Welcome back to your favourite corner! Starting with a warm-up case: pre-op radiograph prior to biopsy of a vocal cord nodule in a 57-year-old woman with hoarseness. Including a radiograph of the shoulder taken eight months earlier in which part of the left lung is seen.
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
1. Widespread adenocarcinoma
2. TB
3. Sarcoidosis
4. None of the above
Findings: PA chest radiograph shows widespread air space disease located mainly in the upper lungs. Comparing with the previous film, the disease has progressed moderately in the last months. In my opinion, the clue to the diagnosis lies in detecting cavitation, depicted as radiolucent areas in both apices (A-B, arrows).
The fact that the one in the left apex has not changed (A-B, red arrows), despite the progression of the disease, supports the presence of cavitation.
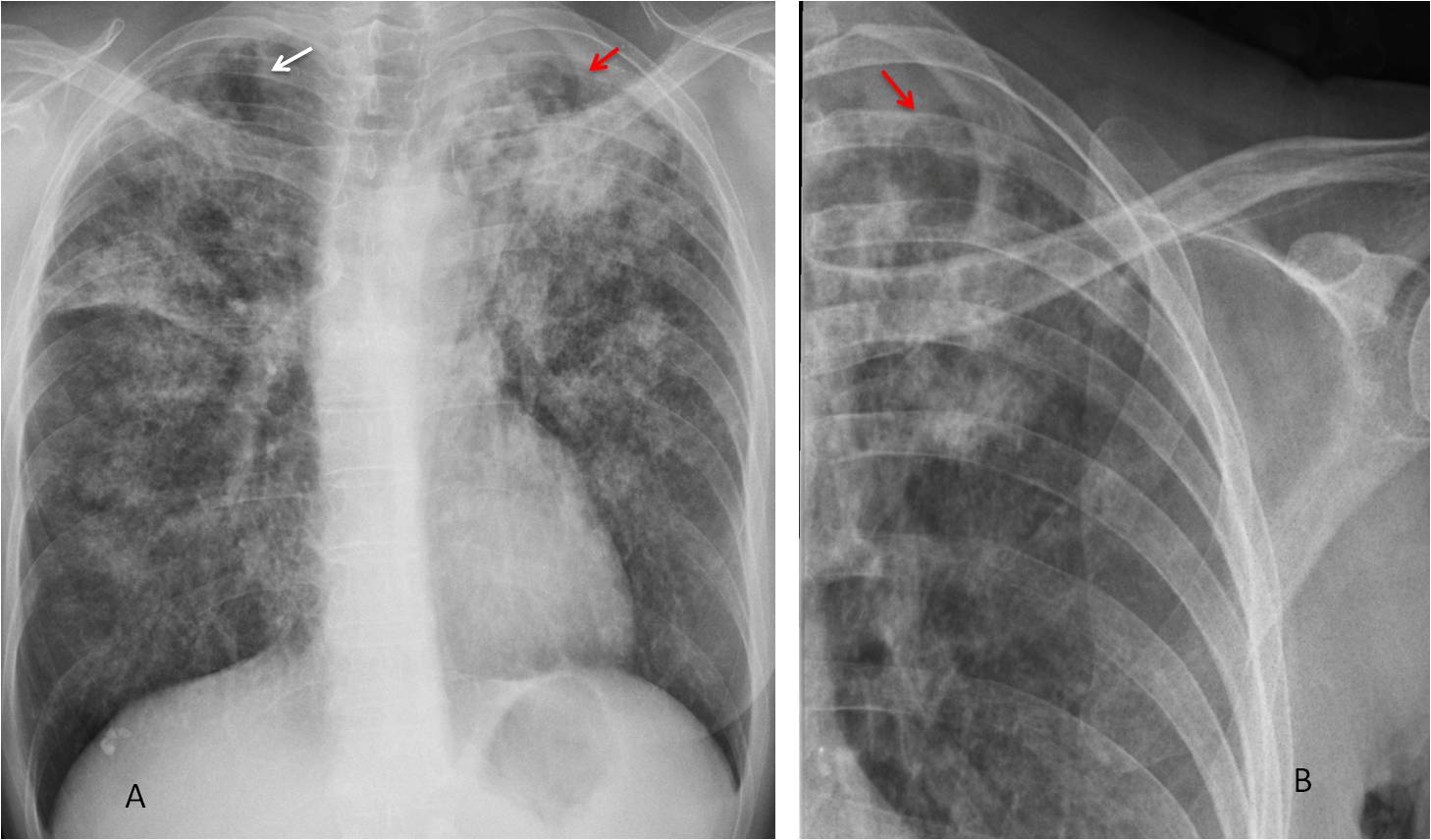
Fig. 1
Once cavitation is suspected, pulmonary TB is the diagnosis of choice, suggesting also that the nodule in the vocal cord may be a tuberculous granuloma. CT confirms the air space disease accompanied by cavities (Fig 2). BK was found in the sputum. Surgery was suspended. The pulmonary infiltrates and the lesion in the cord improved with treatment.
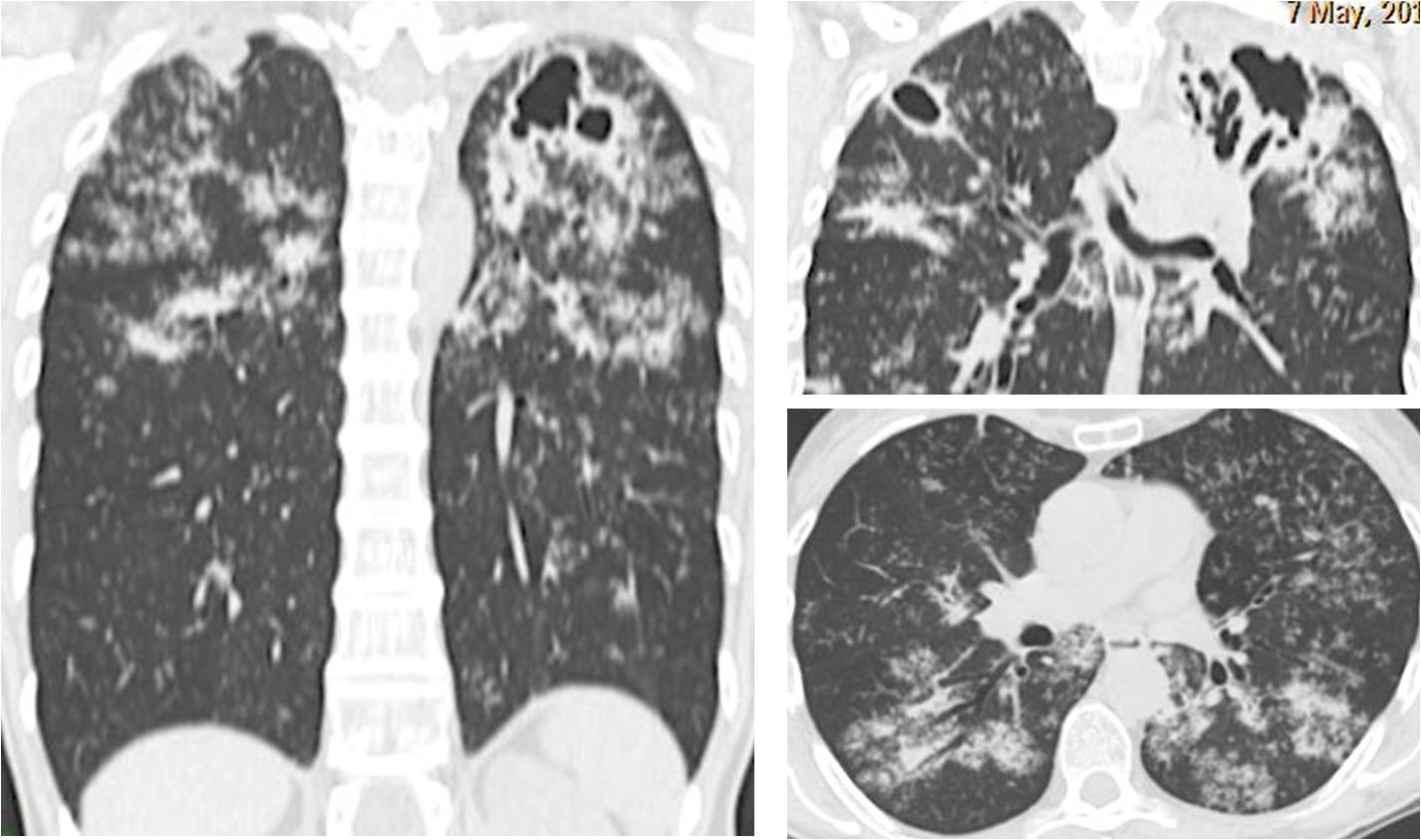
Fig. 2
Diagnosis: cavitated pulmonary TB with TB granuloma in vocal cord
Congratulations to Giovanni Battaglia, who was the first to suggest the right diagnosis.
This case emphasises several teaching points:
1. Paucisymptomatic TB is not rare, especially in middle class, well-nourished individuals.
2. Discovering cavitation is important to suspect TB
3. Remember the association of laryngeal disease with active pulmonary TB. I have seen several cases.




-Extensive bilateral reticulonodular opacities in conglomerated nodules pattern affecting mainly the upper lobes
-Elevated both hila and transverse fissure with displacement of trachea due to upper lobes fibrosis
-Erosion of left glenoid fossa and calcified hepatic nodule are seen
3- Sarcoidosis
Welcome back Professor
Hello after holiday:)
I choose sarcoidosis. There is bilateral and symetric massive reticulonodular opacification in both lungs – predominantly in upper and middle parts of lungs. In comparison with previous examination there is moderate progression of changes and new tiny calcification are seen in supraclavicular region – probably lymp nodes.
Becouse hilar or mediastinal nodes aren’t enlarge I suppose stage III of sarcoidosis.
I disclose TB – no cavitation in opacification.
I disclose adenocarcinoma – no alveolar opacification and hilar lymp nodes involment.
There is also bigger calcification in lower part of right lung behind diaphragm probably hamartoma.
Tubercolosi.
Hello Dear Professor!
I agree with Boruc. It could be sarcoidosis. But the same distribution ( upper lobe predominance of reticular patern) could be also present in silicosis or coal worker pneumoconiosis. This new opacification in upper left lobe could be progressive massive fibrosis, more often present in CWP.
Small opacities along the left clavicle seems to be connected with chest wall soft tissues.
Welcome back (Boruk included). Seems that sarcoidosis is by far the winner.
TB
TB and cariera sicca
There is progressive left apical pleural thickening besides the bilateral opacitication with loss of volume of upper lobes, mainly the left one. This would orientate towards an aspergilloma that could arise in a patient with TB or Sarcoid. If there is not Shortness of breast on exertion I would go for Sarcoid, If there is SOB I would think in TB. A Pancoast tumour would be a further possibility for progresssive apoical pleural thickening but the increase in opacitication over these 8 months is quick and more suggestive of an inflammatory process than a neoplastic one.
Summing up Aspergilloma + Sarcoid or TB ( more likely Sarcoid in absence of SOB)
Nice discussion. We sugested the diagnosis with no clinical information, other than the stated in the presentation.
You are a master
Thinking you leave and work where you leave I go for TB + aspergilloma
Flattery will take you nowhere!
woman with hoarseness we must think about recurrent laryngeal nerve.
The distribution of the findings is mainly on the upper and middle zones with fibrosis (lost of volume),nodular opacities and cavities with pleural thikening on apical caps (chronic tb)that is worse than prior film.
i think we must be careful could be a Ca with chronic tb background.
– CT!!!
Hoarseness can be explained by the nodule in the vocal cord.
..carissimo Professore, scusa il ritardo, ma avevo dimenticato l’inizio del nuovo appuntamento a settembre….sto invecchiando…..ti rispondo pertanto in ritardo…..come sempre un ragionamento clinico iniziale….rx-spalla 8 mesi prima e nodulo laringeo…..assemblando i 2 dati vediamo il peggioramento del quadro polmonare con un grosso infiltrato in sede sottoclaveare sx ed opacità reticolonodulari nel restante ambito…..con la solita “FANTASIA” che contraddistingue noi radiologi , io penserei a TBC polmonare da diffusione endobronchiale del focolaio laringeo….
…vince sempre l’ITALIA !!!!!
Tuberculosis
In the shoulder radiograph a subtle lucent lesion in the region of anatomical neck superolaterally.
within the chest, extensive reticulonodular opacities, predominantly in upper and mid zones, with volume loss in the right upper lobe.
At least two, thin walled cavities in the left upper lobe are seen in the chest radiograph.
A soft tissue density mass in the left upper lobe which has developed in the last 8 months.
left apical pleural thickening without any underlying bone destruction.
Numerous tiny, pinpoint calcific foci in the left supraclavicular region.
A lobulated small calcific focus in the right basal region, possibly a hamartoma.
findings are likely to represent widespread pulmonary tuberculosis with aspergilloma in the left upper zone and caries sicca.