Dear Friends,
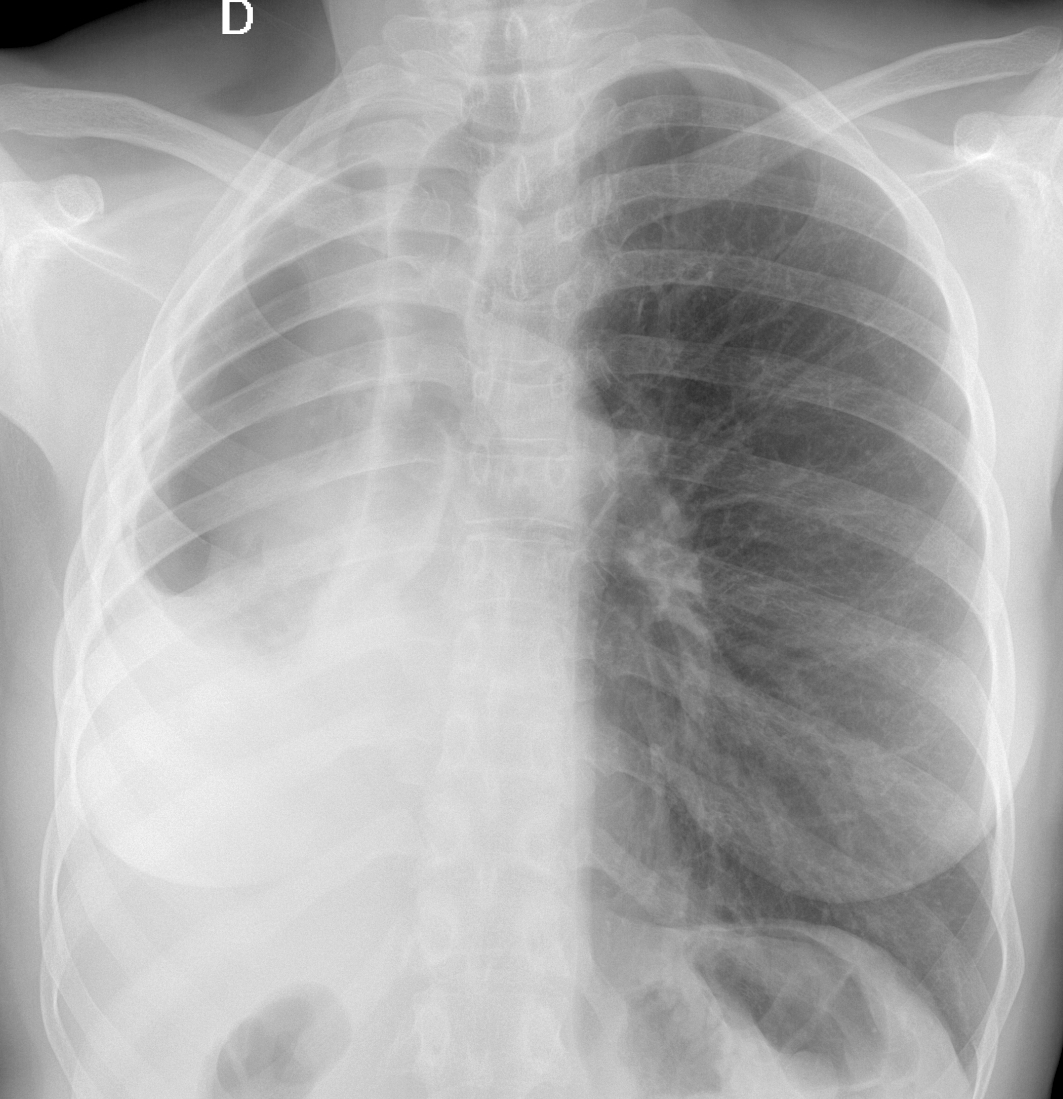
We are starting the new year with a warm-up case. Today we are presenting a PA chest radiograph of a 57-year-old woman with a cough and sputum production.
Check the image below, leave your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Changes post TB
2. Congenital right lung hypoplasia
3. Mesothelioma
4. None of the above
Click here for the answer to case #151
Findings: the PA radiograph shows a small right hemithorax with deviation of mediastinum towards the right. There is marked pleural thickening (A, arrows), and a small right lung. Close inspection shows a lack of vessels in the apparent right lung indicating that the air is in the pleural space. This combination of pleural disease and pleural air is strongly suggestive of a bronchopleural fistula (BPF).
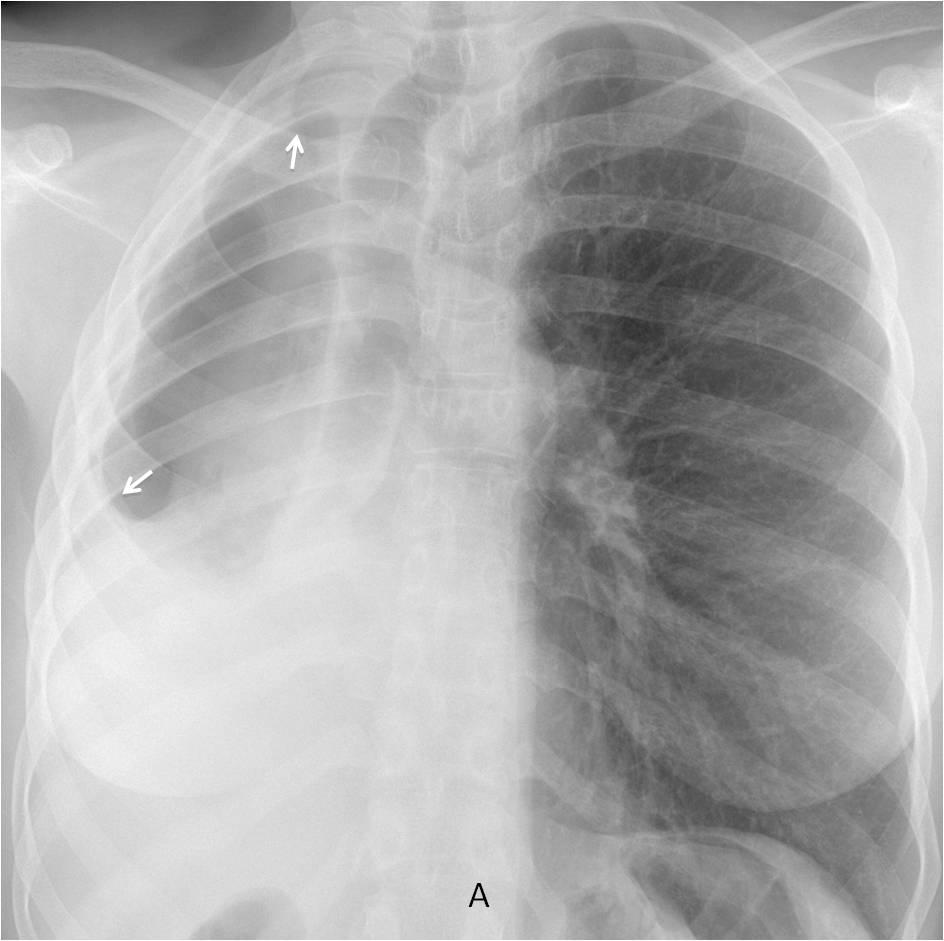
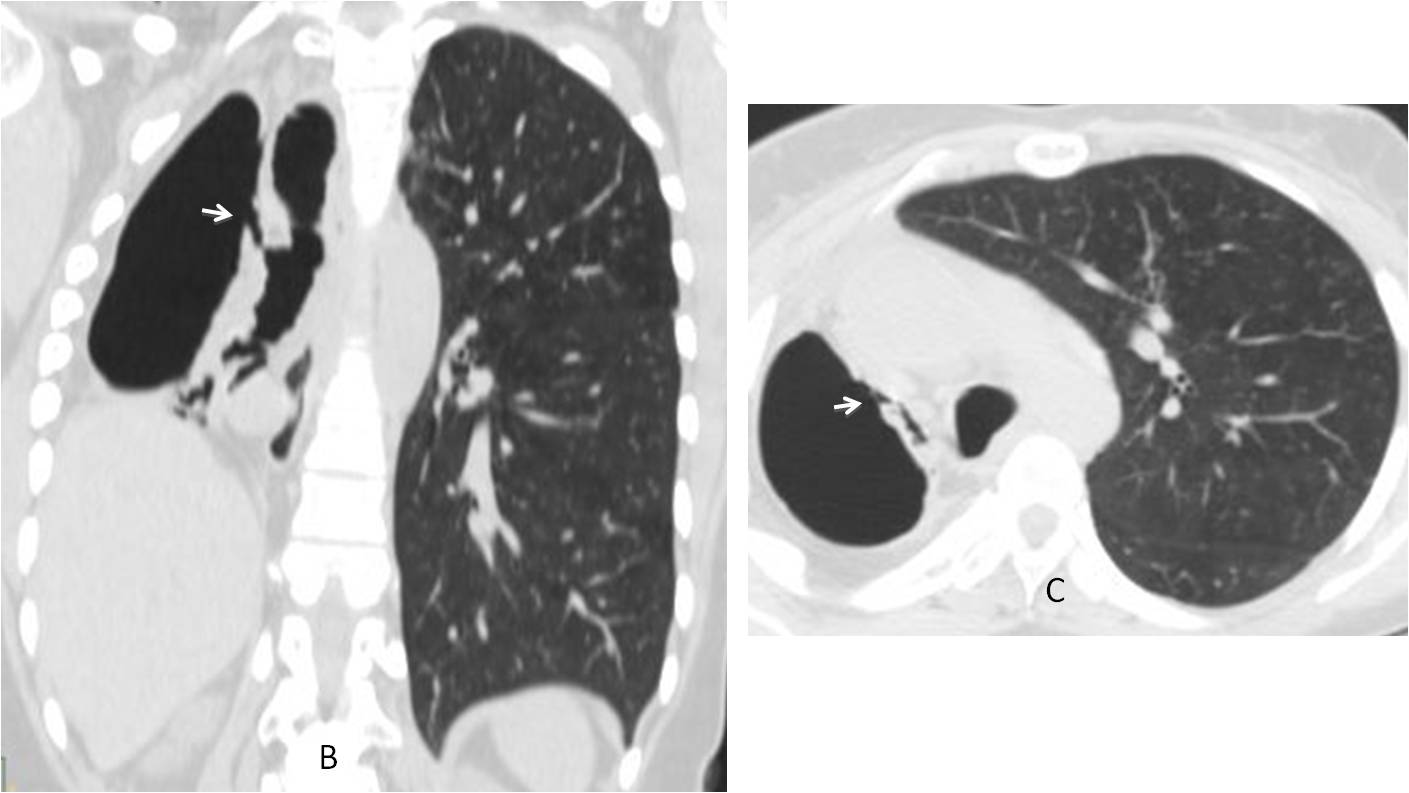
Coronal and axial CT confirm the initial diagnosis, demonstrating the fistulous tract (B-C, arrows). There is marked collapse of the right lung.
The patient was originally from Africa and had had no previous interventional procedures. She did not come back to our institution and was lost to follow-up.
I am showing this case because I thought it interesting to show a rare case of non-surgical BPF.
Final diagnosis: bronchopleural fistula, probably secondary to previous TB
Congratulations to MK who was the first one to suggest the diagnosis
Teaching point: The combination of chronic pleural changes and pleural air with no previous intervention should raise suspicion of BPF.


Change s post TB
There is an important loss of volume of the right hemithorax with displaced mediastinum towards this side. An hydroneumothorax is present so a bronceo-pleural fistula should be descarted.
Also there is a decreased space between the ribs in the right side. Any surgical hystory?
If no surgical hystory, TBC or asbestosis are good causes for chronic pleural disease and so, for broncho-pleural fístula. A pulmonary infection if another cause of broncho pleural fistula.
No surgical history
I will give it a try 🙂 I see displacement of the trachea and cardiac silhouette to the right as well as slightly diminished ipsilateral intercostal spaces. The right hemithorax appears smaller compared to the left. This indicates significant volume loss of the right lung with compensatory hyperexpansion of the left (I see 11 posterior ribs). There seems to be a small air-fluid level with meniscus sign on the right indicating an effusion. I do not see any vascular lung markings in the lateral portion of the right hemithorax which might mean there is also a right-sided pneumothorax. The right mainstem bronchus appears wider than the left. I also see opacification within the right bronchial lumen resulting in significant narrowing/obstruction.
I think the patient has a right hydropneumothorax from an obstruction/narrowing of the right mainstem bronchus due to neoplasm or retained secretions. But without additional patient information or until a CT is done, congenital pulmonary hypoplasia/aplasia must remain part of the differential, although less common.
Tracheobronchomegaly
…penso potrebbe trattarsi di una complicanza di una biopsia transtoracica, con idropneumotorace e completo collasso polmonare dx.
No previous intervention of any sort.
dear professor, we think it could be consequence of TB, probably with a bronchopleural fistula or direct pneumothorax.
My hypothesis is:
Signs of right hydropneumothorax, accompanied with ipsilateral loss of volume (a detailed description is already done by “marco”, so I won’t repeat it). There is also displacement of the main bronchial tree to the right. The cardiac silhouette is not recognisable, due to right displacement also.
This would be cosistent to the presence of a right neoplasm. There is also sign of pleural thickening.
Combining all these, and without additional patient information, I would consider the diagnosis of mesothelioma as more likely. The other cases remain in the differential, and I would consider secondary the post-TB changes (although I would prefer to rule out the neoplasm / mesothelioma case in a plain chest radiograph like this).
there is volume loss in right lung. decreased intercostal spaces likely chronic etiology. right hydropneumothorax is seen. right bronchus appears narrowed distally? obstructing lesion. mediastinal lymhadenopathy due to tuberculosis could be the cause
Hi I am a new member in your really interesting company and a really young radiologist!so I will make my first try.be nice! there is volume loss of right hemithorax and mediastinal shift towards the right (so cardiac contour is not recognised). Further more I think there is abnormal wall thickening of right bronchus. As previously mentioned there are signs of pneumothorax and maybe hydropneumothorax although I cannot see an air-fluid level.I can think of an bronchopleural fistula second to an operation or if there is not surgery history, second to a malignant condition.
Welcome Vivi. Discussion not bad for a young radiologist! You forgot TB as a cause of BPF, though.
Congenital right lung hipoplasia