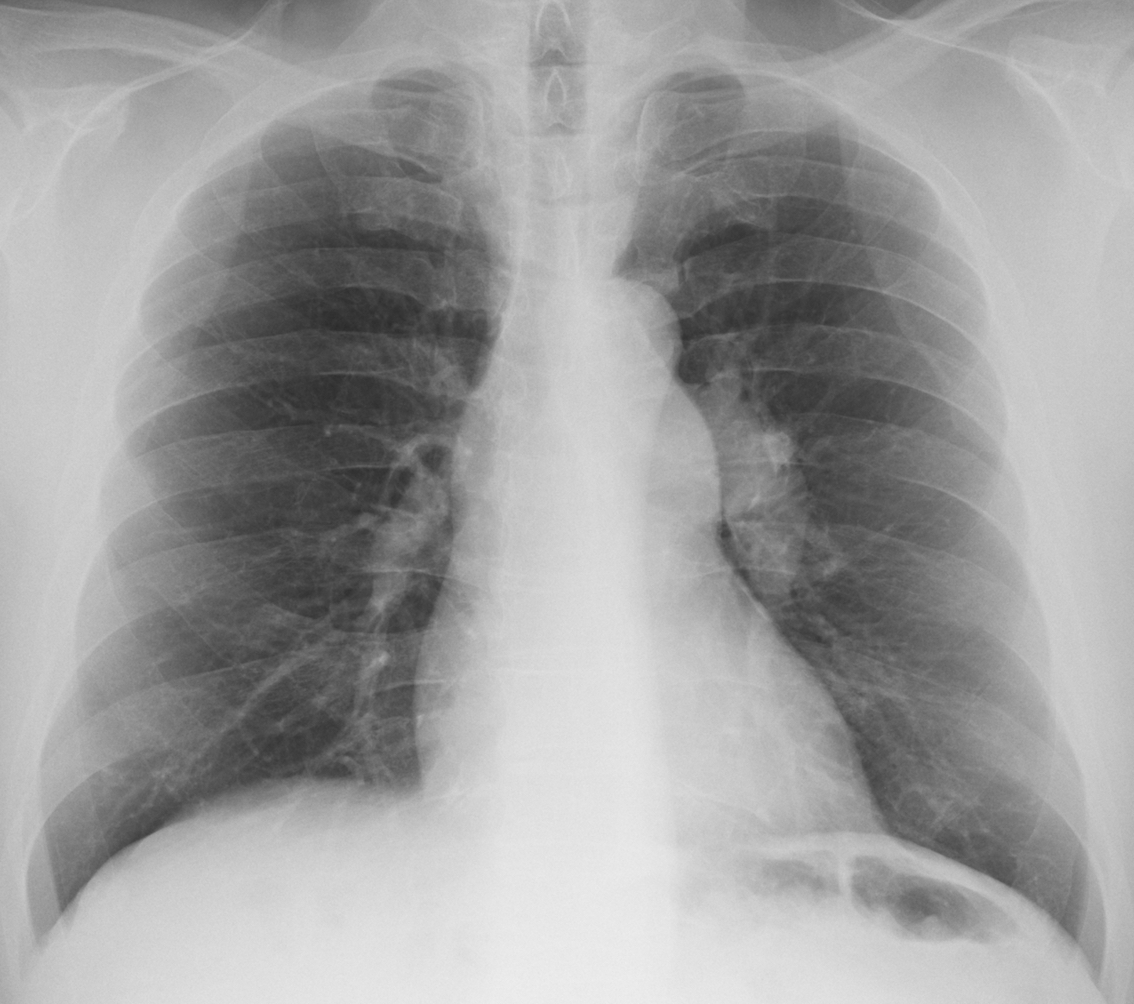
Today we are showing another pre-op case, including a PA chest radiograph of a 62-year-old man with lumbar hernia. Check the image below, give us your thoughts in the comments, and come back on Friday for the answer.
1. TB
2. Carcinoma
3. Pulmonary hypertension
4. None of the above
Findings: the PA radiograph shows a prominent pulmonary artery segment (A-B, arrow) and an enlarged left hilum (A-B, red arrow).
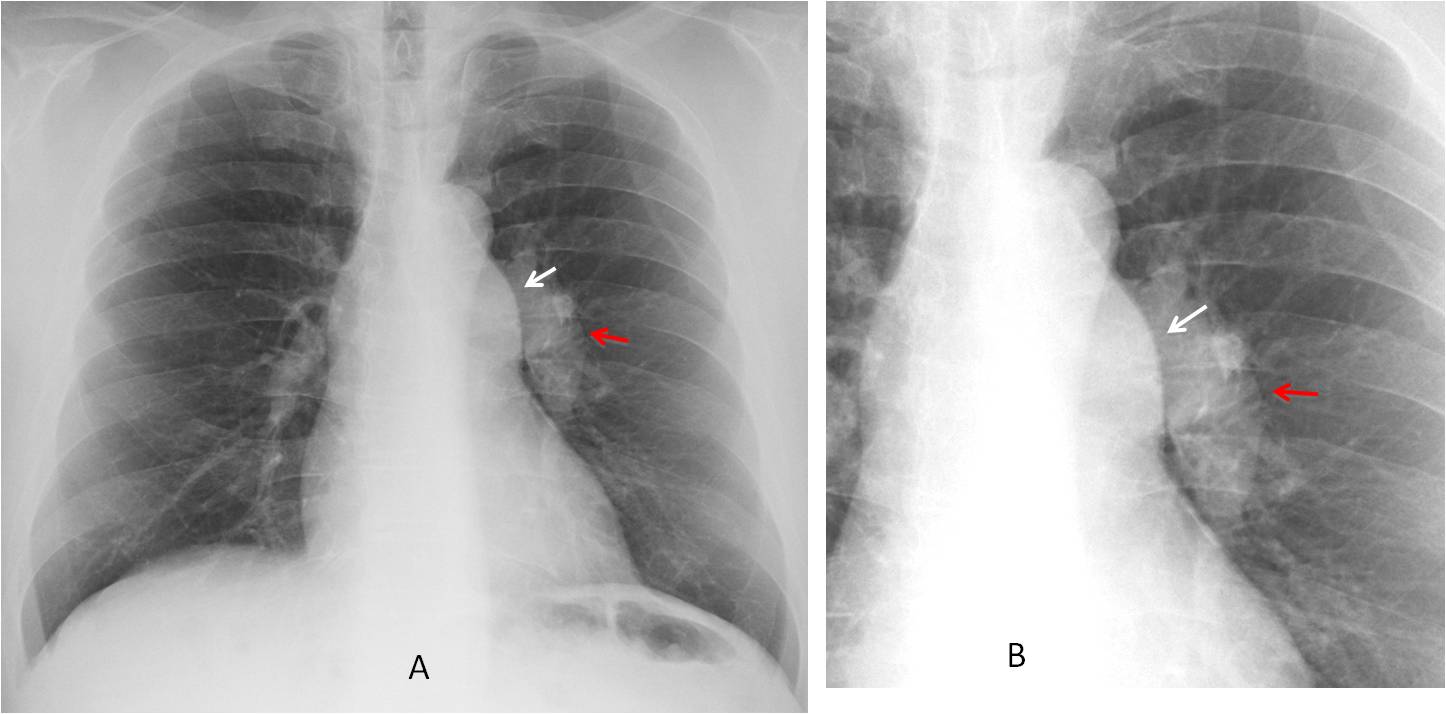
This combination of findings is highly suggestive of dilatation of the main and left pulmonary arteries and should not be confused with enlarged lymph nodes (See Diploma case 52).
Enhanced axial and coronal CT confirms the diagnosis (C-D, arrows).
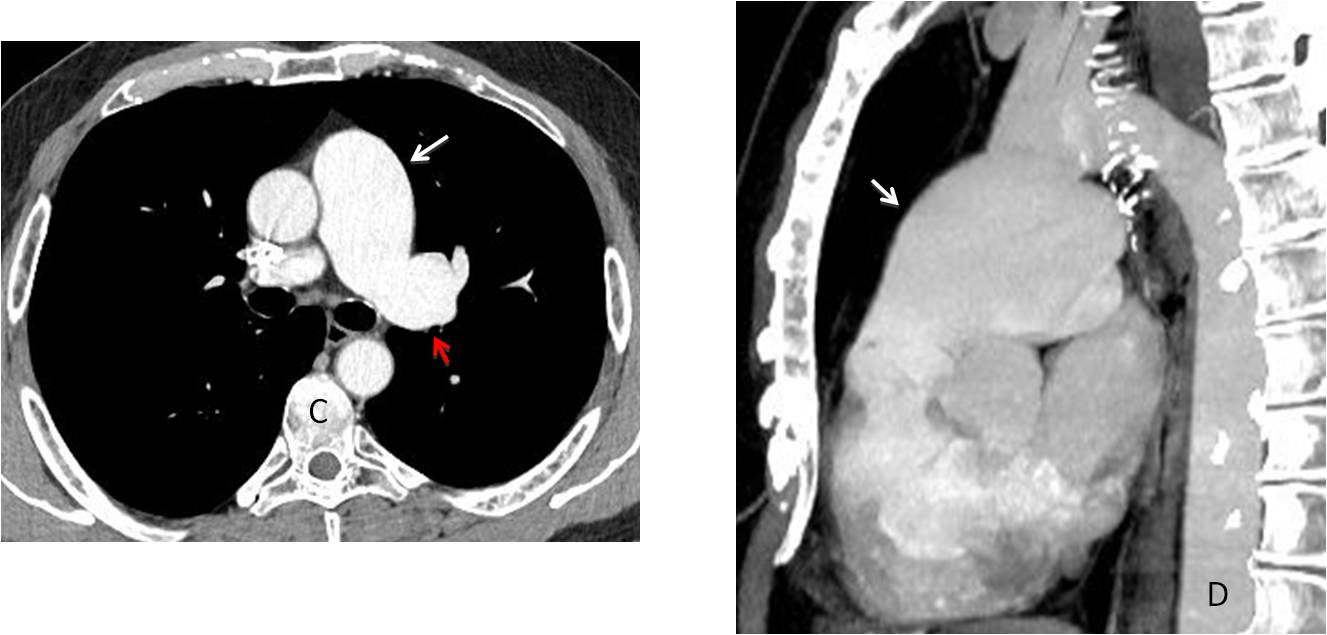
The etiology of these findings is either pulmonary valve stenosis or idiopathic dilatation of the pulmonary artery. In this patient, further work up did not demonstrated valve stenosis.
Final diagnosis: idiopathic dilatation of pulmonary artery
Congratulations to Mauro, who was the first to mention the correct diagnosis.
Teaching point: as I have mentioned before, congenital malformations in adults are not unusual. We should learn to recognise them to avoid confusing them with other pathology.


Hello.
I see enlargement of the pulmonary trunk and the left pulmonary artery, with some calcifications. Maybe an aneurism secondary to pulmonic stenotic valvar disease?
Dear professor, we see a dense and apparent enlarged left hilum, which may correspond a hilar mass or lymphadenopathy. Lateral view could help.
2. carcinoma.
It was a pre-op case and only a PA view was taken. Sorry
Hello,
I think enlargement of left hilum is vascular etiology. Pulmonary hipertension is in my opinion resonable option – only I dont know why finding is only on left side.
I think that he has a dilatation of the main and left pulmonary artery, and I supose that the patient is asymptomatic, so Congenital Pulmonary valve stenosis would be a good diagnosis.
I am also of the opinon that the dense left hilum is of vascular etiology with a dilated pulmonary trunk in an otherwise normal cardiac silhouette. For chronic pulmonary hypertension you would expect a widened right hilum, too.
A rare and in an asymptomatic patient rather unlikely diagnosis would be a intimal sarcoma of the left pulmonary artery and pulmonary trunk.
I like your diagnosis of sarcoma. Is very imaginative. But, as you say, highly unlikely.
In most of my cases, what you see is what you get 😉
We see also an enlargement of the aortopulmonar window, which may correspond lymphadenopathy secondary a hilar mass, which produces a dense hilum.
Lt main pilmonary artery aneurysm
Hello, Dear Professor.
On the PA view there is enlagement of pulmonary trunk and left pulmonary artery. I think it is due to pulmonary valve stenosis, it is usually asymptomatic when it doesn’t coexist with VSD. And asymmetry in pulmonary artery is due to jet stream effect. Peripheral pulmonary vasculature is usually normal – as in this case.
You did your research. Congratulations
There is dilatation of main pulmonary artery and left pulmonary artery
The right pulmonary artery is normal in calibre and heart is not enlarged.
No peripheral oligemia
Findings are suggestive of pulmonary valve stenosis. Echo is recommended for further evaluation.
Good!
There is an opacity anterior to aortic or pulmonary trunk in anterior mediastinal
….pregiatissimo professore….la lezione su questo caso è inerente ad un “segno” radiologico definito come “segno ilare” che serve alla DD tra pertinenza polmonare di una massa, una massa mediastinica ed infine una “massa”di natura “vascolare” della opacita°….in questo caso i vasi polmonari “convergono” verso l’opacità: non vengono oscurati nè dislocati…..INOLTRE il cono di efflusso del tronco della polmonare è dilATATO….i campi polmonari superiori sono più perfusi…..stenosi dell’arteria polmonare distalmente ai vasi per il lobo superiore….sempre da Bari con stima….
…professore, grandissima Spagna nel 1° tempo, ma nessuno goal….goal solo su papera di Buffon nel 2° tempo…..poi la Spagna è sparita…..calo fisico e fari “spenti” di Iniesta che non ha più orchestrato a centrocampo….pari giusto…..ma la Spagna non può fare solo possesso estenuante di palla senza concretizzare con tiri in porta…inoltre il “taka-Tika” è dispendioso fisicamente ed alla lunga stanca, sopratutto gli “anziani”(vedi Iniesta), ….occorre anche giocare con palle lunghe ed attaccanti bravi di testa per far salire la squadra….se il ritorno è a Barcellona ci vedremo….