You may wonder what a foot is doing in a chest blog. The answer is obvious: because the foot belongs to a chest radiologist. These radiographs are of my own foot, where I noticed a painless swelling in the 4th right toe, present for about one year. Check the images below, leave me your thoughts and diagnosis in the comments, and come back on Friday for the answer.
Findings: AP and oblique views of the left foot show a lytic lesion affecting the distal joint of the fourth toe, extending into the distal and middle phalanges. The borders of the osseous lesions are sclerotic, indicating a slow-growing process (A-B, arrows). There is an accompanying soft-tissue mass (B, red arrow). The mass does not enhance after gadolinium injection in the MRI study.
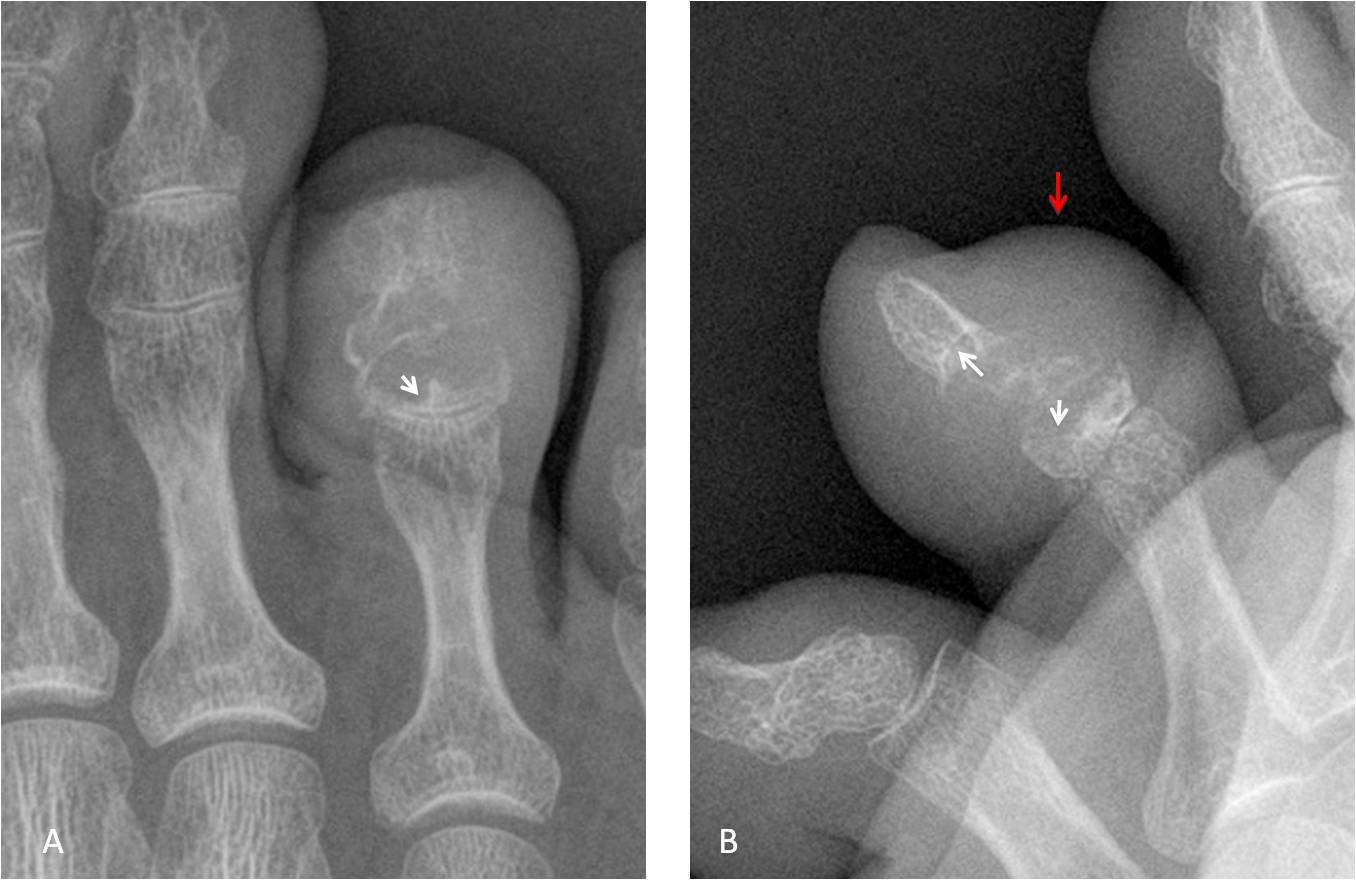
The plain film appearance of the lesion is typical of the so-called lumpy-bumpy arthritis. The differential diagnoses include: gout, sarcoidosis, pigmented villonodular synovitis and amyloid, among others. Percutaneous biopsy confirmed the presence of uric acid crystals.
Final diagnosis: tophaceous gout.
Congratulations to Aloria, who was the first to suggest the diagnosis.
Teaching point: I am showing this case to emphasise the importance of knowing basic semiology. In retrospect, the lesion is a textbook example of lumpy-bumpy arthritis, of which gout is the most common etiology. My colleagues and I were too scared to think clearly. On the other hand, I am proud to have the same disease as my mentor, Dr. Benjamin Felson.




….carissimo professore, quale onore averti come “paziente “….non può essere una sinovite villo-nodulare, perche’ essa interessa due superfici articolari contrapposte e colpisce sopratutto le grandi articolazioni( anca-ginocchio…), non può essere sinovioma perchè in quel punto non c’è sinovia…..non mi sembra un processo maligno come da condrosarcomsa…..sembrerebbe invece un encondroma……Complimenti al Barca….ha spezzettato in 4 il Real….anche il mio Bari vola…..
Intrasseous gout
And I am very sorry to see that, Professor!
Don’t worry, I will survive!
None of the above – gout
maybe 2?
Maybe
Solo Descripcion.
Lesión lítica, agresiva, transarticular, requiere mas estudios de imagen. Entre las posibilidades encomdroma? Sarcoma Sinovial? Artritis? RM correlación con la clínica.
Clínicamente la lesión era indolora. La RM mostró una masa de tejidos blandos, sin captación de contraste.
Maybe
….poche risposte……come il grande Barca, mitico professore hai messo paura a tutti …..chi ti “sfida” rischia la fine del Real o della Roma !!!!!!
Glad you like Barça. Probably, only Bayern can stop it.
Lytic lesion affecting the middle and distal phalanx of the fourth finger with cortical destruction and regional increase in soft tissues. The slow growth and the absence of pain for a long time suggest a benign or a low grade of malignancy lession. We have to take into account: radiographic features, age, the clinical presentation and the personal history. My first choice would be a giant cell tumor but the differential diagnosis is wide: synovial sarcoma, enchondroma, chondrosarcoma, etc. It is necessary to extend study by MRI and biopsy.
Good people deserve the best for what I want it to be a benign lesion, we need the professor in shape.
Thank you for your concern. Don’t worry: I am still in my prime!
Chondrosarcoma of low grade, chondromyxoid fibroma or enchondroma.
Lytic lesion, no periosteal reaction, sharp transition zone sugest benign character. Archs and rings shape and calcifications sugest chondro origin. MR in further diagnostic.
…una visione più attenta delle immagini fa notare una tumefazione concomitante delle parti molli…..nell’encondroma , questa tumefazione non è presente….dovremo allora pensare ad una lesione primitiva delle parti molli con secondaria azione litica sulla falange….sulla superficie dorsale della falange decorrono i tendini estensori con le le loro guaine….pertanto una lesione tendinea….sinovialoma….
This was one of my possible diagnosis