Presenting the last case of “five easy pieces”. Images belong to a 58-year-old woman operated on for carcinoma of the rectum four months ago. She is admitted to the hospital complaining of moderate fever and abdominal pain.
What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
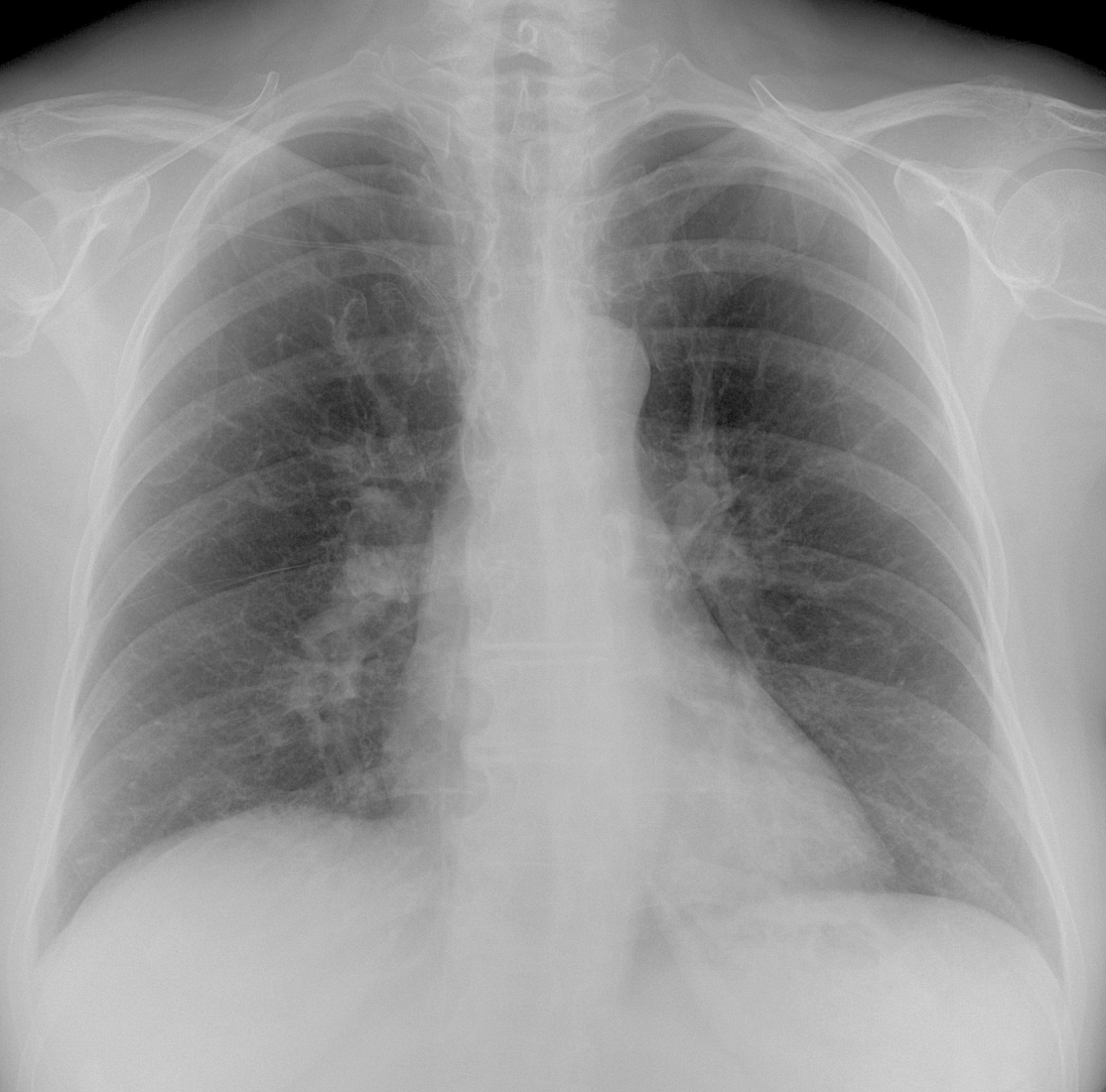
Findings: in my opinion, the pre-op chest radiographs do not show any intrinsic abnormalities. The main finding is an abnormal path of the central venous line (CVL), which goes deep into the abdomen (A-B, arrows).
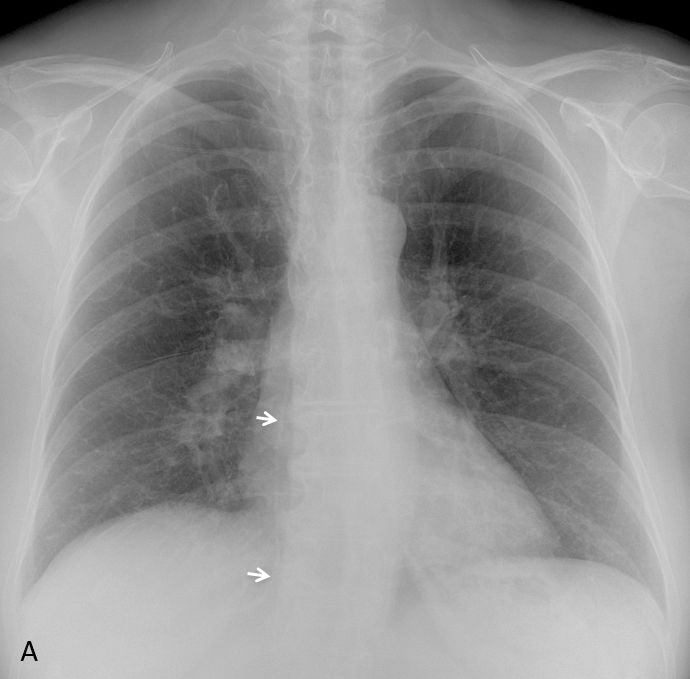

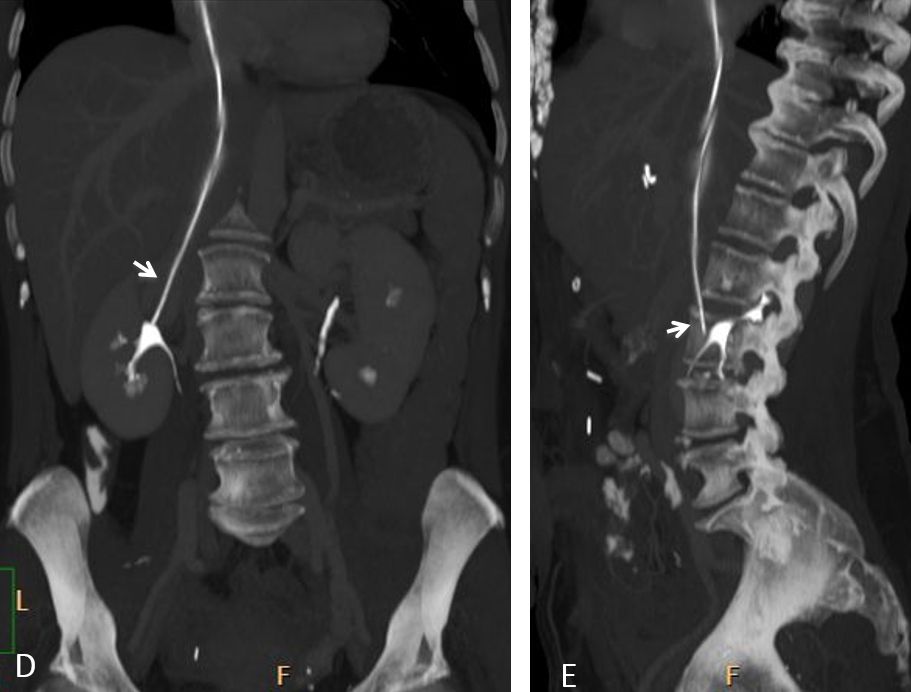
CT scout view shows the CVL in the right side of the abdomen (C, arrow). Coronal and sagittal reconstructions confirm the end of the CVL into the right renal vein (D-E, arrows). The catheter was removed and no complications ensued. The patient’s initial symptoms were caused by a pelvic abscess (not shown) successfully drained.

Final diagnosis: Malposition of the CVL into the right renal vein.
Congratulations to all who saw the abnormality, led by M A Fahmy who was first to mention it.
Teaching point: as I have said before, diagnosing malposition of a catheter is not very glamorous, but it can avoid significant complications to the patient (see Diploma cases 67 and 88).



There is a healed fracture of left clavicle.
There is a line is seen extending from the right side through the subclavian vein to SVC, right atrium, IVC to the abdominal cavity ? malpositioning therapeutic line.
there is an oval opacity is seen at the lateral X ray just anterior to the bifurcation of the trachea ? enlarged lymph node.
This patient likely has hilar lymphadenopathy (lymphoma) & under chemotherapy.
I think that the oval opacity is related to the pulmonary artery. CT was normal.
Right hiler nodal lesion.
Frontal view:
Following airways – trachea and left main bronch look normal, is there widening of right main bronch?
Aorta contour is normal
Both lungs are applied to the chest wall on all sides, there are some higher areated zones – symmetrically on the level of 1-2 ribs
But the linear shadow of the minor fissure is shifted caudally – the decreased volume of right middle lobe? inferior lobe? On lateral view the major fissure is shifted dorsally – decreased volume of left inferior lobe
Consolidated fracture of medial part of left clavicula
Both hila: there is evidence of venous stasis – the increased vessel shadows in hilar and prehilar zones and decreased vessel architectonic on the periphery, mostly in the right side. That is why on lateral view the pulmonary arteries could mimic enlarged lymphatic nodules
Cardiac: smooth mediastinal contours and normal shape
Right hemidiaphragms is shifted cranially (the increased size of hepar?)
Soft tissues show no pathology
On the right – the shadow of catheter in vena subclavia to SVC to IVC
On latereal view – on the level of sternum – high density shadows – suggesting calcified cartilaginous part of ribs ? were any surgical manipulations on the heart?
There are high intensive shadows on the level of abdomen – metal clips ? probable cholecystectomy (anamnesis)?
Malposition of central venous catheter
I agree with M. A. Fahmy.
1. Old fracture left clavicle.
2. Line on the right passing right through right heart into abdomen.
3. Round hilar opacity – LN.
4. Degenerative changes spine. Sternocostal cartilage calcification.
In my opinion, the right hilum looks normal
anterior aspect of the second rib on the left is different than on the right.Slightly increased lucency in the first intercostal space on the left side.
Maybe I’m wrong but I think there is metastasis of the anterior part of the 3 right rib. Bone scan is required.
The distal end of central venous catheter below the diaphragm level acceptable.
I image you mean not acceptable
Oops! Misprint. Course it is not acceptable
Features of Cholecystectomy.
PICC line with tip in IVC (Thrombosis?). Would need to be withdrawn and a CT depending on the time the line was placed for ruling out thrombosis.
Bulging of the anterior outline of the ascending aorta: Aortic aneurysm? Mediastinal tumour such as a thymoma for example?
Hola, Lola. Correct diagnosis albeit late.
….il PICC deve mantenere la sua punta alla giunzione tra atrio dx e VCS…..risulta evidente che il catetere è ” migrato” in addome….come sia giunto in quella sede sicuramente non attraverso il sistema vascolare ma per” altre” vie…fistolizzandosi …..bastererebbe iniettare del mdc e scoprire dove si posiziona la punta….Superba ripresa del Barca….non fate arrabbiare il cane che dorme !!!!
I think that lines are more frequently missed and not reported in CT scans than in X Rays examination. Actually I think incluiding lines as a part of the checking list on bone when reporting window on CT scans could help.
We are doing an Audit about PICC lines on chest Xrays and CT and at the moment the outcome is CT 0 Chest X ray 10 Champions league
Any comment on the floor?
Nice observation, although I find hard to believe that misplaced lines are missed more often in CT than in RX. Looking forward to the results of your audit.
what’s about? is it dangerous?
I am no expert in this subject, but I imagine it is not good for the patient and catheter should be removed as soon as possible.
I have seen long standing misplaced catheters causing venous thrombosis. I believe perforation of the vein is also a possibility.