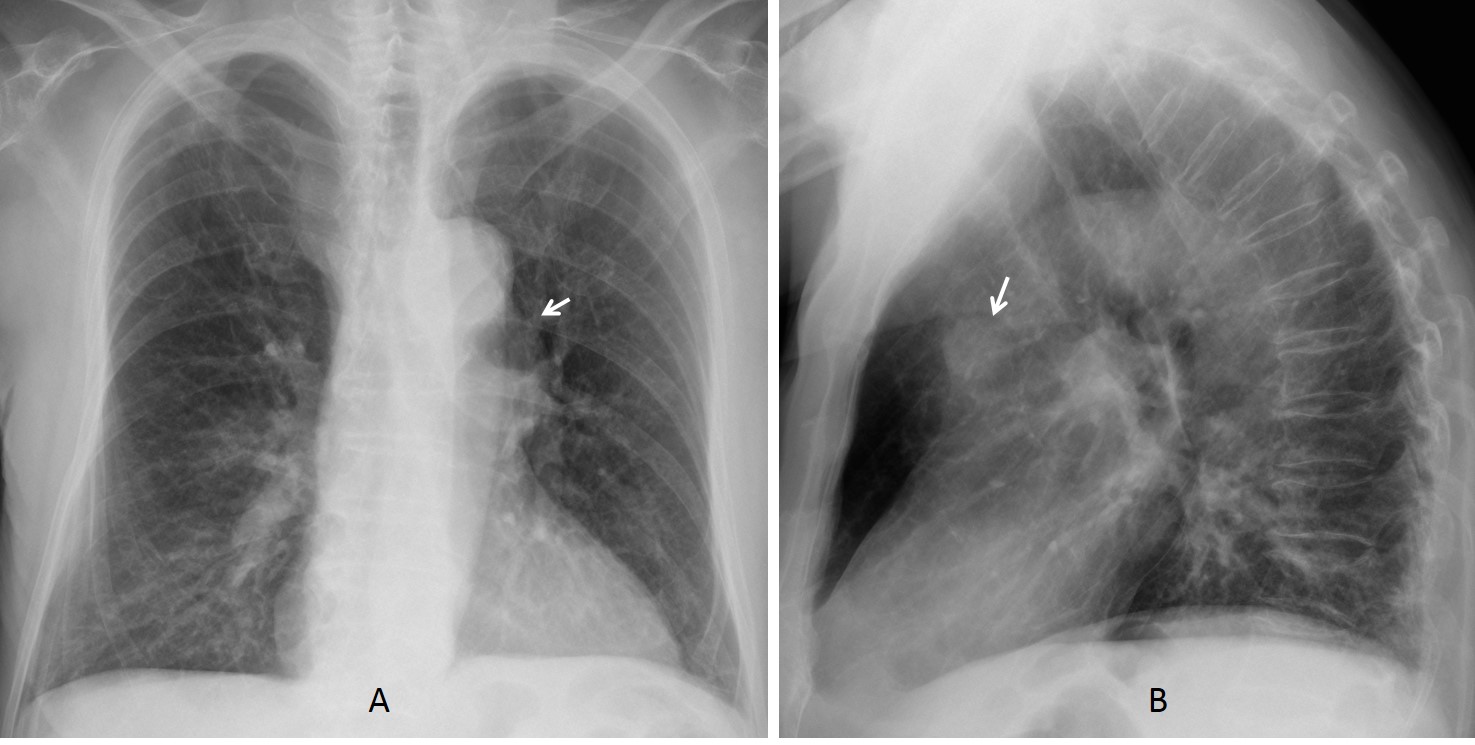
Fig. 1
Radiographs taken five years earlier did not show the abnormality (Fig 2).
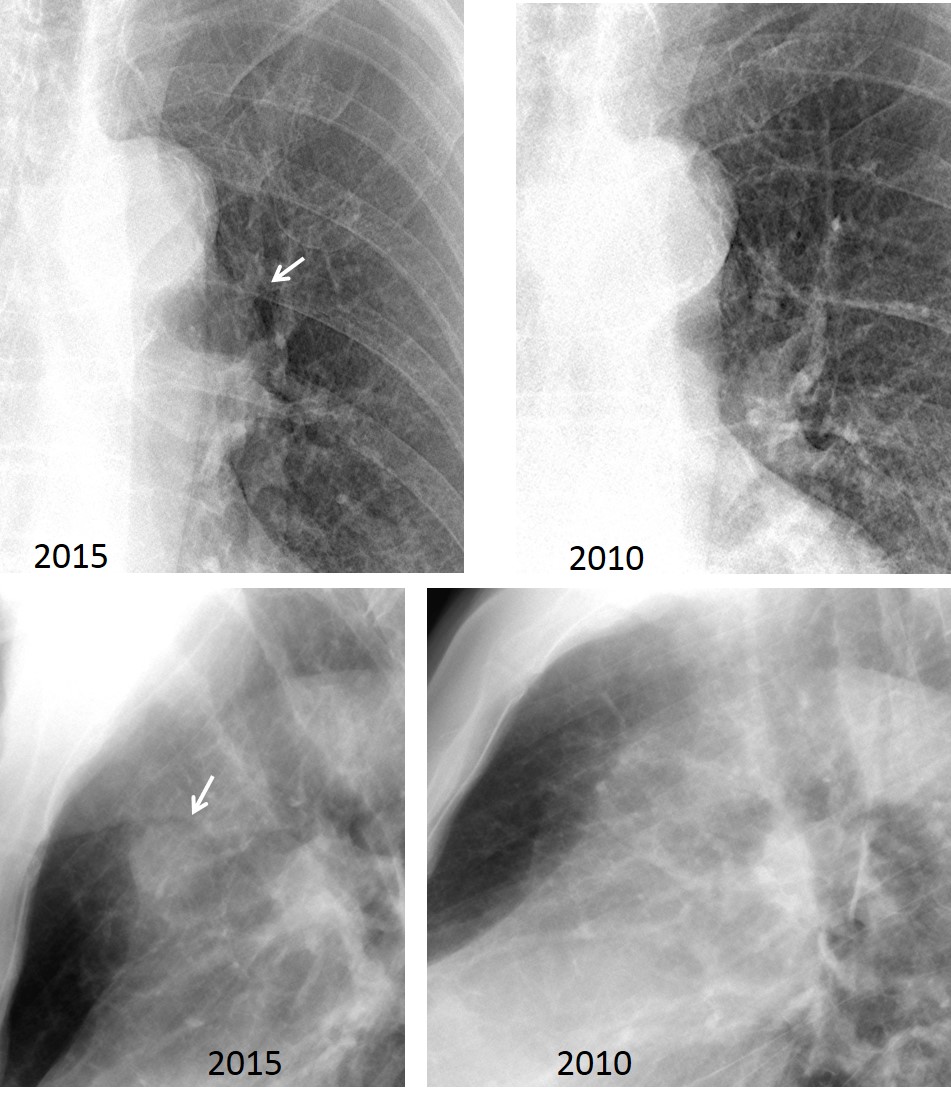
Fig. 2
The location of the lesion suggests enlarged lymph nodes as the first possibility, although other etiologies cannot be excluded. Enhanced axial and coronal CT demonstrates that the mass represents a saccular aneurysm arising from the aortic arch (Fig 3, arrows).
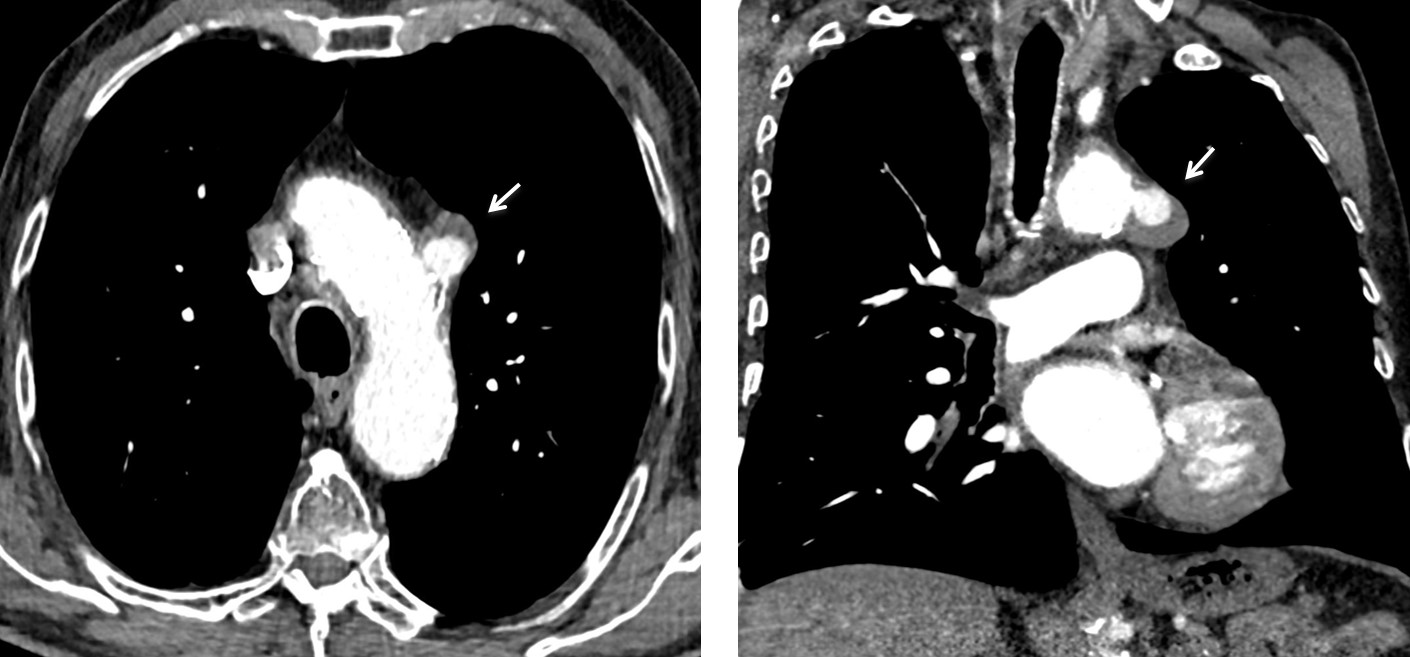
Fig. 3
Final diagnosis: saccular aneurysm of aortic arch.
Congratulations to Gus, who was the first to discover the abnormality
Teaching point: remember that any mediastinal mass may have a vascular origin. Enhanced CT should always be performed to explore this possibility.




Hello after Easter:)
there is overinflated of the lungs with flattened of diaphragms and widened of intracostal spaces- in smoker man I suppose COPD. In other hand I don’t see bullosa – maybe one in retrosternal space?
Main pulmonary arteries are widened with increase of vascularity in lungs.
There is also increased size of heart.
My diagnosis is pulmonary artery hipertension secondary to changes of COPD.
What you say is probably true and compatible with the patient’s history. But it is not the reason for showing this case. Try again.
Thoracic aorta aneurysm.?
I hope muppet and you had a good vacation. thank you for your work with the case blog……
answer:
widened ant. mediastinum pronounced on the right suspicious of mass primarily enlarged lymph nodes. prominent pulmonary arteries suspicious of pulmonary hypertension. degen. spine
An ill – defined left hilar opacity associated with widening of the superior mediastinum by a smoothly outlined opacity , the picture suggestive of central bronchpgenic carcinoma with right para-tracheal enlarged lymph node ( metastatic lymph node )
I agree with you about the mediastinal mass. Where do you see the associated carcinoma?
mmm, the old aged patient , the history of smoking, the mass opacity itself shows fine speculation at its margin , also collapsed D6 vertebra, all of these finsings take my mind to malignancy
I think it might be a posterior mediastinal, paraspinal, mass on the left. There is smooth outline on the left superior mediastinum passing to level of left hilar region without silhouette with aortic knob, descending aorta or left hilar. On lateral view, the retrosternal space is clear. The neurogenic tumor, may be ganglionic in origin, is suspected.
Background changes of chronic bronchitis and emphysema.
A mediastinal mass in the region of the aortopulmonary window on the frontal view, and projecting over the ascending aorta on lateral view; consistent with a medial mediastinal mass. Generalized osteopenia with anterior wedge compression of D6 vertebral body.
taking into consideration:
– mediastinal mass – may be right paratracheal adenopathy;
– and diffuse interstitial changes
Posibil is Sarcoidosis
Is there is opacification(neoplasm) on the right side under the clavicle?
Para spinal masses with lower vertebral end plate irregularity. Infective spondylitis?
I think i saw a superior mediastinal mass on the right and a left sided mass near the aortopulmonary window. Seems that the left bronchus is pulled downwards also, so maybe the left sided mass is the primary carcinoma with mets to superior lymph nodes?
I agree about the mass in the aortopulmonary window. However, I believe that the widening of the right superior mediastinum is due to the innominate artery.
I do not see drawing lung on the right apical , and are fibrous- change after and under the clavicle right – possible sequelae tuberculose
Aparte de los cambios de enfisema, llama la atención que la ventana aórtico-pulmonar esta ocupada por una opacidad y en la proyección lateral se ubica anterior, a nivel de la aorta ascendente.
Pienso que se trata de una masa o tumor posiblemente pulmonar.
Además hay un acuñamiento anterior del cuerpo vertebral de D6 por osteoporosis.