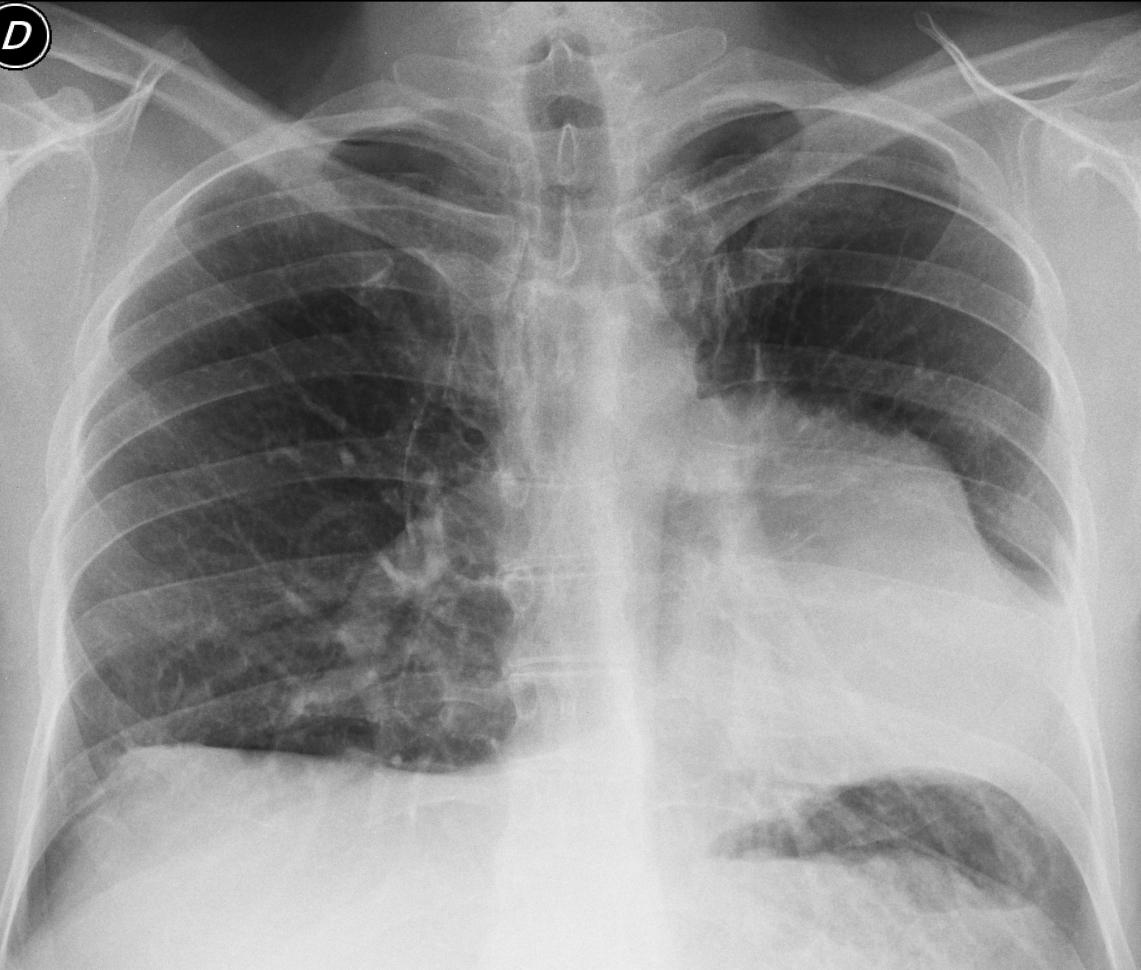
Today we are presenting pre-op radiographs for inguinal hernia in a 37-year-old-man. Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
1. Pulmonary arterial hypertension
2. Thymoma
3. Pericardial cyst
4. None of the above
Findings: the PA radiograph shows an unusual shape of the heart, which is displaced towards the left and has a bumpy left border (A, arrow). The lateral view gives the clue to the diagnosis, by showing interposed lung between the diaphragm and the heart (B, arrow). In an asymptomatic patient, this sign is highly suspicious of absent pericardium.
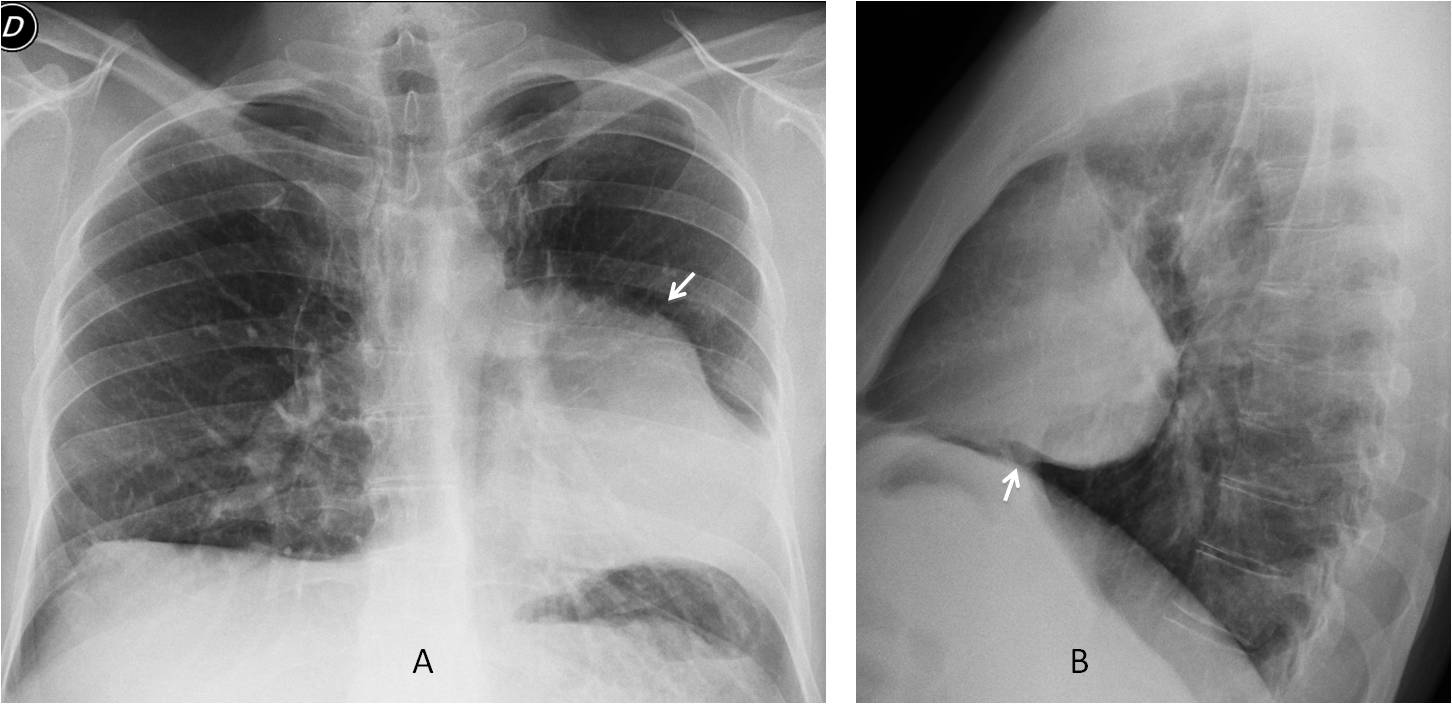
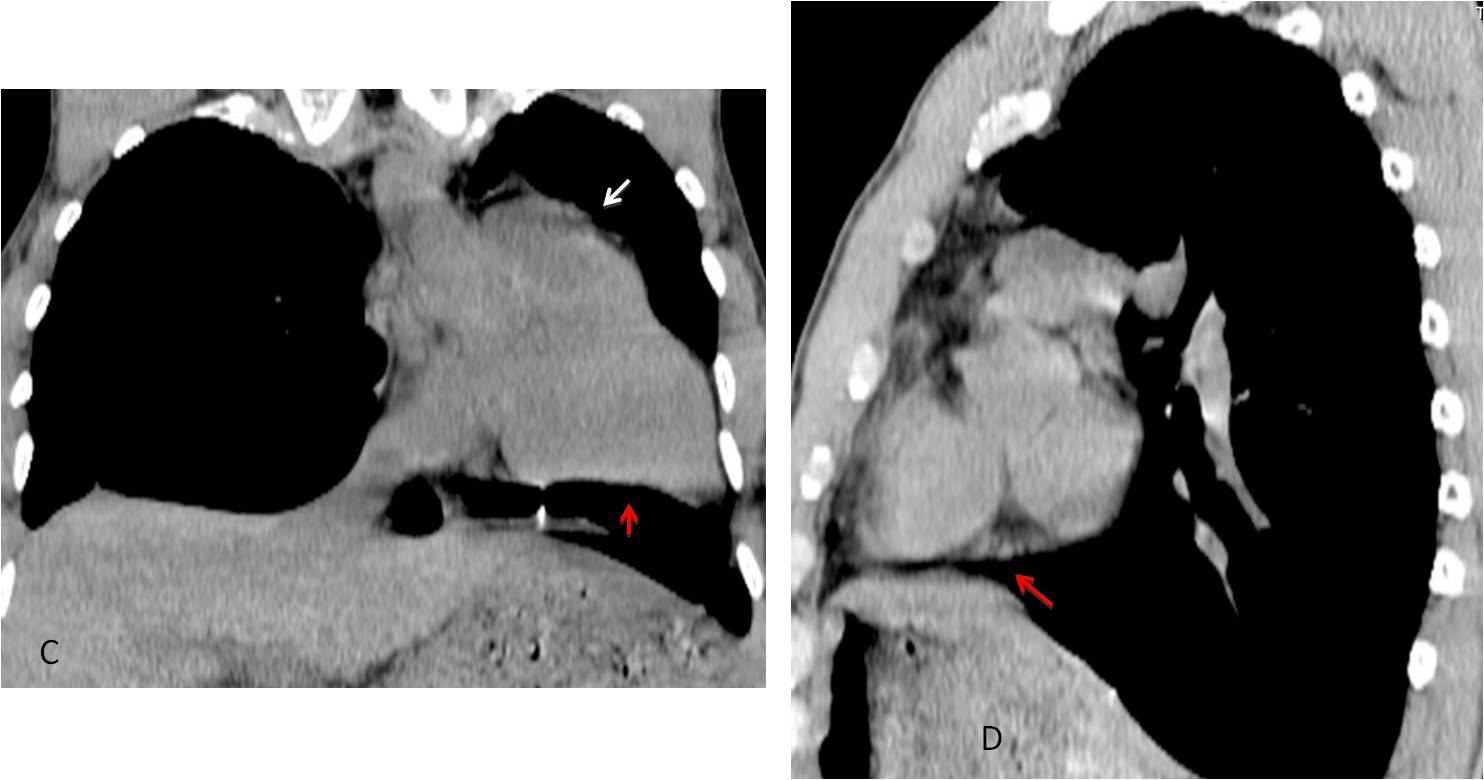
Unenhanced coronal and sagittal CT show lung under the heart in both views (C-D, red arrows). The lump in the left heart border corresponds to the pulmonary artery (C, arrow).
A chest radiograph taken five years earlier (not shown) showed identical appearance.
Final diagnosis: congenital absence of pericardium.
Congratulations to Diogo, who was the first to make the diagnosis.
Teaching point: remember that even the lowly pre-op chest (and its humble interpreter) may give pleasant surprises. This case was seen three months ago.



PA: The mediastinum is enlarged and shifted to the left with the following shadowing of the middle and inferior lung fields; has clear and smooth outer upper, middle contours but the outer inferior contour is connected with lateral chest wall and obscures the view of diaphragm and left lateral sinus – the sign of lifted and enlarged right ventricle, which is confirmed on lateral view: the retrosternal airspace and the right ventricle seems to be in contact with more than one-third of the distance from the sternodiaphragmatic angle to the point where the trachea meets the sternum.
The right central and peripheral pulmonary vessels are enlarged as the same peripheral pulmonary vessels on the left due to high blood pressure. The central left pulmonary vessels are not clear visible due mentioned mediastinum enlargement.
Laterally on the right on the level of 1-2 ribs subpleurally the small consolidation is seen – healing/ healed pulmonary infarction.
1. Pulmonary arterial hypertension
… the retrosternal airspace is filled…
There´s levoposition of the heart with abnormal left cardiac contour. The aortic knob seems normal in position. Maybe there is interposition of some lung parenchyma between the aorta and pulmonary artery. Since this is an asymptomatic patient I think partial absence of the pericardium would be a good hyppothesis.
Dear professor, in PA x ray we see a left mass and we can outline de heart and left hilum, suggesting a retrocardiac mass. In perfil we see this mass shows an round contour and has a apparent contact with heart shadow. Our opinion: mediastinal mass, probably pericardial cyst. Timoma, we think it`s not the typical mediastinal position.
Three responses and three different diagnosis.
Waiting for a brave radiologist to break the tie!
The cardiac silhouette is missing. I can´t delimitate its right and left border. In the lateral view there is an increased density proyected over de anterior-medium mediastinum, son I think a pericardial cyst would be a good option. The retroesternal space is partially obliterated.
There is a flattened/inversed right hemidiagphram, and I am doubting about LLL collapse but the lateral view is unremarkable in this aspect.
I vote for Option 4 (none of the above) . my answer is left pulmonary atelectasis, probably lingular bronchus.
as we can see normal pulmonary arteries through the opacity, so we can exclude pulmonary hypertension, the opacity silhouetting the adjacent cardiac border, considering the fact that the lesion is incidentally discovered, with no eleventh patient compliant, most proper diagnosis is pericardial cyst.
Analysing the case with care, there is levoposition of the heart with loss of the right heart border and producing a round image on lateral view, that seems to be displaced upward from the left hemidiaphragm. Congenital defect of the pericardium (agenesis) would be a great diagnosis.
Better late than never! 😉
Pericardial cyst