Since summer is coming (Game of Thrones revisited), I am presenting an easy case today. Images belong to an asymptomatic 67-year-old female with scleroderma. She had a lung transplant last year and a gastrostomy one month ago.
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
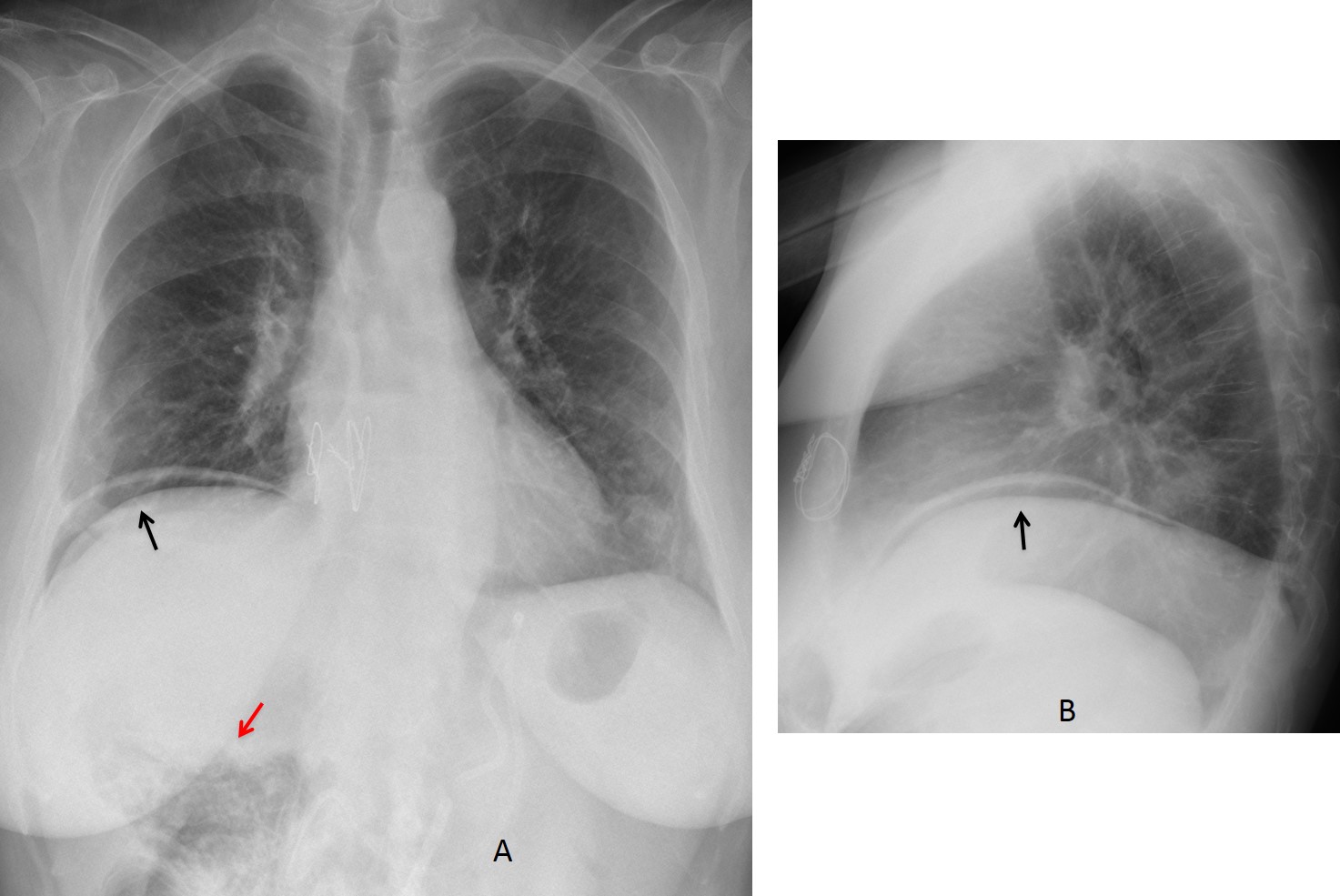
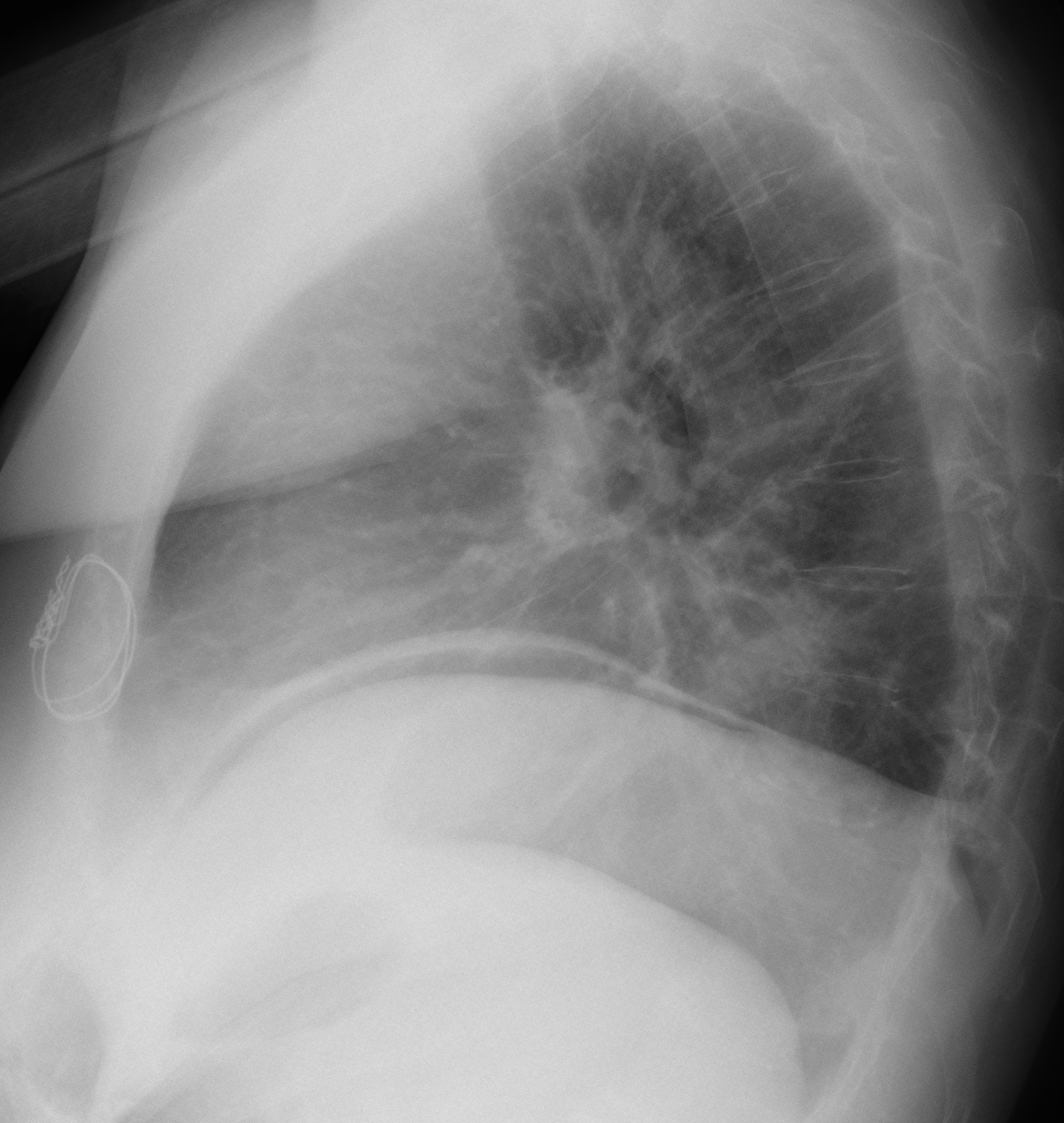
Findings: there is free air under the right hemidiaphragm (A-B, arrows). There is also a bubbly appearance of the hepatic flexure of the colon (A, red arrow), which suggests intestinal pneumatosis.
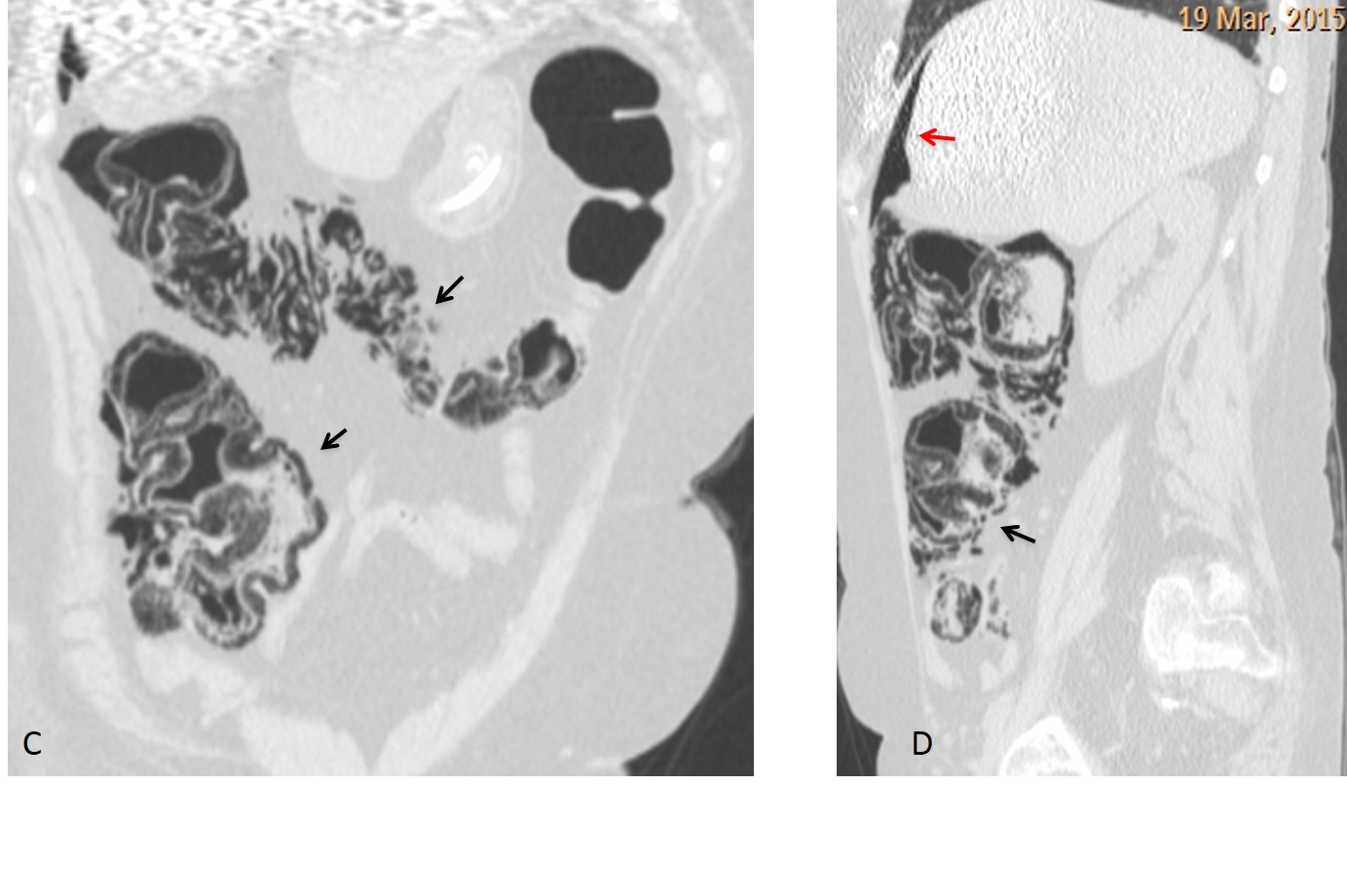
CT confirms pneumatosis of the right colon (C-D, arrows) and the free air (D, red arrow).
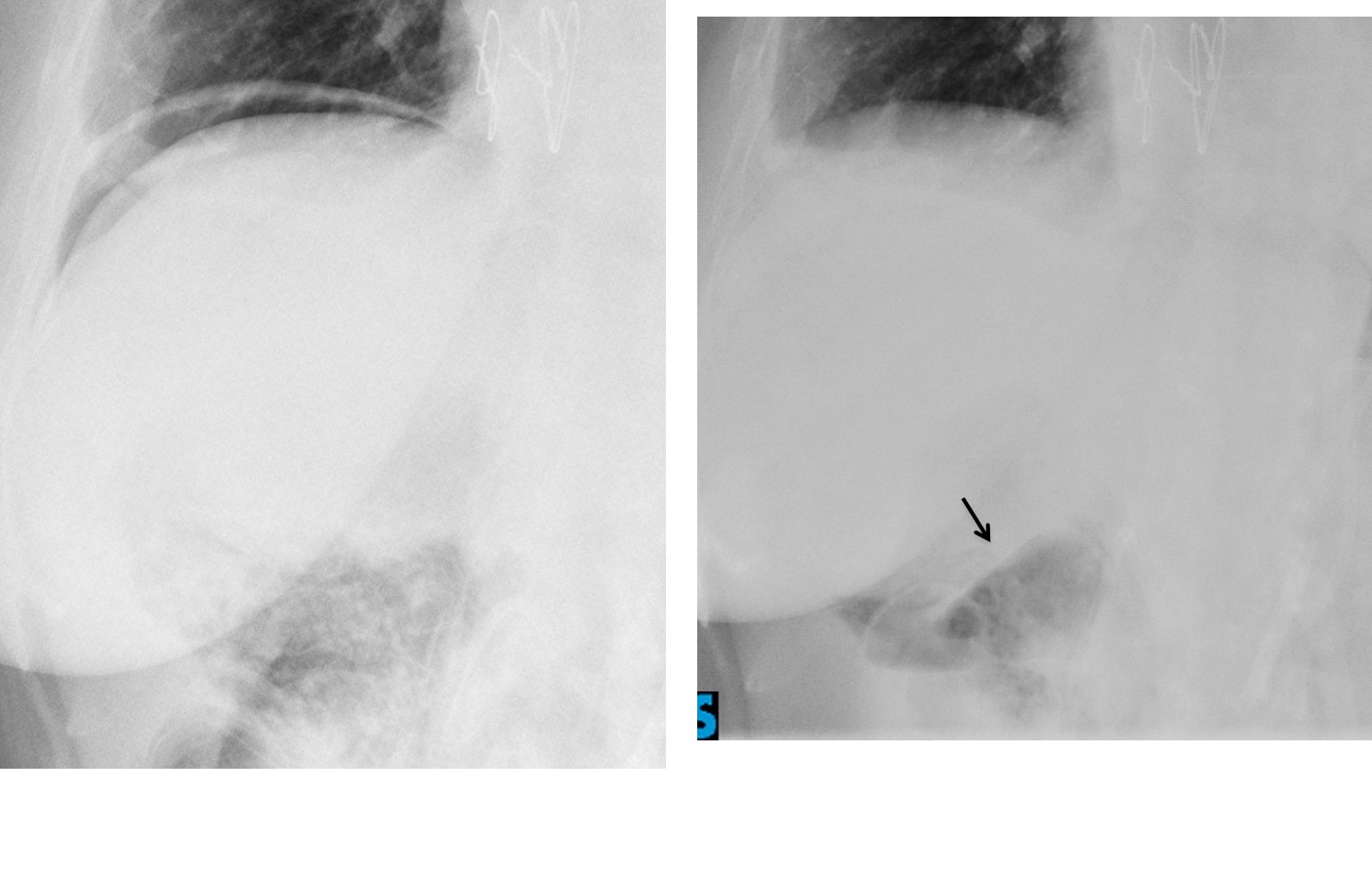
As the patient’s symptoms were minimal and scleroderma is known to cause pneumatosis, it was decided to wait. Four days later the pneumoperitoneum disappeared and the appearance of the hepatic flexure had improved (F, arrow).
Final diagnosis: pneumatosis cystoides intestinalis with pneumoperitoneum, probably secondary to scleroderma.
Congratulations to Fares, who mentioned the right diagnosis.
Teaching point: remember that free abdominal air is either due to instrumentation or perforation of a hollow viscus. Intestinal pneumatosis should always be considered, especially if the appearance of the bowel suggests it.
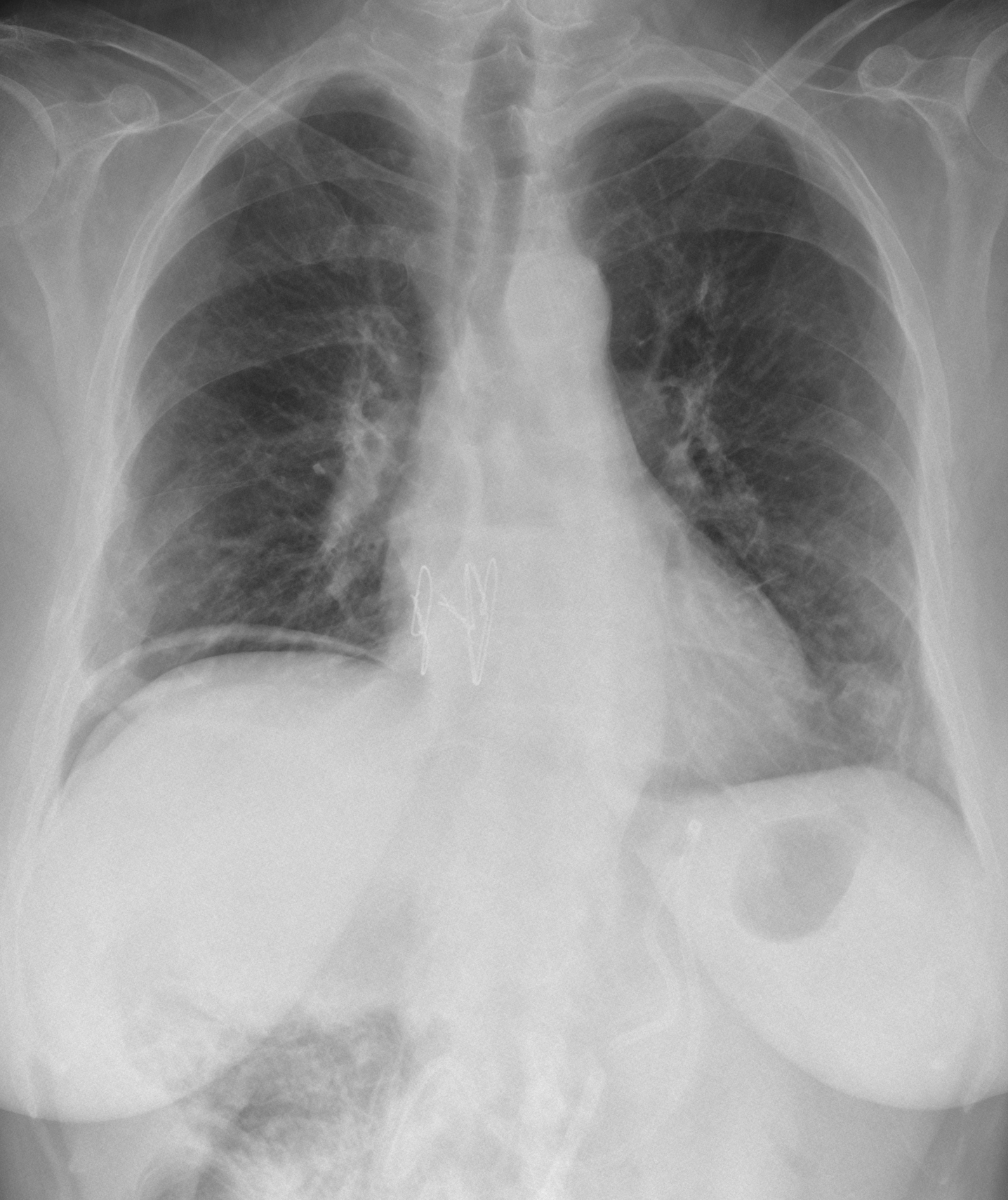


Right pneumoperithoneum. Elevated right hemidiphragm.
…il caso è facile, anche se il mitico professore non dice sempre tutta la verità !Il trapianto di polmone non c’entra nulla….c’è stata una PEG, per la patologia esofagea e quest’ultima ha avuto una complicanza…si è sfilato il catetere di abboccamento sulla cute, per la nutrizione enterale ed esso è visibile,”accartociato ” nel lume gastrico deteso…naturalmente la mancata connessione del catetere con la cute ha provocato un pn-peritoneo…TRIPLETE in vista ?
Triplete is obvious! Hope to enjoy watching Barça-Juve with my good friend Lorenzo Bonomo.
No comment about your diagnosis. Too early in the game.
il prof Lorenzo Bonomo di Andria (BARI) è colui che mi insegnato l’Ecografia , nel lontanissimo 1983 e lui sa che la mia superspecialità è la radiologia “pediatrica” ….
Hello,
Free air under right diaphragm. There is also dilatation of esophageus.
Perforation of gastrointestinal tract after gastrostomy?
Two things not compare – that patient is asymptomatic and it’s too easy for Caceres’ Corner:)
I am innocent! The Muppet made me do it!
Elevation of right diaphragm
there is Air subcutaneous in soft tissue on the right with possible comunication with the right diaphragm
complication post omentopexy?
CRAZY ?
Plus i think i see Air fluid levels on esophageus and a (mass) opacity posterior of cardiac silhouette on lateral view, post transplant lymphoproliferative / lymphoproliferation disorder (PTLD)?
I think its presence of air cause of the past surgery .If there is no clinical sintomps I think isth air from the surgery of the past month.
The patient did not have any pneumoperotoneum one week before the current radiographs were taken.
I go with interposed bowel gas between the liver and the right hemidiaphragm (Chilaiditi’s sign). As i see some intestinal structures on the level of the liver.
Chilaiditi is one of the D.D. of pseudopneumoperitoneum.
Right sub-pulmonic effusion/ empyema
Pneumoperitonum , obliterated aorto pulmonary window + suggestion of prominent lt pulmonary artery
There is mild elevation of right hemidiaphram. This may be normal in this case, upto 2interspaces may be normal, or related to post op phrenic nerve palsy (dissection during transplant surgery)… The linear shadow above diaphragm is most likely some form of linear atelectasis in this asymptomatic lady. Overlying right 7th posterior rib is surgically absent which may account for locally different ventilation.
I’m not thinking of pneumoperitoneum as I feel there is some lucency above liver below diaphragm related to abdominal fat contiguous with fat on right side of liver. Also post gastrostomy leaks usually present within 24-48 hours. I have seen delayed cases up to a week. After 1 month, track has matured.
I can see a tube projected over the upper abdomen with a discontinuity, its ends are not covered… Would like to compare with any prior post gastrostomy chest/abdomen radiograph to confirm if its intact and not fractured. The later is highly suspicious on this film
Esophageal fluid level is expected due to reflux esophagitis and stricturing in scleroderma related esophageal changes.
There is an air under right hem diaphragm, we can see air anterior and posterior to the area nuda. It is probably after PEG implantation or persistent leak of air. End of PEG is in duodenum. I don’t why there is small gap within the tube, but for me it is outside the body.
In posterior mediastinum there is a small buble air with fluid level – probably small gastric herniation. Right dome is higher due to phrenic nerve palsy.
I am looking forward unpatiently to your answer.
See my comment below
So far, nobody has mentioned the etiology of the pneumoperitoneum. Use the KISS method: air is coming either from ouside or from inside. Which is it?
I think the origin of this pneumoperitoneum is pneumatosis intestinalis.
Especially with a patient has a past history of lung transplant.
Pneumatosis cystoides intestinalis has ben reported after thoracic surgeries, when air travels through the mediastinum into the retroperitoneal space and then comes through the perivascular spaces in the intestinal wall.
The patient no symptomatic , its mean no dependent to her gastrostomy or perforation . But he is a SSc known case and there is a benign penumoperitoine that occure in Ssc after pnematisis cystoides intestinalis that show in this patuents in RUQ and central of abdomen in AP x ray…
Its benign
Pneumatosis cystoides intestinalis (PCI) is a rare gastrointestinal complication in scleroderma. I supposed the air in this case may be escaped around the gastrostomy catheter.
I think that air in peritoneum comes from outside. Because of mobile part of stomach it is imposible to keep stomach wall close to the abdominal wall, which is necessary to keep gastrostomy air – tight. The gap between these to walls causes persistent air leak around skin entrance of the tube.
To support this assumptions -gastric entrance of the tube seems to be quite high in the left upper abdomen. It would be very inconvenient for the patent to keep it Just below the ribs.
See you tomorrow Dear Muppet.
Yvette, Muppet’s heart bleeds for you!
See tomorrow’s answer.