This week’s images belong to a 16-year-old boy with a cough and fever for the last two weeks.
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
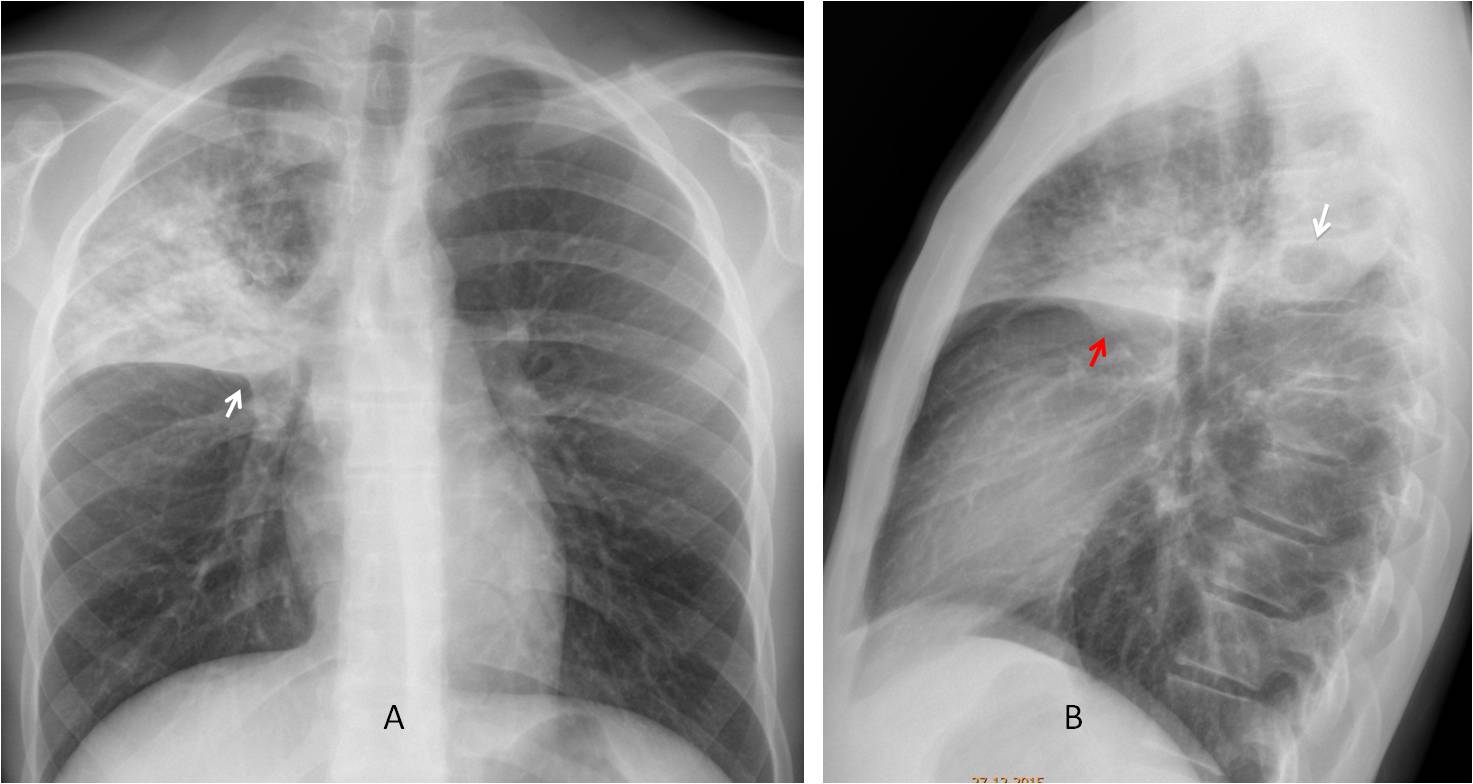
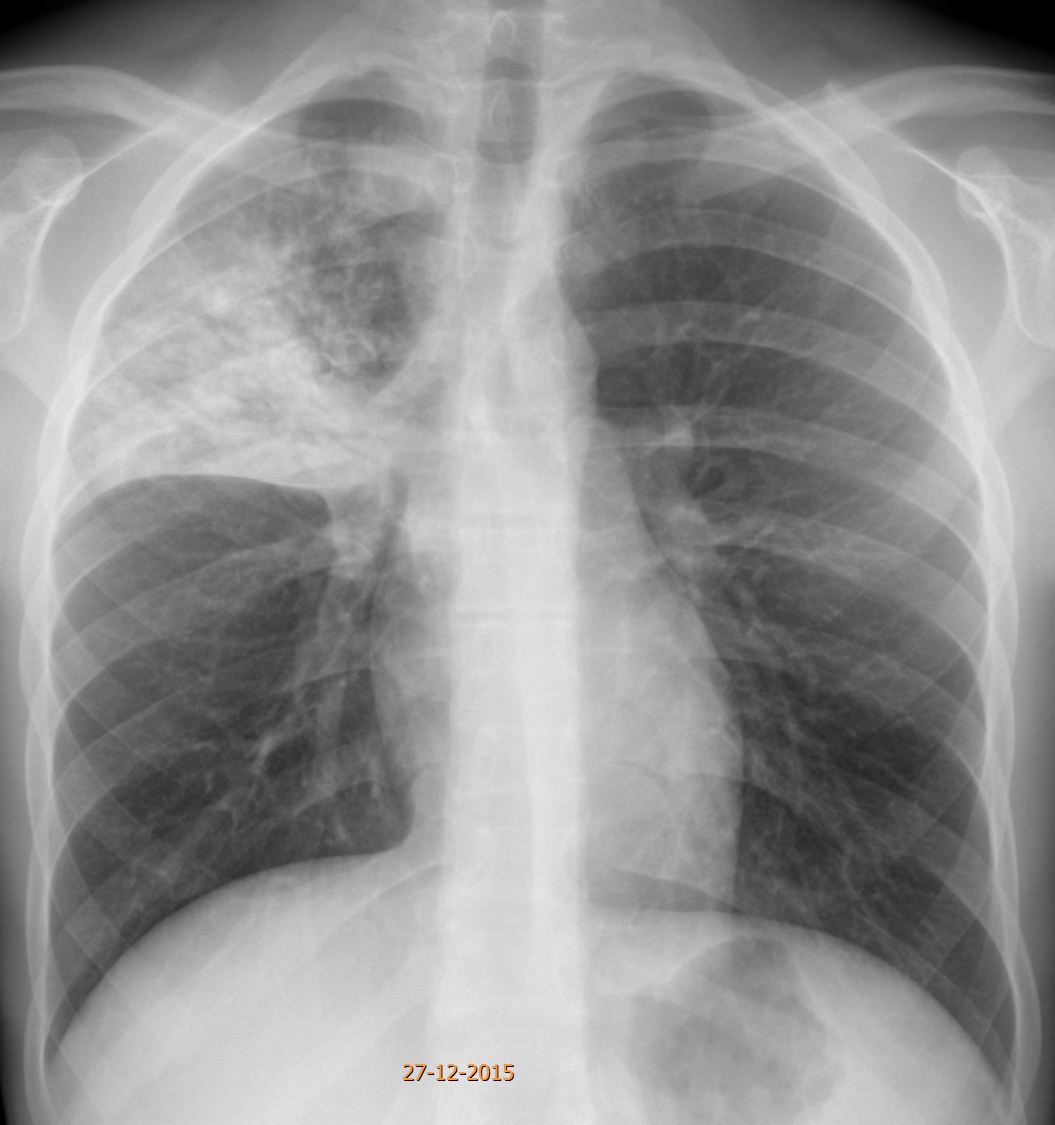
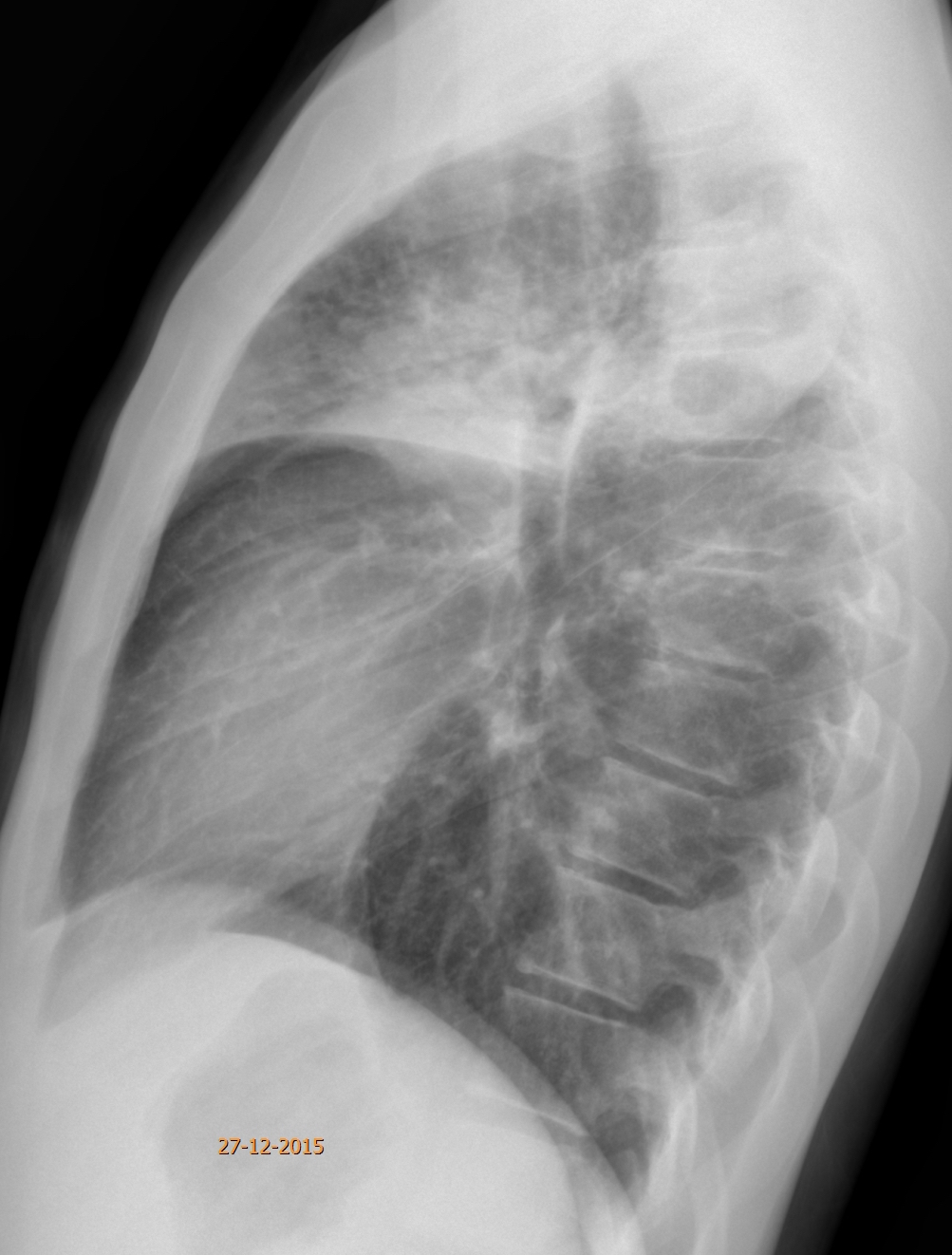
Findings: PA radiograph shows RUL disease with a suggestion on a Golden’s sign (A, arrow). There is an obvious cavity in the infiltrate in the lateral view (B, arrow). There is also a hint of a hilar mass or enlarged lymph nodes (B, red arrow).
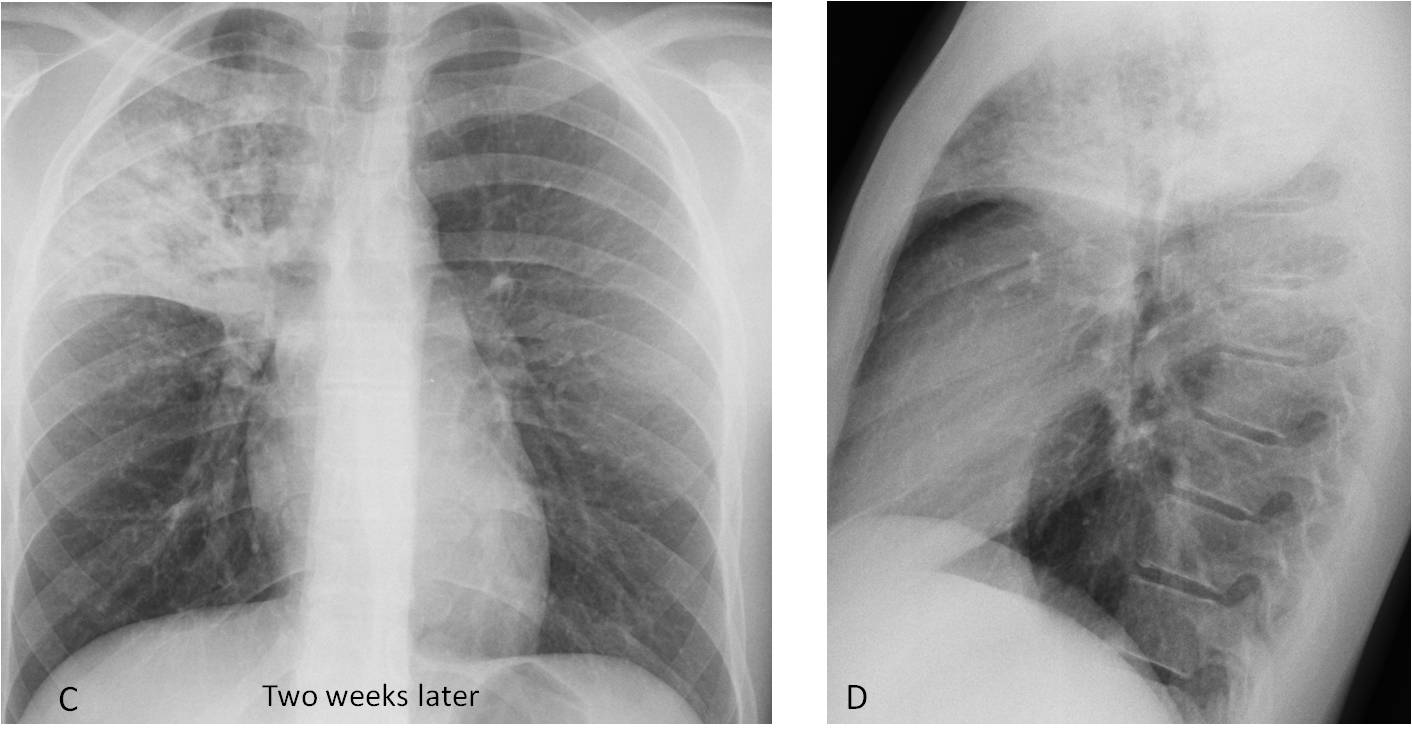
The patient was treated for pneumonia and two weeks later the appearance of the chest was practically unchanged (C-D).
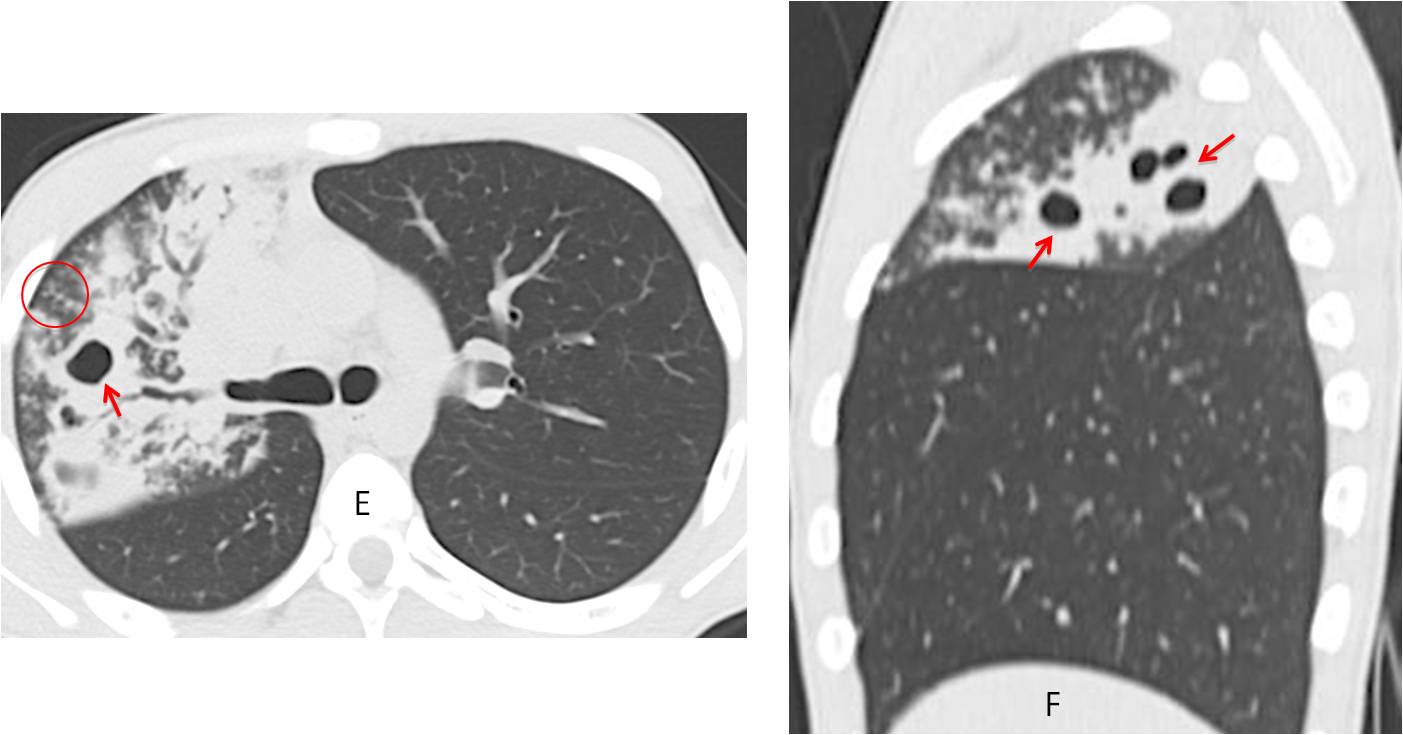
Axial and coronal CT show multiple cavities within the RUL infiltrate (E-F, red arrows), and areas of tree-in-bud in the periphery (E, circle). Sputum yielded abundant Mycobacterium tuberculosis bacilli.
Final diagnosis: Acute lobar TB
Congratulations to all of you who suspected TB, led by Leila, who was the first to mention the diagnosis
Teaching point: Always look at the lateral view. The cavity was missed in the first examination, delaying the diagnosis.


There is consolidation and nodules in the right upper lobe, and on lateral view cavity in the posterior segment of right upper lobe. I would think about tuberculosis.
Pneumonia
The first one. Welcome!
(Seeing too many ifs and buts so cant really decide!!)
There are infiltrates in the rt upper lobe.
There is also segmental consolidation (air bronchogram?) and collapse and Goldens S.
A cystic focus (better seen in lat view overlying vert) – no fluid level. ?Pneumatocele / ?cavity
Be a man! Decide!
Since too young for ca and too old for FB, TB should be excluded.
However, am not a man!
Any h/o weight loss?
Sorry about the mistaken identity.
No weight loss
RUL consolidation with a cavity at the posterior segment. Confluent acinar nodules at the margins of the consolidation. There’s a little of volume loss of RUL (horizontal fissure and right hilum dislocated superiorly).
I´d consider granulomatous infection (tuberculosis, fungal) and necrotizing bacterial infection as the main hypotheses.
right upper lobe pneumonia
right upper lobe patchy consolidation with air bronchogram obscuring right upper heart border with loss of volume ( elevated right hilum and transverse fissure ) .
there is increased inhomogeneous lung attenuation in right upper lobe, with well-defined lower margin due to horizontal fissure, mostly in hila and prehilar zone and less on the periphery, right apex is not involved (it is known as contra to tuberculosis), but there are shadows of multiple nodules seen through this lung consolidation and on the lateral view it seems that there are lung parenchyma destruction zone (in S2)
the right hila and trachea are shifted to the right because of mainly suggesting inflamation process but not atelectasis – there is no shift of horizontal fissure cranialy.
if suggesting this young patient have cough and fever the last two weeks, with such symptoms he should be healed as pneumonia, but with no positive progression, it looks like it is
2. tuberculosis
2. Tuberculosis
Lobar pneumonia, with small pneumatocele formation. TB is less likely; however interval follow up would be recommended after a course of empirical antibiotics; following which further evaluation for TB could be indicated, if there is no resolution.
TB without weight loss is very unlikely.
Am unsure whether I can see the Rt bronchus in the lateral view.
Along with Golden S, am leaning towards obstruction.
The pneumatocele/cavity is confusing.
…gentile Professore, ho aspettato a rispondere perchè con le tue opzioni diagnostiche mi hai messo” of-side”( il calcio è la mia pelle!)…come potrebbe una ragazza di 16 inalare un corpo estraneo? non è una bambina !…però una risposta stravagante ci sarebbe….abbiamo una opacità con perdita di volume, come indicato dalla risalita dell’ilo e della piccola scissura, indicativi per una sub-atelettasia, da corpo estraneo e magari broncopolmonite post-ostruttiva e piccolo pneumatocele…l’anamnesi cosa dice per eventuale inalazione, magari di un dente(estrazione), una nocella etc….
neumonia lobar derecha
picture goes with TB
consolidation with air bronchogram in posterior segment of rihgt upper lobe suggest TB