Today we are showing a case that our good friend Carles Vilá showed us three weeks ago. Images belong to a 44-year-old woman admitted with renal colic. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
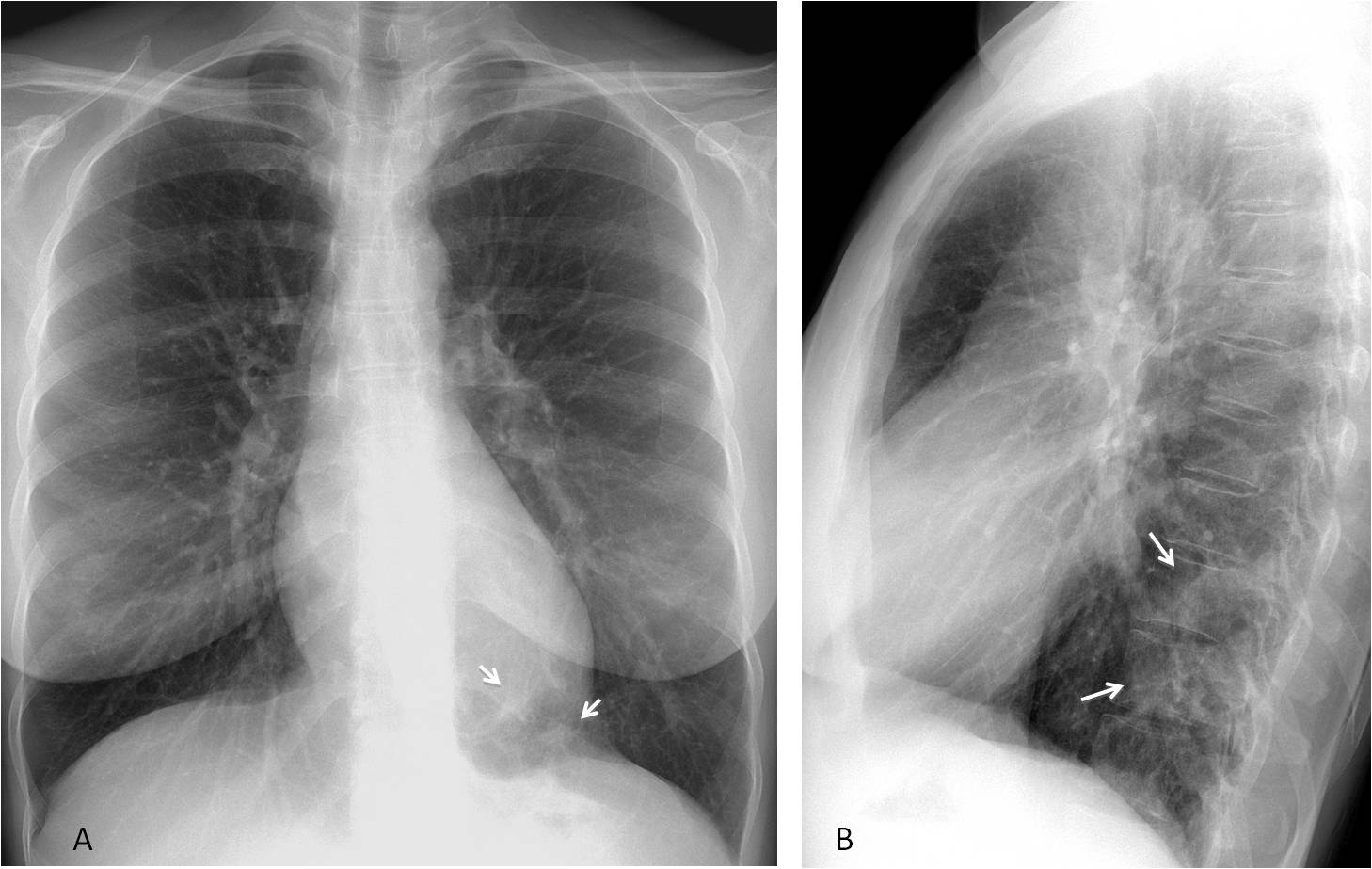
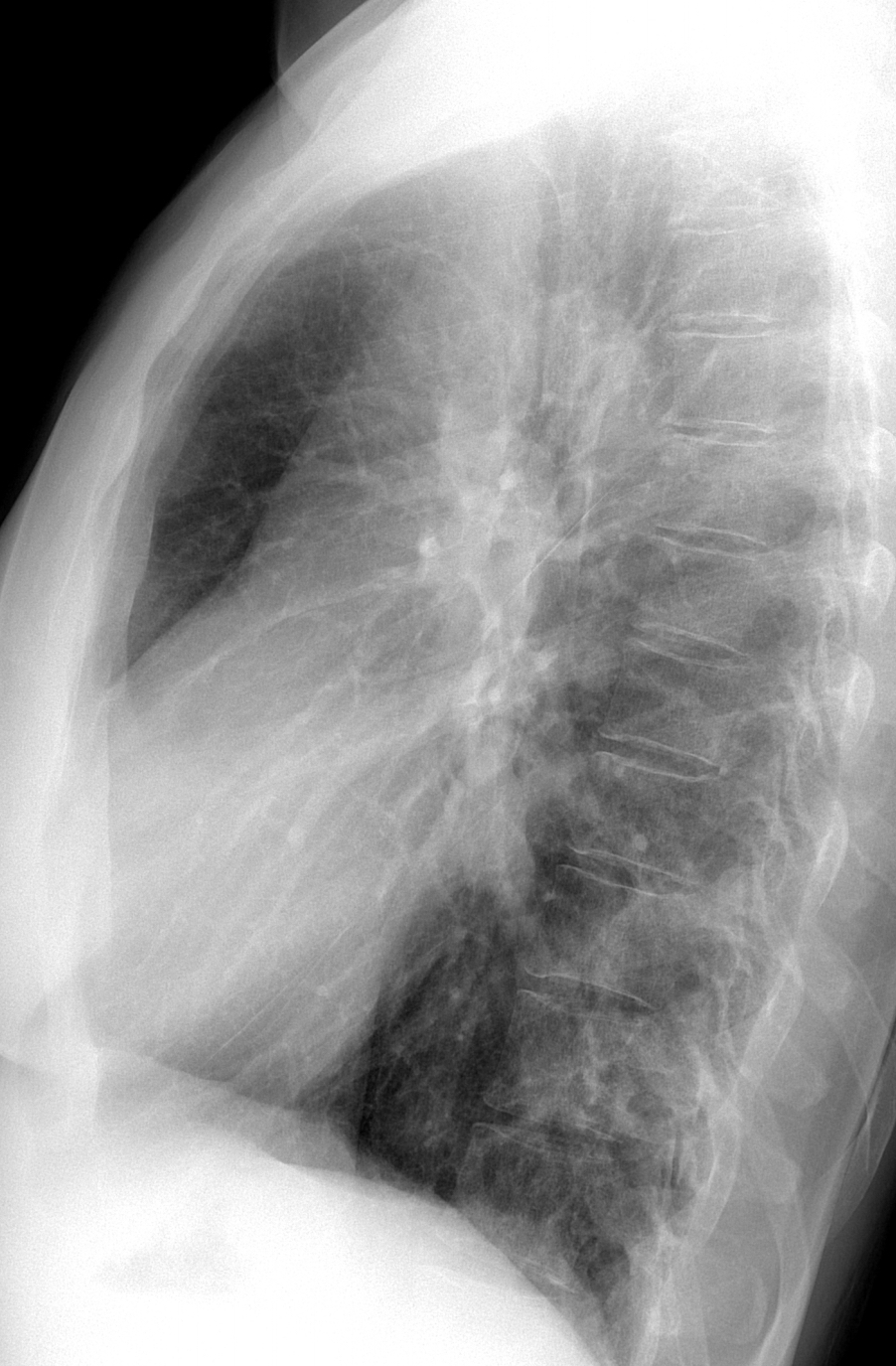
Findings: the lateral view shows an increased opacity at the level of the T10-T11 vertebral bodies (B, arrows), which is visible as ill-defined opacities at the left lung base in the PA view (A, arrows). They are not specific for diagnostic purposes.
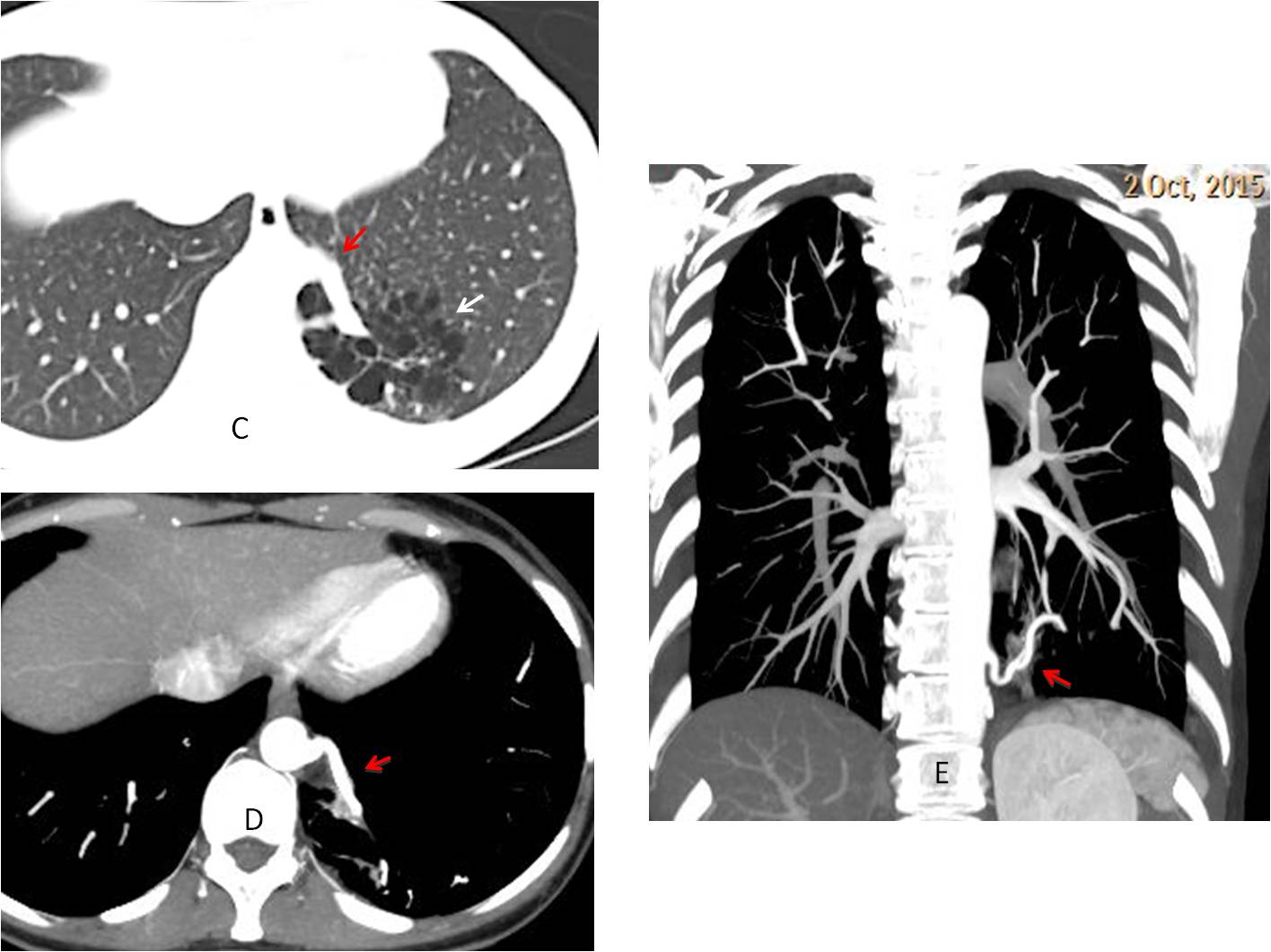
Unenhanced abdominal CT for the study of renal colic discovered a multicystic lesion in the left lung (C, arrow) with a possible abnormal vessel arising from the abdominal aorta (C, red arrow), confirmed with enhanced chest CT (D-E, red arrows).
When questioned, the patient denied any episode of previous pulmonary infection.
Final diagnosis: cystic sequestration of the lung
Congratulations to Ryan, who was the first to observe the abnormality
I am showing this case because it is a nice complement to case 121, in which the increased opacity of the vertebral bodies was due to spinal disease. In the present case, the opacity is also obvious and due to superimposed lung pathology.
Teaching point: Remember that congenital lesions are not rare in the adult and are seen more often than expected.



there is poorly defined opacity in retrocardiac area near the lower parts of the thoracic vertebrae. also in retrosternal clear space, there are perhaps 2 rounded peripheral lesion. maybe im looking too hard in the later. pneumonia?
I believe you are looking too hard at the retrosternal space. It looks normal to me.
1. Moderate pectus excavatum.
Very moderate…
opacity at the left superior mediastinum
vascular origin
Left-sided superior vena cava or partial anomalous venous return
lateral view : left dome of hemidiaphragm is blurred;
an opacity extending from lower part of the hila to the posterior clear space (it partially projects over the lower part of thoracic spine).
A trachea is poorly seen, maybe there is small ovall opacity near the infracarinal area (lymph node?)
PA view : an opacity projecting over the cardiac silhouette and the left dome of hemidiaphragm;
left hilum is situated higher than right.
2. I not see a gastric air buble . On the lateral view trachea is reduced in diameter -possible esophageal pathology ?
….LA colica renale è in reaLTà un dolore di” origine” ossea: alterazioni osteostrutturali di tipo litico sembrano evidenziarsi a carico di D10-D11
Do you think that the opacity may be in the lung?
il profilo cardiaco inferiore sx sembra dissociato dalla cupola diaframmatica….in ll a livello di D10-D11 sembra evidenziarsi una opacità il cui angolo superiore è ottuso, quindi extrapolmonare…..aspettiamo la TC
Waiting for the CT is a wise decision
…sede…infezioni respiratorie ricorrenti….sequestro polmonare….
3. May be. On the PA – in the 6 right intercostal space determine opacity, and the lateral view in front of the Th9-Th10 vertebrae.
3. May be. On the PA – in the 6 right intercostal space determine opacity, and the lateral view in front of the Th9-Th10 vertebrae.
sorry. I forgot to write that I do not agree with this comment
peribronchial and pericardium radiolucency
Clinically insignificant PAPVR ?
Close. But you need CT to make this diagnosis
lat view show suspicious lucencies in lower thoracic vertebral bodies, needs further assesment like CT chest
Ap . There are mulit nudollar opacity in both lung .
Lt hillar afenopathy was seen.Rt paratracheal erea isn’t Nl.
At latral view t9-t10 body isn’t clear….
Isn’t sarcoidosis?
Or TB?
I don’t believe it possible making the diagnosis in the plain film. What would you think if I say that the patient has recurrent infections?
pulmonary sequestration in the left lung base
Good! Better late than never…
double rt heart border ? left atrial enlargement