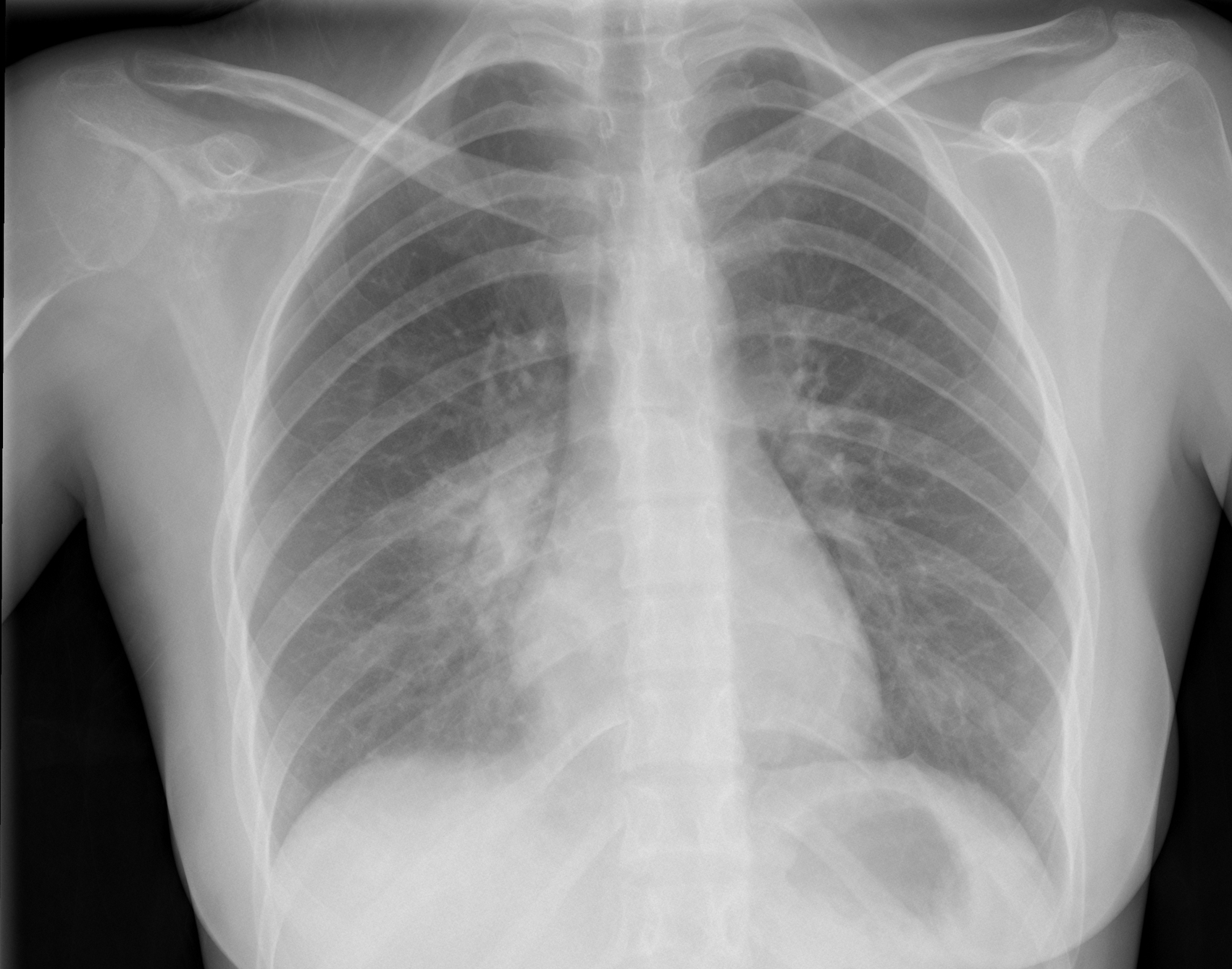
Today we are presenting a PA chest of a 28-year-old woman with fever and pain in the right hemithorax. What do you see? Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Findings: PA radiograph shows air-space disease around the right hilum and RLL (A, arrow). Given the age of the patient and the clinical symptoms, the most likely diagnosis is acute pneumonia. There is also loss of opacity and lack of visualisation of the outer cortex of the right humeral head (A, red arrow). These findings are more evident in the magnified view (B, red arrow) (compare with left shoulder, above).
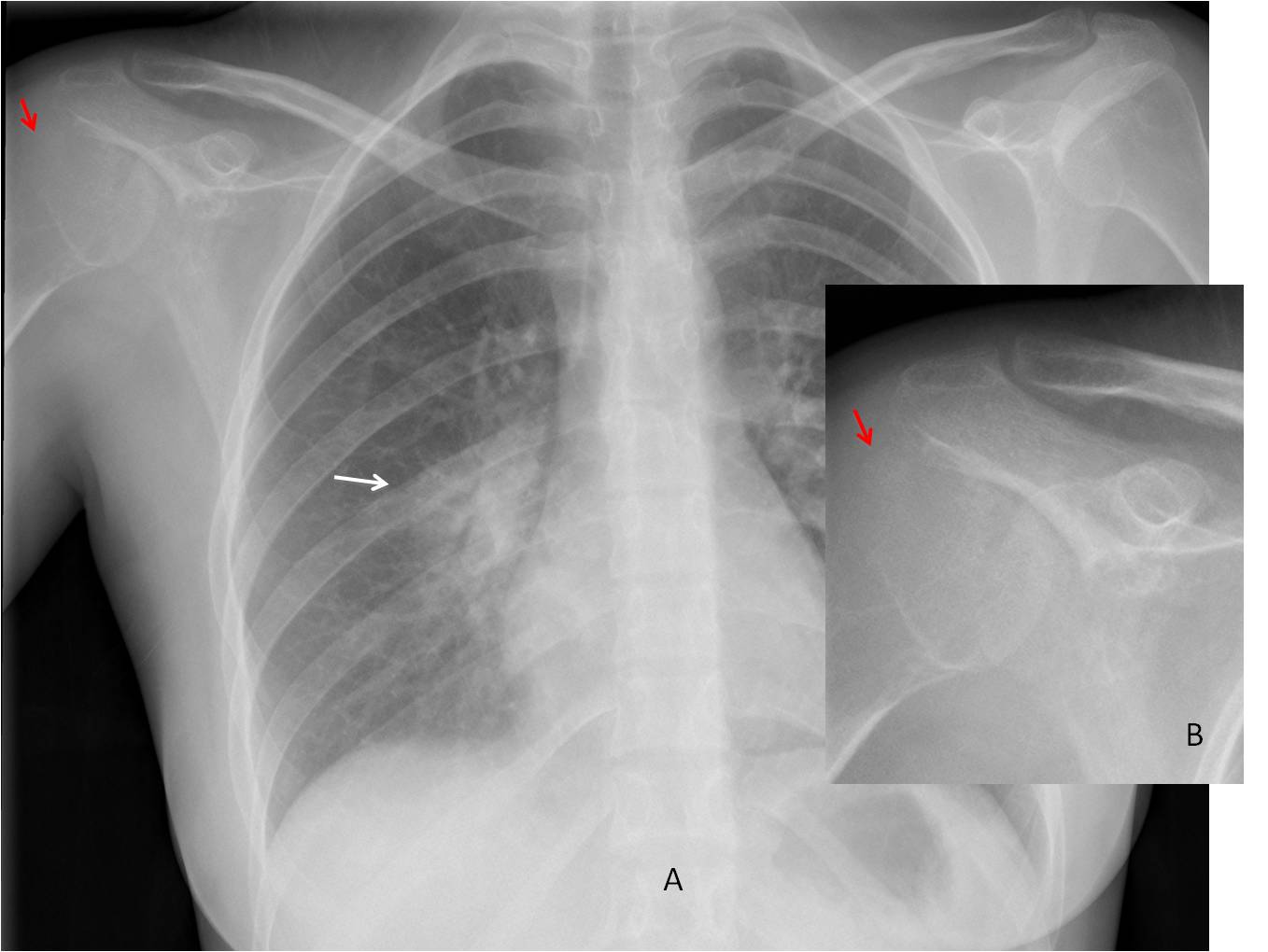
PA radiograph of the right shoulder shows a slightly expansive lytic lesion of the humeral head with numerous bone ridges inside (C, arrow). CT confirms the findings (D, arrow).
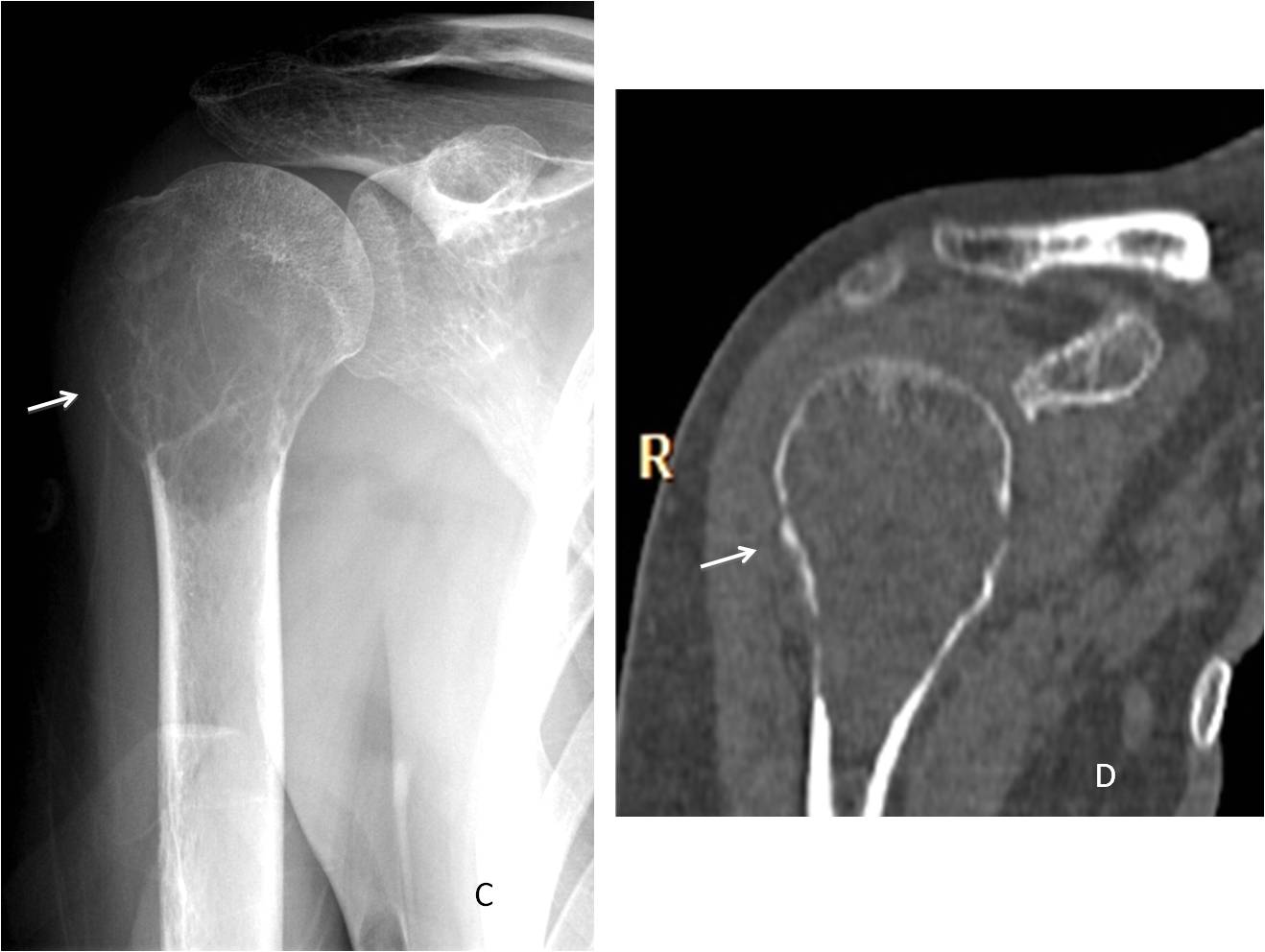
Diagnosis: Giant-cell tumour of humeral head
Congratulations to Murzin, who was the first to detect the humeral lesion.
Teaching point: remember to avoid satisfaction of search. It is important to look at the whole radiograph, because other pathologies may be found, as in this case


There are no evident changes in soft tissues.
In the right lung:
there is peribronchovascular infiltration in prehilar and hilar zones, with light shift of the right hila laterally;
there is inhomogeneous dicresed lung attenuation in paracardiac region abow the diafragm – infiltration probably in middle lobe (lateral view is needed);
cardio-diafragmal angle is shadowed because of pleural reaction;
on the shadow of right atrium it seems like there is a desrtuction – lateral view is needed
It seems lke there is destructive pneumonia of the right middle lobe, with probable pleural reaction
Hello,
There is prominent interstitial reticular changes near right hilum I suppose inflammation.
On the left are two artificial ring-like shadows projecting over lower lung and diaphragm – probably from outside body – I suggest repeat exam without clothes.
Don´t worry about the ring shadows
Rt lower lobe pneumonitis
Hello,
there’s an obvious perihilar infiltration on the right…
It seems to me that we can also see abnormal right glenohumeral joint- is it possible that the pain is localized laterally?
Yes, it is.
….sempre controcorrente…..a me sembra che ci siano delle alterazioni osteosclerotiche a carico dell’arco posteriore della 7 costa di dx…se così fosse l’ombreggiatura potrebbe essere di origine muscolo-cutanea per precedenti interventi chirurgici… BARI…un disastro!!!!!
.
Sorry about Bari.
Barça is playing very well.
…da rivedere l’articolazione scapolo-omerale dx !!!!! 9 punti sul Real sono tantissimi !!!
RIght lower lobe pneumonitis
right pericardiac pneumonic patch with prominent right hilar shadow
Les agradesco por su pagina y sobre todo los casos son de gran ayuda lo felicito y les mando sa ludos des de mexico
Gracias. Me alegro de que los casos le sean útiles
Patchy opacity rt perihilar region – consolidation.
Mild tracheal shift to the right.
Soft opacity rt paratracheal stripe – not sure whether extending across the midline to the left, but aortic knuckle clearly visible.
Punctate opacities rt hilum – ?vs/?calcifications.
A Rt shoulder AP required.
Hello! The lungs are well aerated showing a heterogenous confluence of opacities with apparent few air bronchograms at the area of the right hilum. This may represent consolidation possibly in the superior segment of the right lower lobe. The rest of the lungs are clear. Heart is not enlarged. Great vessels are within normal limits. Diaphragm and sulci are intact. Visualized Ossetia structures are preserved. I suggest lateral view of the chest for better evaluation.
Pulmonary (right perihilar region) and extrapulmonary (right humeral head) TBC?
It is not TBC, but you offered a nice diagnosis
Let me suppose, osteitis of the glenohumeral joint and humeral head in the right, complicated with septic pneumonia.
Thanks for each case, dear teacher .
I believe that the point of this case is detecting the shoulder abnormality. Further evaluation should be done with specific views of the shoulder.
Well done!