This week we are showing a relaxing case. Images belong to a 64-year-old man with a cough and fever. What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Findings: chest radiographs show a pulmonary infiltrate in the anterior segment of the RUL. There is loss of volume as demonstrated by concavity of the minor fissure (A-B, arrows). For those of you that have diagnosed fluid in the minor fissure, remember that the border is convex instead of concave.
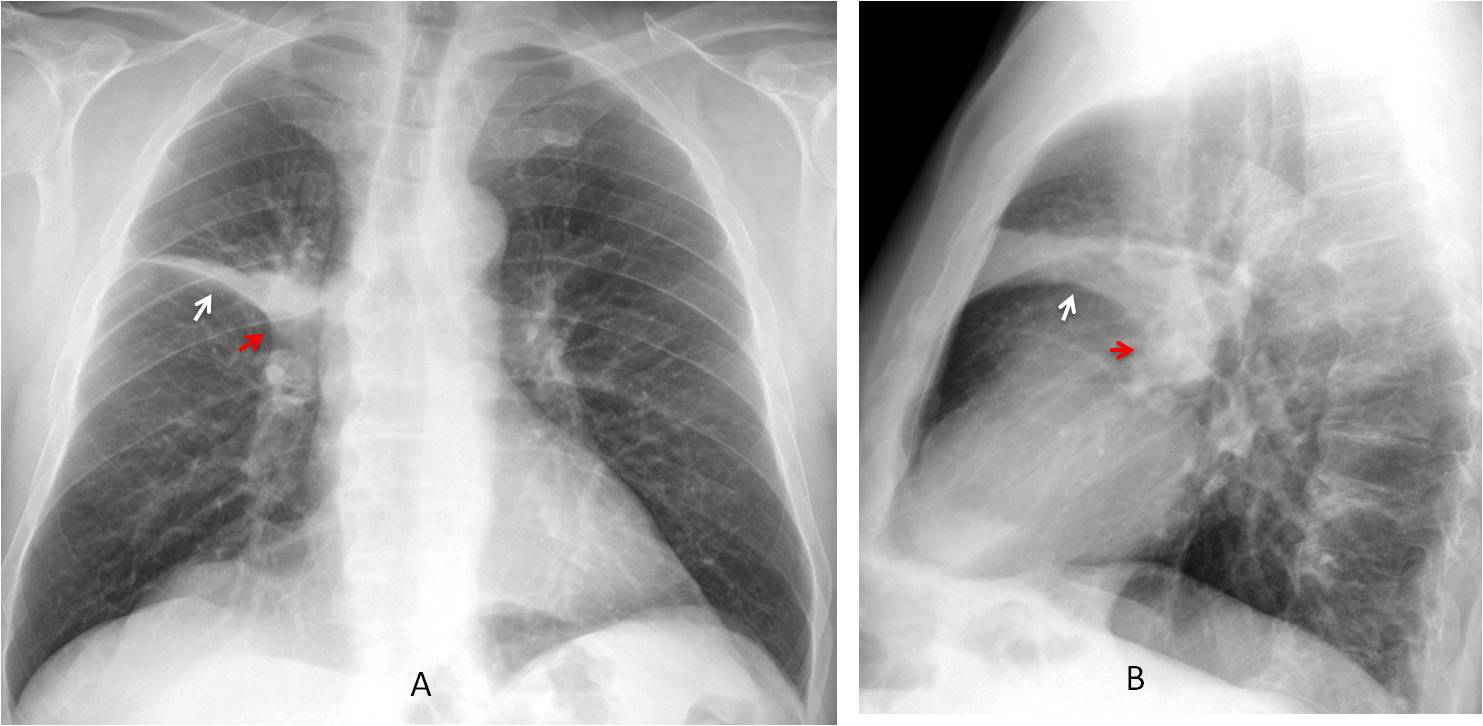
Another significant finding is a mass in the hilar region (A-B, red arrows), creating an evident reverse “S” (Golden sign). This sign is highly suspicious of a central carcinoma.
Enhanced coronal and axial CT demonstrate a mass obstructing the RUL bronchus (C-D, red arrows) and narrowing the main right bronchus (C, arrow). PET-CT shows enhancement of the mass (E, arrow).
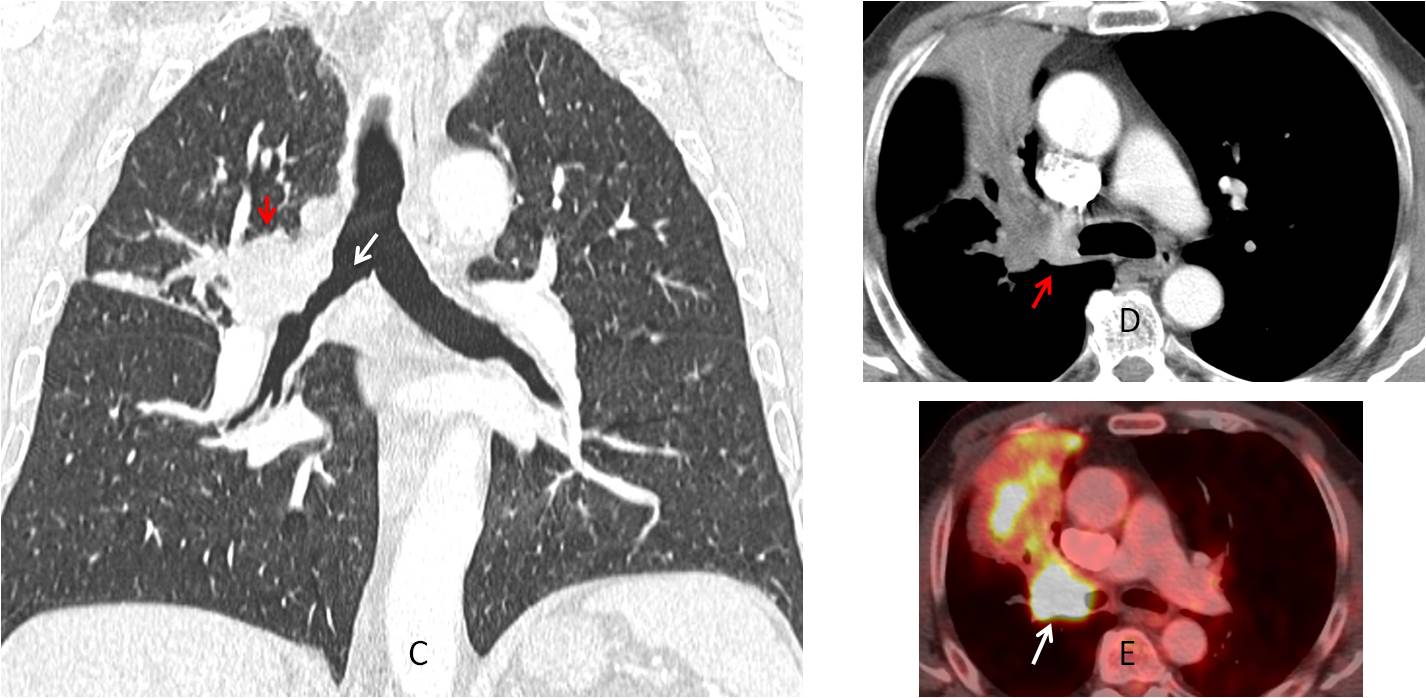
Final diagnosis: carcinoma of RUL bronchus with segmental collapse.
Congratulations to MK, who was the first to suggest the diagnosis
Teaching point: Golden sign is infrequent but, when present, is a good indicator of malignancy and should prompt a CT




Good morning!!
In the AP view there is a slightly right displacement of the trachea and an amputation of the principal right bronchus. There is an increased density with smooth margins over the minor fisure, probably an atelectasis.
In the lateral view there is an increased density in the right hilum.
Hiliar lesion (adenopathy, tumor…) with secundary atelectasis?
The medial lobe is colapsed. It is right medial lobe atelectasis.
Agreed…
Additionaly there’a a large rounded lypmh node in the right hilum indicating lung cancer being the cause of the collapse.
The lung disease is above the minor fissure, meaning RUL afectation. If it were RML, disease would be below the fissure. Sorry to disagree 😉
Fluid in minor fissure with adjacent pneumonia consolidation.
Lost of volume of the right upper lobe with enlargment and increased density of the right hilum and segmantari atelectasis. In the lateral view we can add the finding of a probably subcarinal adenopathy.
First treat the acute symptoms (atb…) and order a control plain in a few weeks to check a radiological improvement, if it doesn’t consider
Consider CT*
Yes, we did a CT 😉
Fluid along the horizontal fissure
Golden sign
Fluid in the minor fissure.
Fluid in the fissure usually have a convex border. This one is concave. Sorry to disagree 😉
On the right there is homogeneous wide horizontal linear opacity well marginated localized on the level of projection of minor fissure – suggestion of pleural inflammatory reaction, with probably restricted effusion in fissure.
Paying attention the decreased attenuation in subpleural region of the vessel architecture in the right upper lobe due to apical pleural thickening.
Doubled shadow of the right diaphragm due to its relaxation
On lateral view there is increased transparency in retrosternal space due to lung herniation and opacity in the lower anterior mediastinum suggestion pleura thickening/infiltration
Conclusion: suggestion pleural thickening and effusion in minor fissure, periscisuritis
Welcome back! See answer to Irina.
….lipoma pleurico…..Bari in ripresa…..riasaliamo ai piani alti….Non ti avevo dimenticato…
Atelectasis of the anterior segment of the right upper lobe. If persistent it is needed to rule out endobronchial lesion such as a tumour – neuroendocrine?- or other causes – benign bronchial stenoses secondary to chronic infection/Tb?, foreing body in an adult? CT will help
Hi! I cannot clearly see the continuation of the roght bronchus. So I believe there is golden sign associated with right hilum opacity (endobrochial lesion ?)and severar pycnotic-atelectatic elements of RUL. Let’s start with a CT.
Late but right 😉
Atelectasis anterior segment right upper lobe.
Hilar opacity – ?LN ?mass
right middle lobe collapse
Too high to be RML collapse. See answer to Murzin
central mass with partial segmental collapse of anterior segment of right upper lobe
Hi,
anterior segment RUL collapse with right hilar mass.