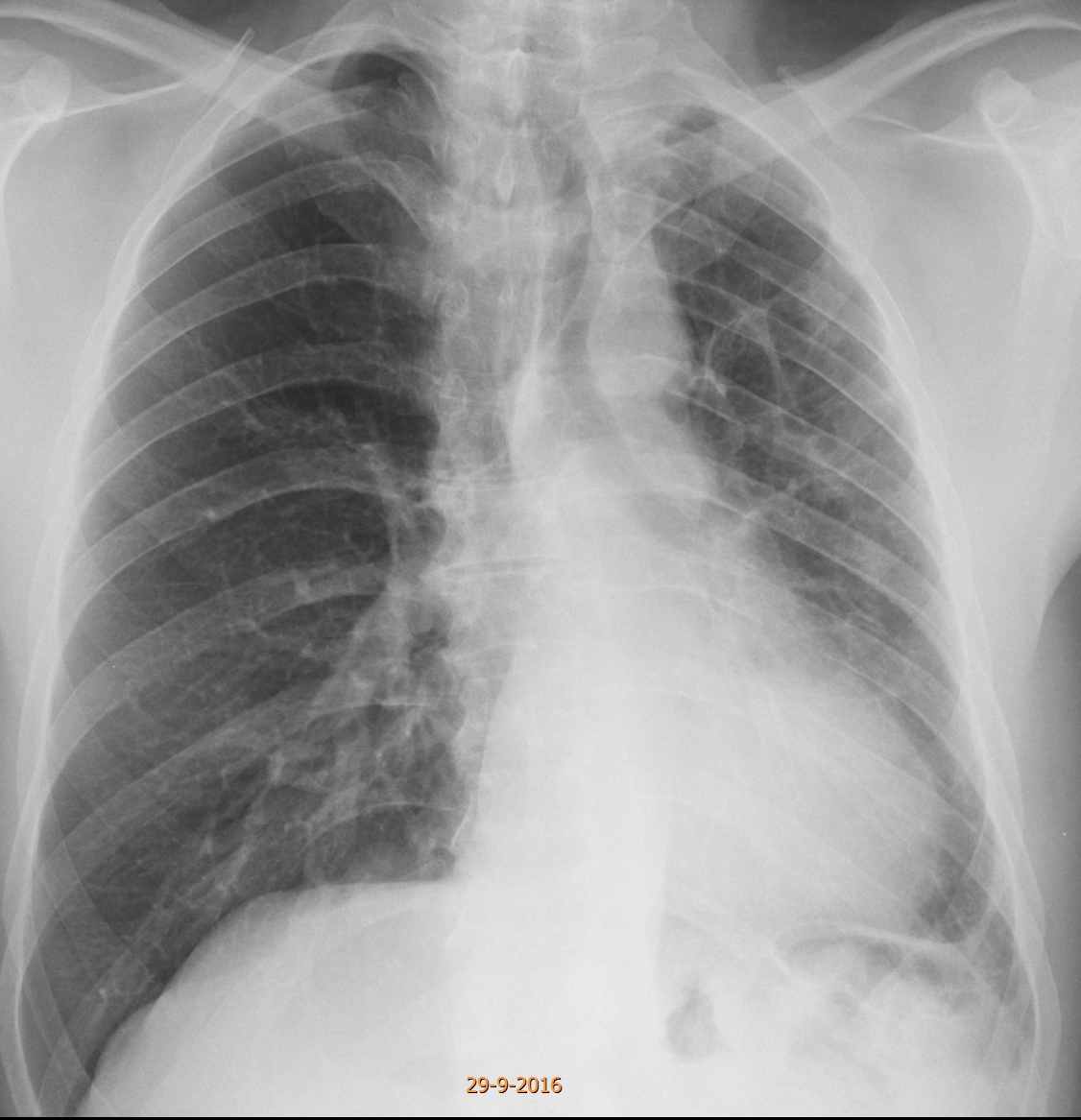
Today we are presenting a recent case. The PA radiograph was made for routine check up of a 49-year-old male.
Check the image below, leave your thoughts in the comments and come back on Friday for the answer.
1. McLeod syndrome
2. Changes post-TB
3. Congenital lung hypoplasia
4. None of the above
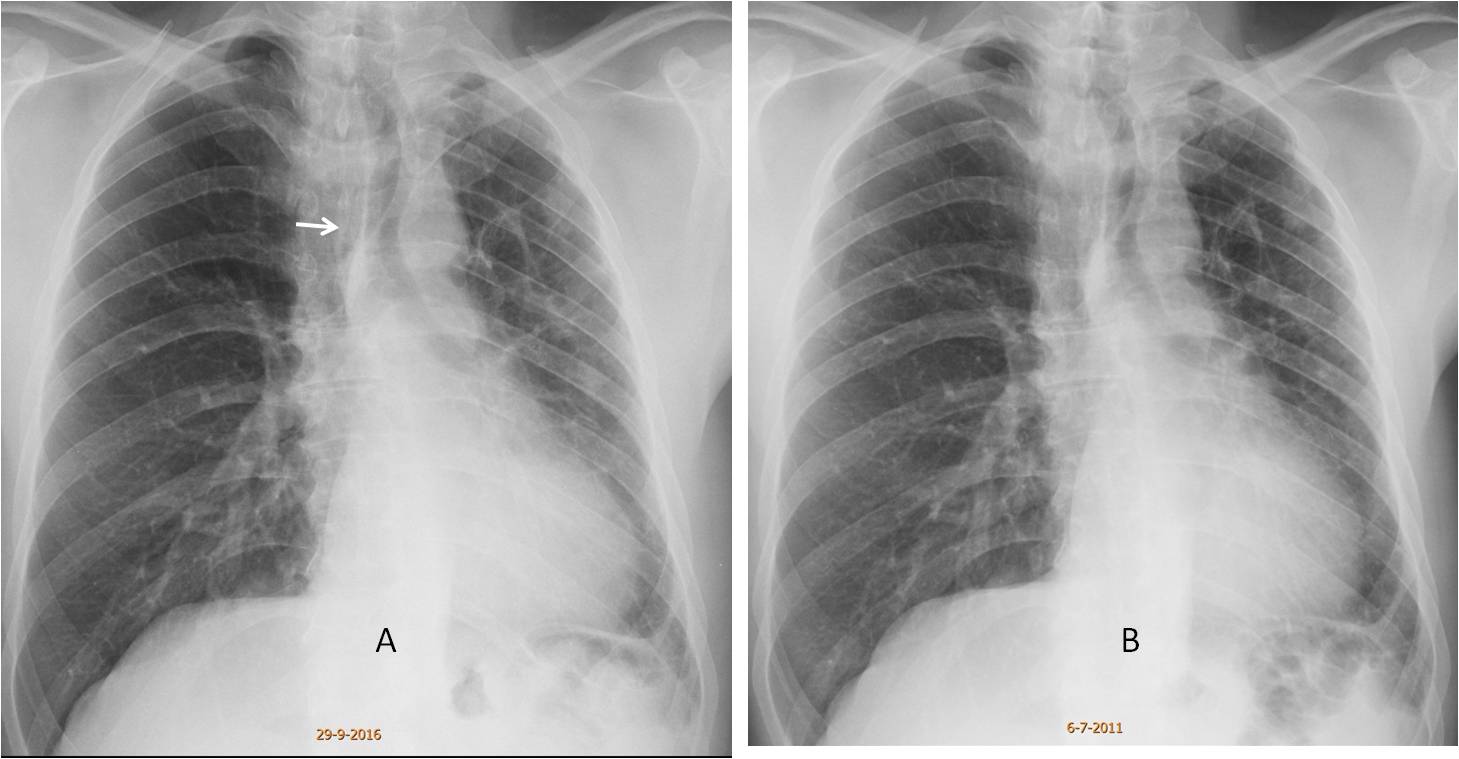
Findings: the PA radiograph shows a small left lung, with mediastinal shift (A, arrow). Of the proposed answers, hypoplasia of the left lung is very rare (agenesis occurs more frequently, but it appears as a white hemithorax). McLeod is a good possibility, but an expiration film did not show air trapping. The patient had been diagnosed with old TB in a previous film five years earlier (B), but we questioned him and he denied any history of TB.
The appearance of the chest and the lack of symptoms suggested to us a congenital vascular hypoplasia, either arterial or venous.
Enhanced CT shows an absent left pulmonary artery (C, arrow), with numerous bronchial collaterals at the left hilum (D, arrow). There is a reticular pattern in the left lung with pleural nodules (E, circle), which represent collateral circulation from pleural vessels.
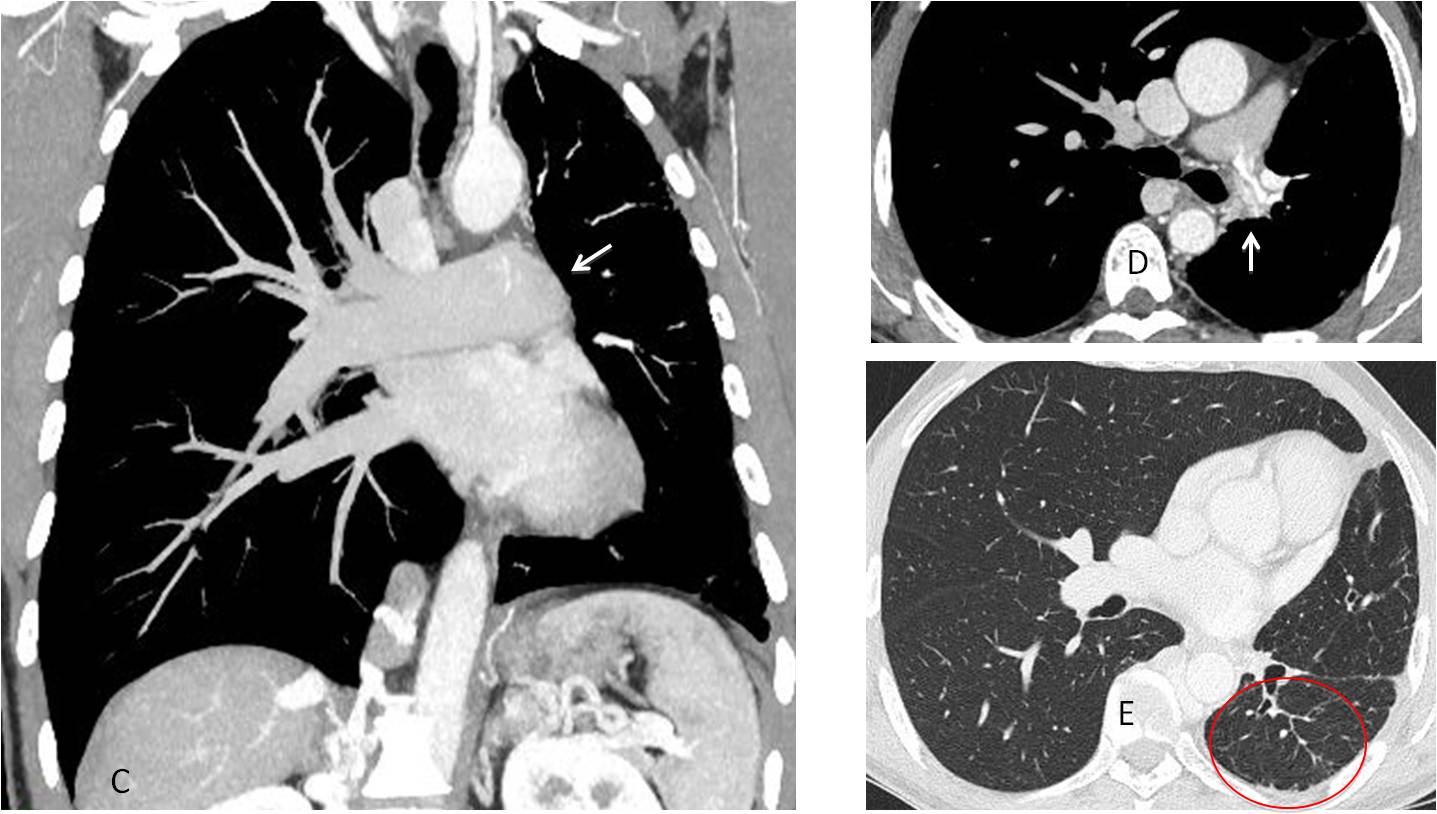
Final diagnosis: congenital absence of left pulmonary artery
Congratulations to Mahmoud and MK, who were the first to suggest this difficult diagnosis
Teaching point: this is another example of a rare congenital condition discovered because intellectual curiosity led us to perform CT and arrive at the correct diagnosis


Answer : Non of the above.
McLeod syndrome: unlikely as the smaller left lung is not hyperlucent
Changes post TB: unlikely as there is no fibrotic scary changes
Congenital lung hypoplasia: unlikely as it is usually opaque
Possible cause is interrupted left pulmonary artery , CECT is recommended.
There is a lost volume of the left hemithorax, and we can see mediastinal and tracheal shift toward the left affected side. I can´t delineate the left hemidiagphram.
We can see some tracts, so I thinK that MacLeod syndrome will be a good option (1), but a left pulmonary artery atresia (4) it´s too a nice option.
Hello professor.
Is there the “figure of 3” sign? If there is aortic coarctation, maybe there could be an associated anomaly of the pulmonary vasculature, as mentioned by above.
No figure of three. There was no systemic hypertension
I think there is mild blurring of the left heart border, associated with increased density of the left lung. These findings may secondary to LUL collapse. Maybe bronchial neoplasm?
Maybe, but films taken four years earlier were unchanged
Small volume of left lung (but it is not hyperlucent so it is not Swyer James syndrom) mediastinal shift to the left, I can not see any vascular structures of the left hilum so I would say that it could be LLL colaps or hypoplastic left pulmonary artery. I think lateral approach would bring some additional information.
Ok, perhaps McLeod syndrome is not a good option (too much loss of volume and no hyperlucent).
There is a loss of left hemithorax volume with mediastinal and tracheal shift toward the left side. Agenesis of the left pulmonary artery with pulmonary hypoplasia is the best option.
In my opinion, McLeod is always accompanied by air trapping.Therefore, you cannot make the diagnosis without expiratory films.
I agree with your second opinion
Hyperexpanded compensatory right hemithorax.
….pregiatissimo prof. Il polmone sx è’ ipoespanso, con compenso funzionale del controlaterale, con shiit di tutto l mediastino…..non si vede l’arteria polmonare sx e le sue diramazioni, mentre la vascolarizzazione polmonare appare disordinata…..il seno costo frenico è libero e non ci sono calcificazioni adenopatiche e/ o polmonari quali esiti di pregressi eventi flogistici(d’altronde basterebbe questo ad escludere una tbc),,,MC leod si esclude perché’ non c’è’ air trappista anzi il polmone sembra opaco….l’ ipotesi di una ipogenesia polmonare da anomalia vascolare sia la più’ probabile…..prima di eseguire una angiotc…….NB il Bari, un disastro !!!!!!