
Dear Friends,
My good friend and former resident Romá Vidal sent me some images of a 39-year-old man with cough and moderate fever. Have a look at the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. TB
2. RUL collapse
3. Fungus ball
4. None of the above
Click here for the answer to case #115
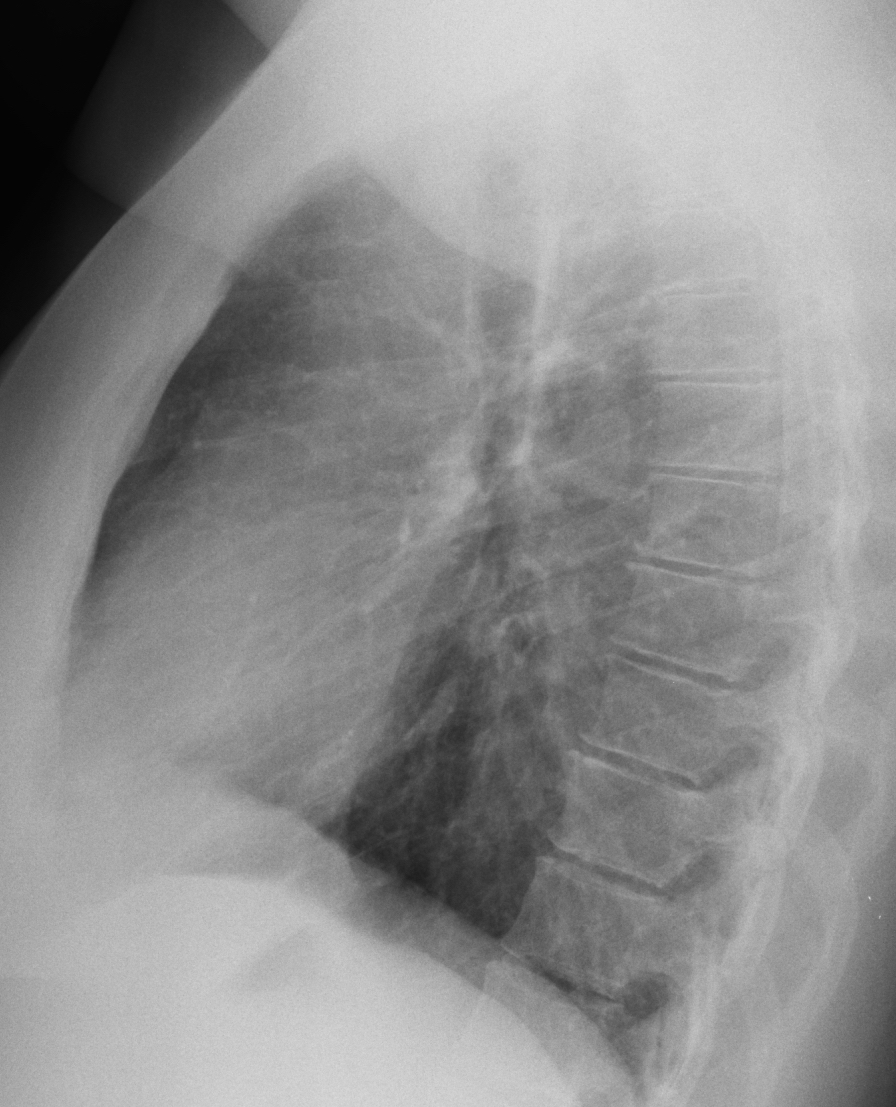
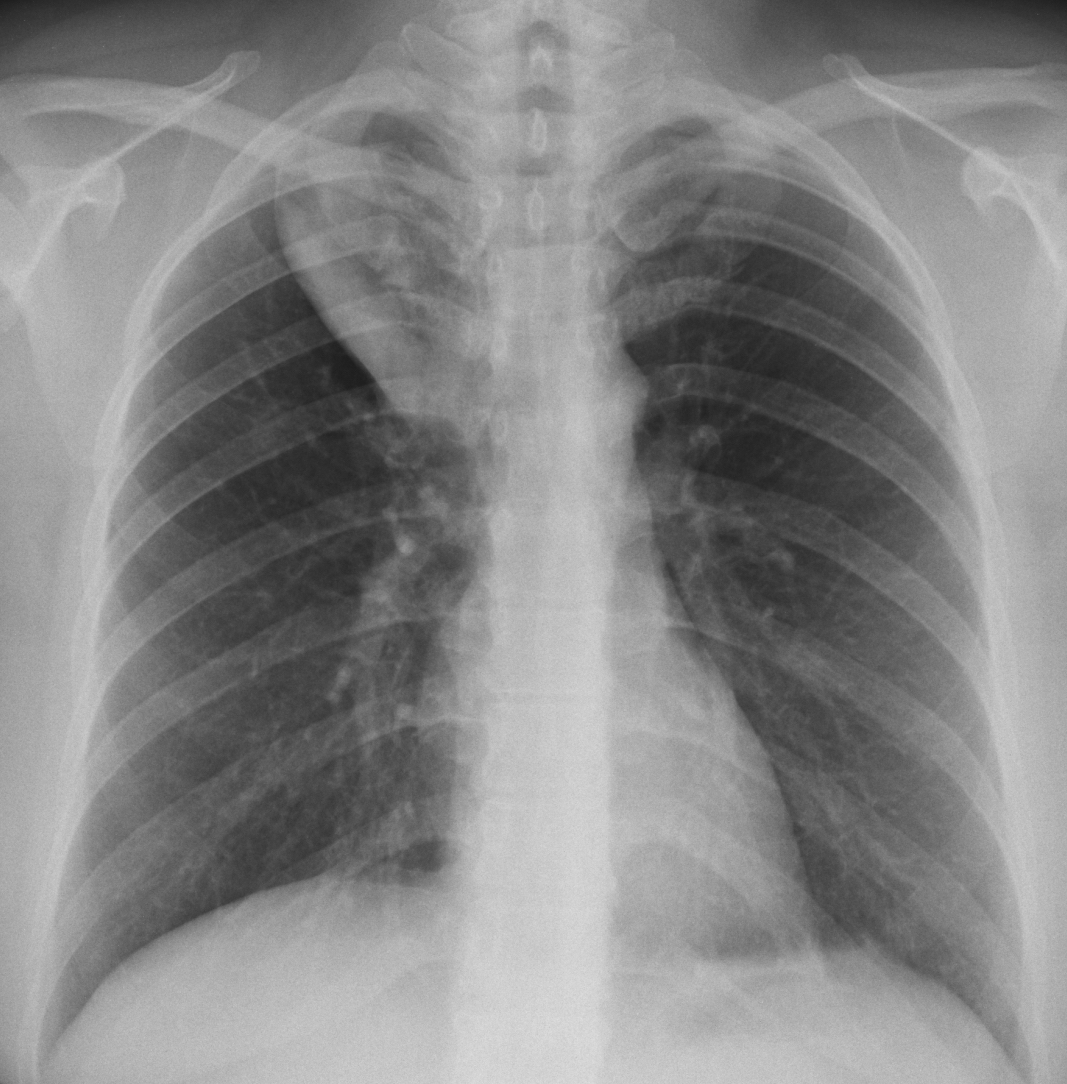
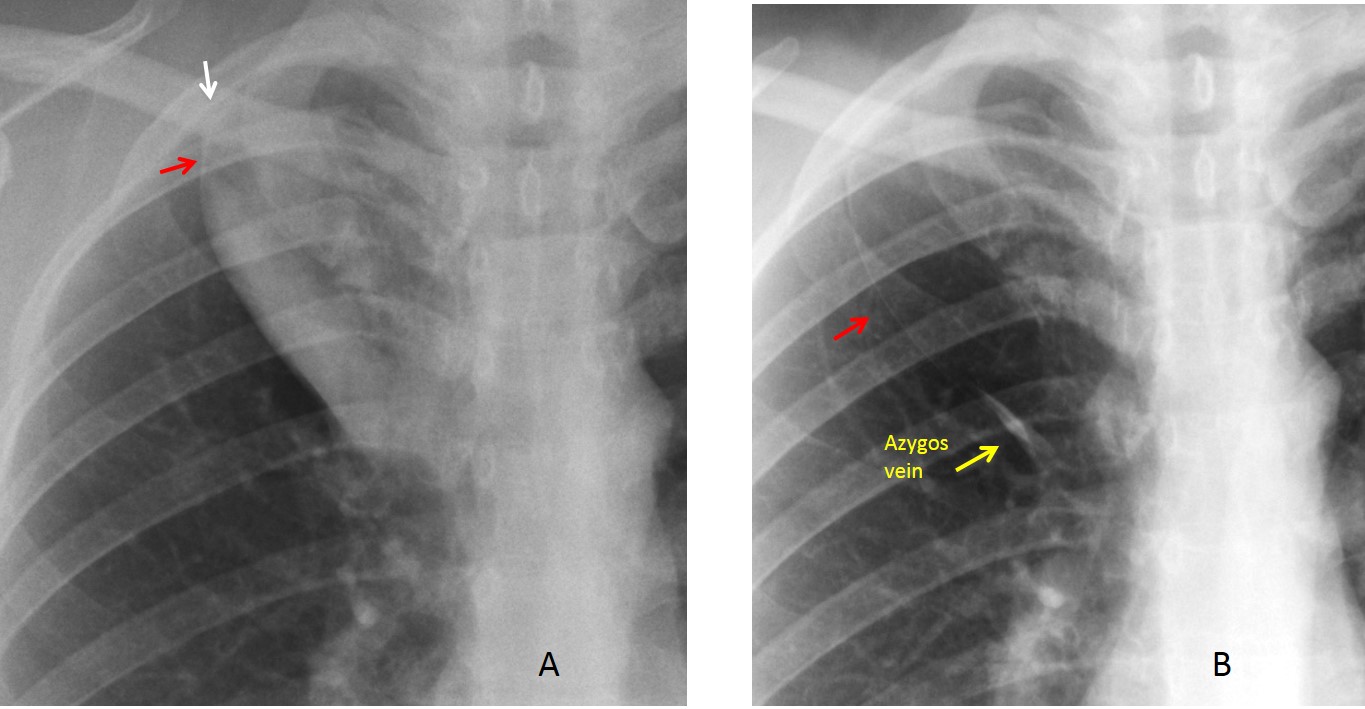
Findings: the lateral view is unremarkable. PA radiograph shows a well-defined triangular opacity in the right upper lung that at first look simulates an RUL collapse with a bulging fissure. The fact that the trachea is in the midline and the right hilum is not elevated go against this possibility. The clue to the diagnosis lies in recognising an upper trigonum (A, arrow) and a fissure (A, red arrow), which are the hallmark of an azygos lobe. The findings can be explained by an inflammatory process within the azygos lobe, simulating an RUL collapse.
A follow-up radiograph a month later shows the disappearance of the pneumonia and confirms the azygos lobe (B, arrow).
Final diagnosis: azygos lobe pneumonia
Congratulations to Fares, who was the first to mention the right diagnosis, with Lola la Piconera and Cocotet as close seconds.
Teaching point: remember that pneumonias have ill-defined margins except when limited by a fissure.


4, 4, 4, 4, 4, etc etc
Do you have any suggestion?
On lateral film, if u follow the outline of the ‘upper lobe opacity’, you can trace the outline out of the hemithorax.
So i think it is 4
Yo creo es el numero 2, sin embargo por la clínica podría tratarse de un foco neumoníco sobrepuesto allí tambien
Está elevado el hilio?
I think there is a pathology in the azygus lobe, may be a pneumonia
I would say 4 Patient has an azygous lobe. There is a dense tubular structure following the azygous fissure as well that could represent a dilated azygous vein inside the fissure. Causes of this dilatation could be for example an anatomic abnormality or a pathological condition like IVC thrombosis in the venous retourn that shunts a lot of blood to azygous system. But this usually doesn’t cause cough nor fever….I can not see the cause of the fever unless as Fares says this tubular opacity corresponds to a pnaumonia.
….l’opacità’ e’ di pertinenza della scissura da v. Accessoria lobo azygos…..quest’ ultimo e’ normo trasparente ed indenne….la patologia e’ della pleura…..lipoma o tumore fibroso della pleura(dd con TC)…..saluti da Bari…..ed attenti a Vidal, quello della Juve….e’ un terrore X le squadre avversarie…..arrivederci a …..Londra !
We’ll see tomorrow. Anyway an Italian coucher or an Italian team is going to succeed.
And a Spanish team or a Spanish coach!
grazie >>>>>>>Lola!!!!!!!
A consolidation in the azygos lobe?
4, azygous lobe pathology, most likely a pneumomic consolidation. Consolidation tends to be denser outlining the fissure. D/d encysted fluid in azygous fissure. Azygous vein enlargement is usually more subtle, medially and the patient will not have a history of fever. Comparison with prior film if possible, will be helpful. If not, will recommend follow up cxr after appropriate antibiotic therapy.
Also I don’t think azygous vein is enlarged based on the lateral view.
Nice discussion. I like it
TB
Loculated pleuropneumonia in the accessory azygous lobe…
I think none of the them is correct acording these ,
1, both hemidiaphragm and both hillum at normal it show no decrease in lung size.
2. No mediastinal , tracheal devetion it show no volume loss in RUL and no collaps.
3.no LAp was shown, in pA And LAT ,
I think its an azygus lobe ,,
I agree with Amir in point 1 and 2. There is no corresponding changes on lateral view. But is there an opacification in the retrotracheal triangle? Posterior tracheal line a bit wider? I also think about structures coming from posterior mediastinum like duplication cyst, vascular anomalies,neural tumors or diverticuli.
This is a very difficult case Dear Doctor.
I am looking forward to your answer. ☺
Actually, it only looks difficult. Analize the image and the answer is obvious. Don’t give up!
Although a small density was show at LAT weiv ant port of T4 vertebra can be a fungal ball…..but i am not sure
Golden S sign
Could be a normal variant (azygus lobe type A trigonum parietale lateral in pulmonary apex ) but because the patient symptoms consolidation is the first thinking.
By the way Dr Caceres, all your former residentes looks like your self and the mupet as much as Dr Roma Vila does?
Dr. Vidal is younger and more handsome
Dear Sir
Greetings
Looks like option 4 as pathology seems to be consolidation involving Azygous lobe…mimicking positive cervico thoracic sign
Good diagnosis. See answer tomorrow
I thank that it is consultation in the right upper lobe apical segment with cavitary changes associated with multiple hilar LNS – TB is my first choice
….grazie mitico blaugrana professore per i saluti portatemi dal mio amico e collega dr Florio , Bari, da Davos….sono veramente onorato di tutto questo…..spero di incontrarti di persona , magari a Barcellona….per il caso in oggetto devi comunque convenire che in una DD ci poteva stare anche la mia diagnosi….Incredibile MESSIIIII !!!!!
Hope we will see a Barça-Juve!
Hai I’m doctor gela fron the Philppines i can see the real X-ray of the heart