This is the fourth case of the “five easy pieces”. Pre-op chest radiograph for lumbar hernia of a 54-year-old woman.
What do you see? Check the image below, leave your thoughts in the comments section and come back on Friday for the answer.
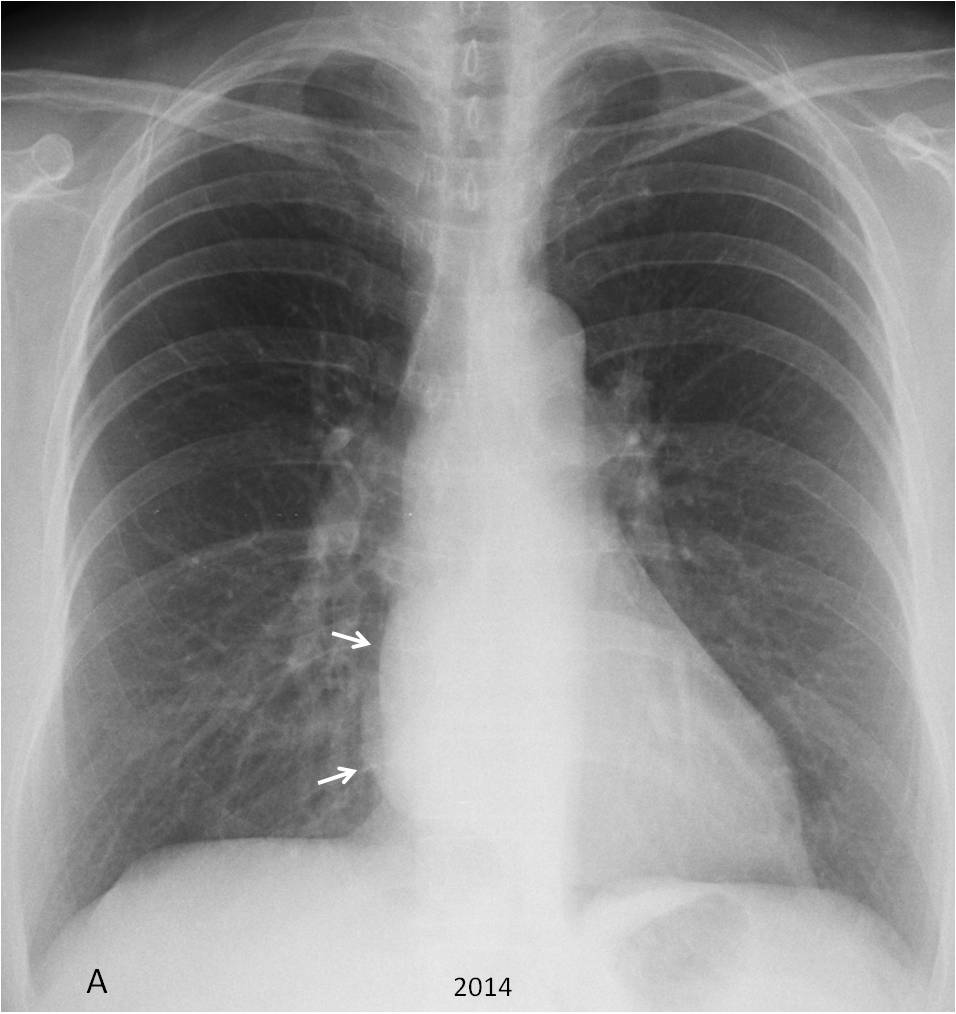
Findings: PA chest taken in 2014 shows a double contour of the right heart border (A, arrows), which suggests a retro cardiac mass, either in the middle or posterior mediastinum.
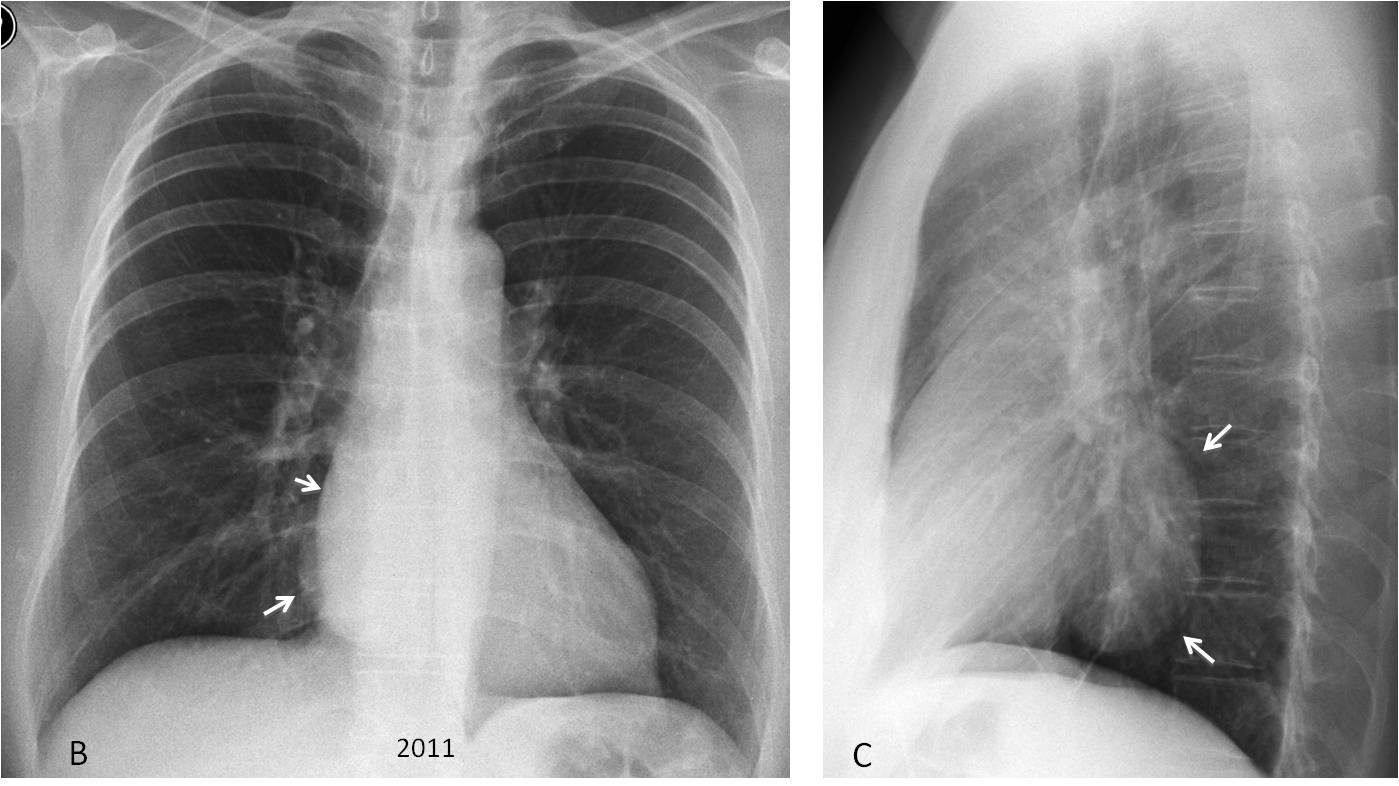
Review of previous films taken in 2011 confirms identical findings in the PA view (B, arrows), which in the lateral view correspond to an ovoid middle mediastinal mass (C, arrows).
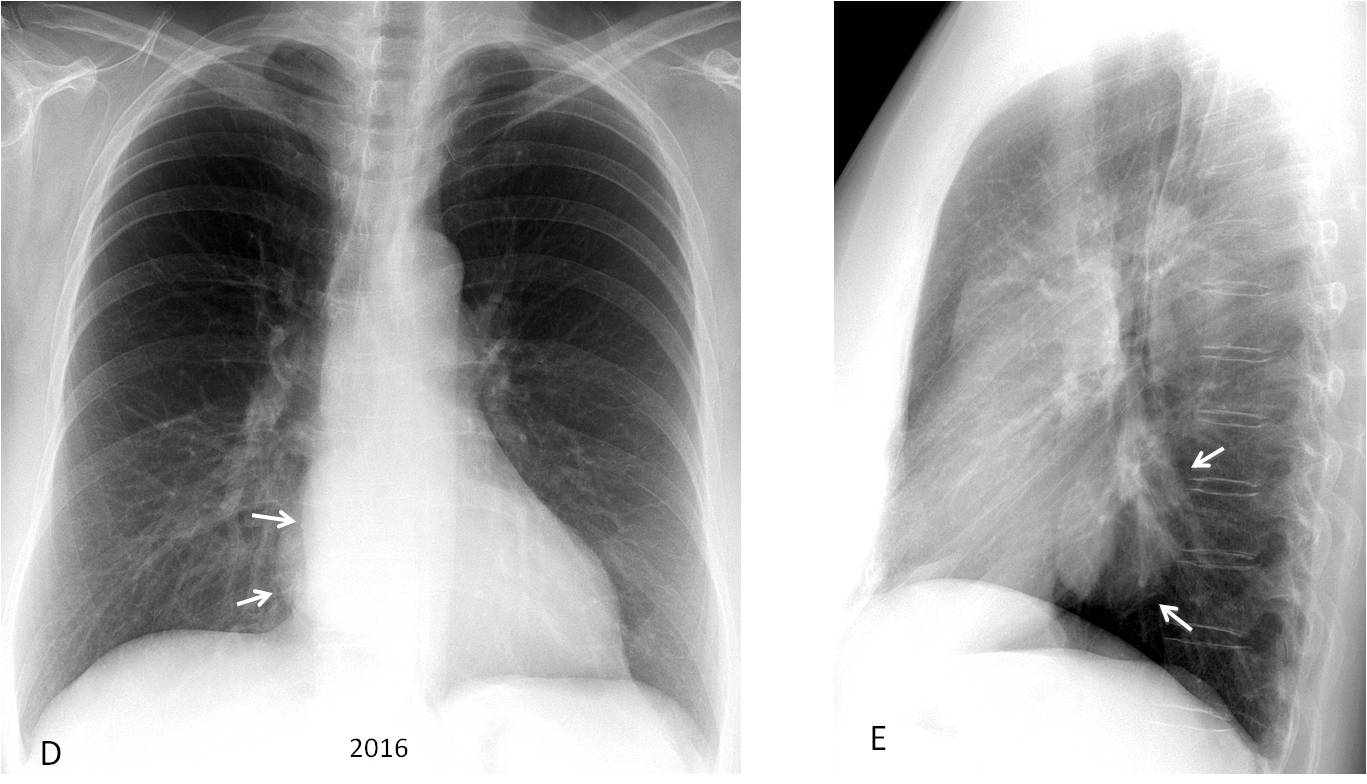
A recent study from 2016 shows that the mass is unchanged ((D-E, arrows). Because of this lack of change, a CT was not done.
Final diagnosis: probable mediastinal duplication cyst (unproven).
Congratulations to Eugeny, who was the first to notice the abnormality, unlike the radiologist who saw the chest in 2014 and read it as normal.
Teaching point: this case emphasises the importance of taking a lateral view. And looking at previous films, that in this patient were available in the PACs station.



Right paraspinal well-defined density in the retrocardiac region (neuroma?)
Round soft opacity overlying right heart.
Hello,
right well circumscribed density projecting over heart. Vascular or spinal origin could be suspect. Lateral viev needed.
Right paravertebral mass, DD include :neurogenic tumor,extra medullary hematopoisis
….il Professore vuole sottolineare l’importanza della LL nell’Rx torace, nonchè quelle delle linee paraspinali in AP….venerdì sapremo la probabile natura della massa….il Bari in netta ripresa e vede la serie A…..forza BARCA, supererete il momento nero….
Even more important, checking with previous films, where the abnormality was obvious!
The radiologist read the film as normal because he didn’t ask for a lateral, did not look properly at the PA and did not look at previous studies, which was available in the PACs
Força Barça and forza Bari!
Calcified proximal end of rib .
Chest clear no any leation detected.
Calcified of proximal end of rib to
Vertebra .
Chest clear
on the right is determined by the contour of the heart shadow with a rounded contour is possible pulmonary (neuroma?).
Homogenous well diefined opacity behind right heart border with blunt right cardiophrenic angle. There is some crowding of blood vessels on the right lower hila. Also there is sligh increase of transparency of right midle and upper lobes. Could be right lower lobe atelectasis.
The opacity is convex and the hilum is not descended. I think that these findings go against RLL atelectasis
They do, you are right. Stil, additional studies are necessary.
Convex opacity projected behind right heart atrium – posterior mediasitnal mass. My first opinion is focal dilated esophagus -suspect esophageal diverticula.
The algorithm as always is lateral view then esophagogram.
sorry, middle mediastinal mass.
There is widening of the inferior azygoesophageal recess and right paravertebral line. These included differential of middle or posterior mediastinal masses, its silhouetting the right cardiac border, likely middle mediastinal included DDx: hiatus hernia, oesophageal duplication cysts, malignancy or lymphadenopathy
Increased luceny right mid and upper zones with reduced vessel density. May reflect air trapping. Should be a chronic finding. Can’t see any definite signs to suggest atresia, mucus plugging or other structural cause for air trapping.
Eosophageal mass or aortic aneurism
obliteration right paravertebral line likely due to posterior mediastinal lesion mostly neurogenic cyst or duplication or neurofibroma.