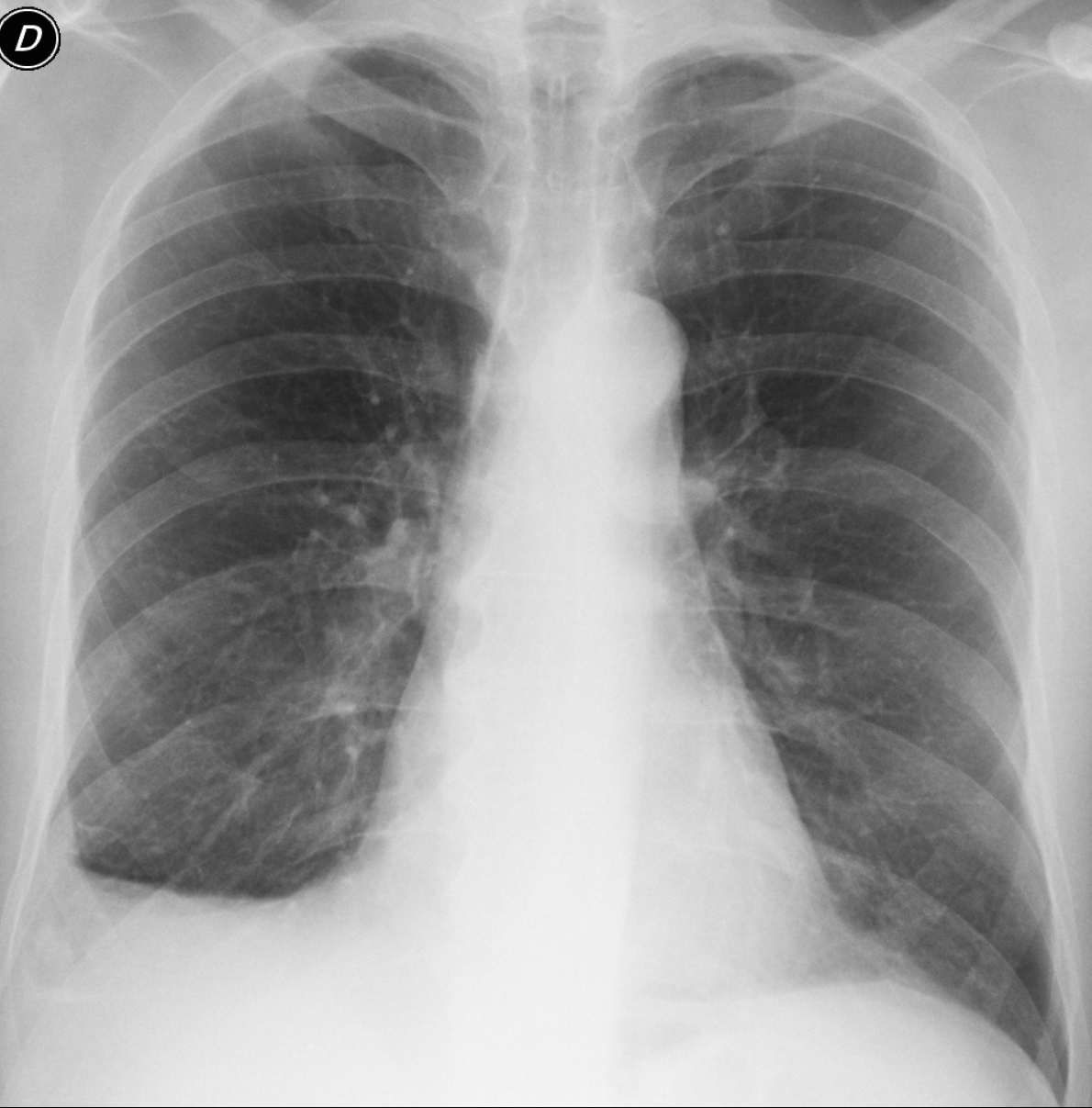
Today I am presenting the third case of the “five easy pieces”. Images belong to a 63-year-old man operated on for carcinoma of the colon five years ago. Previous annual CTs were read as normal. What do you see?
Check out the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Findings: the most important finding is a small pulmonary nodule seen in the lateral view (B, red arrow) and barely visible in the PA (A, red arrow). Considering that the patient has a primary tumour, metastases should be suspected. There is also obvious blunting of the right costophrenic angle (A, arrow), which looks like scarring because of the straight diaphragm and the absence of blunting on the posterior sulcus (B, arrow).
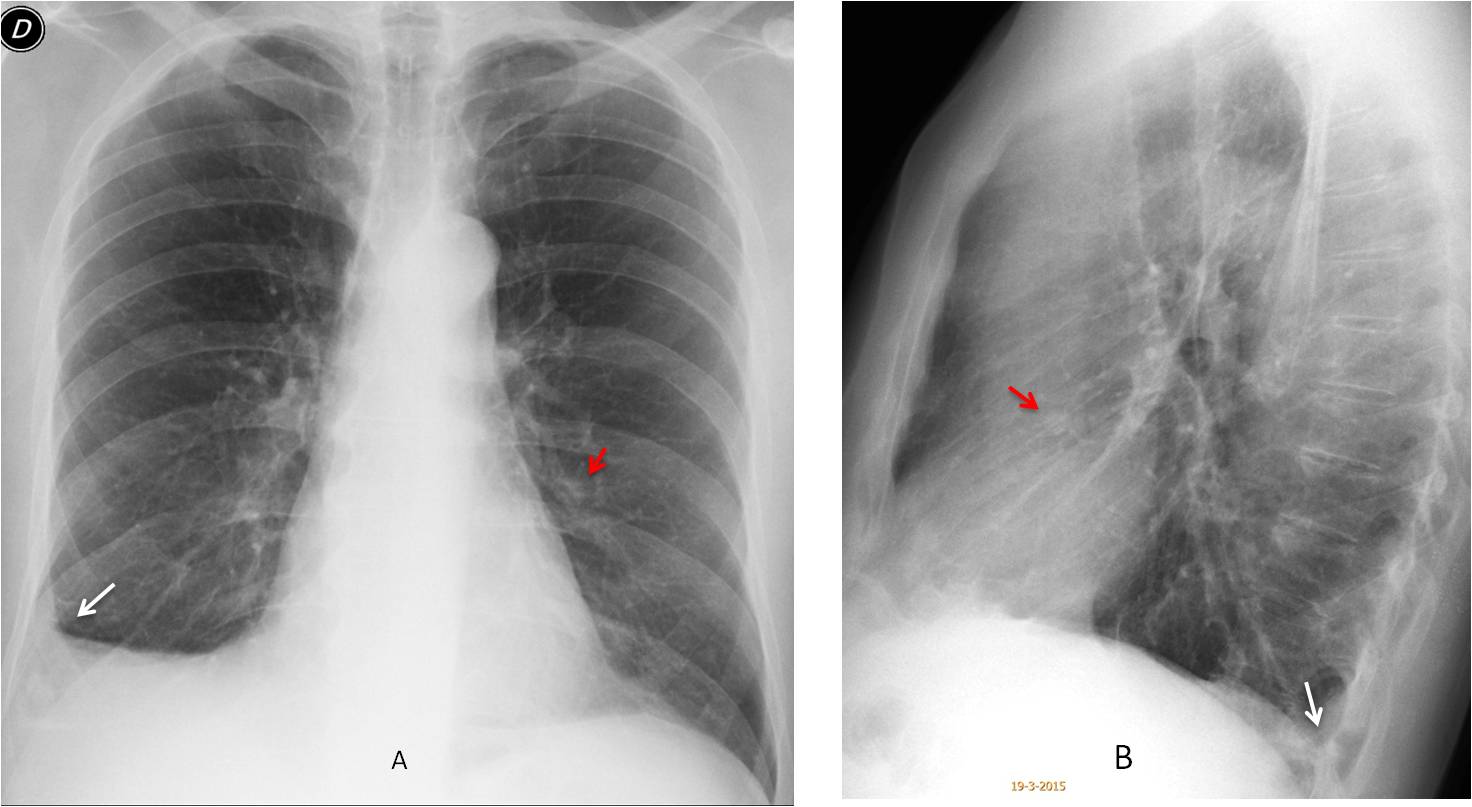
Axial CT confirms the presence of the nodule (C, arrow). Free fluid was not present. Review of previous studies shows that the nodule was overlooked in previous CTs, taken in 2014 and 2010 (D-E, arrows). Surgery confirmed metastases.
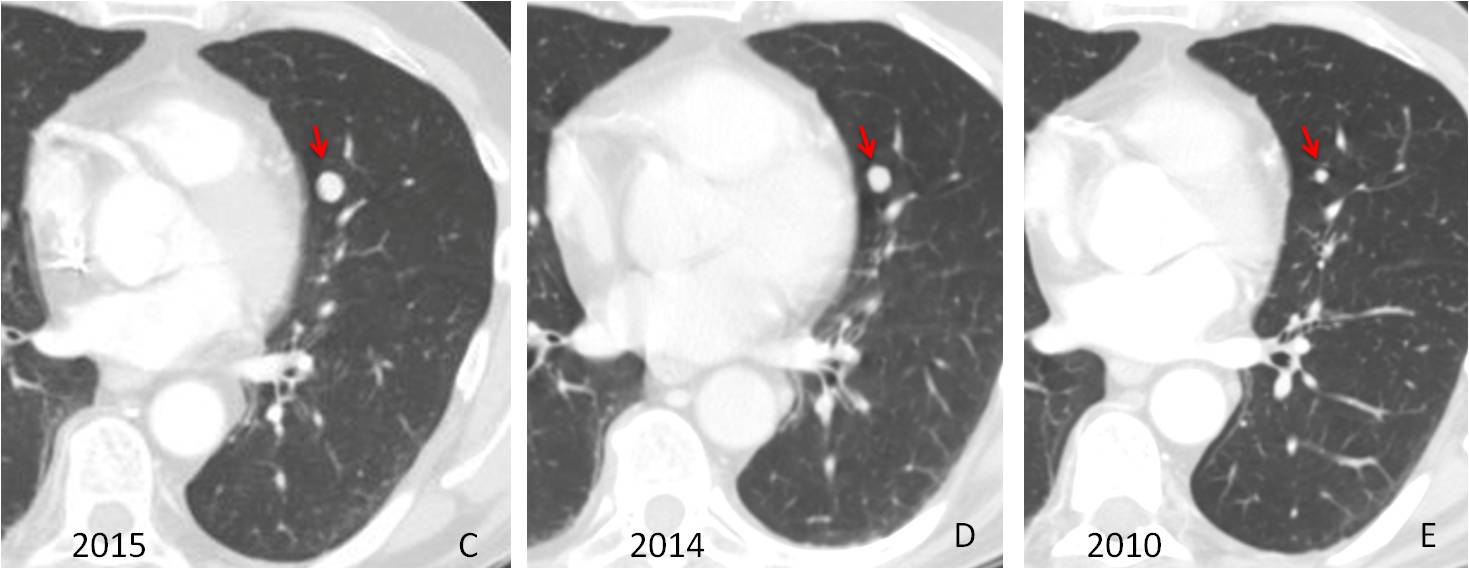
Final diagnosis: solitary metastases, overlooked at previous CTs and discovered in the chest radiograph.
Congratulations to all of you who saw the metastases, led by Olena, who was the first to make the diagnosis.
Teaching point: this case is a demonstration of the value of the lateral film, demonstrating a metastatic nodule that was overlooked at CT.



There is homogeneous shadow of pleura thickening on the right which is mostly on the anterior part of thorax wall and also in the middle part above of diaphragm in great fissure, suggesting pleural effusion (on lateral view).
On PA on the level of VI intercostal space there is a round nodular opacity, the similar nodular opacity is seen on lateral view on the level of heart shadow mostly anteriorly in lingula.
Regarding to anamnesis of carcinoma of the colon five years ago DDx is needed – nodulal mts with mts pleural effusion
Besides, pulmonary structure shows increased and intenceed due to peribronchovascular infiltration mostly in right lung and there is suggestion of multiple micro nodules on the right on the level of IV – VI ribs
I agree with Olen only adding pleural apical thickening of the lung and some nodular ill-defined opacities in the anterior recessus. DDg secondary meta lesion.
“apical thickening of the lung” – where? left ? right?
because I thought about one on the left but was not sure – it seems like it is sum of shadows
yes, and I agree about multiple nodular opacities anteriorly – I do not detailed
but where is that pleural apical thickening of the lung on lateral view? on the anterior part of superior mediastinum? close to sternum?
I believe the apical thickening is minimal. It is not seen in the lateral view, usually
Opacity in the upper field of the left lung?
Hello,
on ap it looks like pleural effusion on the right but on lateral view there istn’t any fluid in posterior right costophrenic angle. I suppose opacity on ap view is caused by change in pleura (as mentioned pleural thickening) or chest wall. Taking into account previous colonic carcinoma pleural mets is most probable diagnosis.
Hello
Suspected thickness of right cotiophrinic angle du to pleural effusion.
There are metastases in the upper lobe of the left lung, and hilar lymph nodes. There is more rounded opacities in the middle lobe (mets). Right frontal sinus obliterated, it can not be excluded encysted fluid.
Right pleural effusion. I feel like in lateral film the anterior mediastinal space is obliterated. on PA film the heart doesnt look that enlarge to me.
….grande maestro….la clinica…..storia di CR colico 5 anni prima…..versamento pleurico unilaterale con ombra cardiaca nella norma….piccola opacità nodulare in LL contro l’ombra cardiaca… sospetto di opacità nodulare pleurica alla base posteriormente…..l’ipotesi è versamento da metastasizzazione pleurica…conferma diagnostica , oltre che con l’esame citologico del versamento,….con la PET-TC ….Il Bari supera la crisi e viene acquistato da un Tycoon Malese…..diventeremo grandi….tifo blaugrana stasera….
Great game today! Hope Barça will pass.
The appearance of the pleura suggests scarring, supported by the normal costophrenic sinus in the lateral view.
Right sided pleural effusion along with a metastatic radioopaque density/module in right mid mum zone
Right sided pleural thickening/effusion with multiple nodules seen through it both in PA and lateral.
Another nodule seen in lateral view overlying the heart/ ascending aorta.
Is there any erosion with soft tissue opacity in the posterior elements of the last visible thoracic vertebra?
No vertebral problems. There is only one nodule, well seen in he lateral view.
Regarding the pleura, see answer to Genchi Bari above.
Rt sided pleural effusion and diffuse pleural thickning with lung nodule…metes?
Right sided pleural thickening/effusion with multiple nodules seen through it both in PA and lateral.
Another nodule seen in lateral view overlying the heart/ ascending aorta.
Is there any erosion with soft tissue opacity in the posterior elements of the last visible thoracic vertebra?
No vertebral erosion. Digital films give funy images in that area sometimes
Right lower lobe collapse due to endobronchal metastasis. Another nodular shadow is seen on lateral image.
Normal position of the right hilum is against lobar collapse
I can see multiple scattered fine nodules of tree in bud appearance at both lung fields.
There is opacity of the right lower lung zone sillhuotting the diaphragm, at the lateral view there is associated cystic like dilatation of the right lung base.
Picture may suggest fine pulmonary nodular metastases with suspected right basal pleural nodular thickening and underlying lung tissue changes.
An opacity is seen through the right effusion in PA and multiple round structures are present at the anteroinferior aspect on lateral.
If they are not mets then ?cystic bronchiectasis.