Presenting today chest radiographs of a 9-year-old girl with a persistent cough for the last two weeks, vomiting and fever. What do you see?
Check the images below and leave your thoughts in the comments section. More images will be shown on Wednesday, followed by the answer on Friday.
Dear friends, showing a chest radiograph taken seven days later. What do you see?
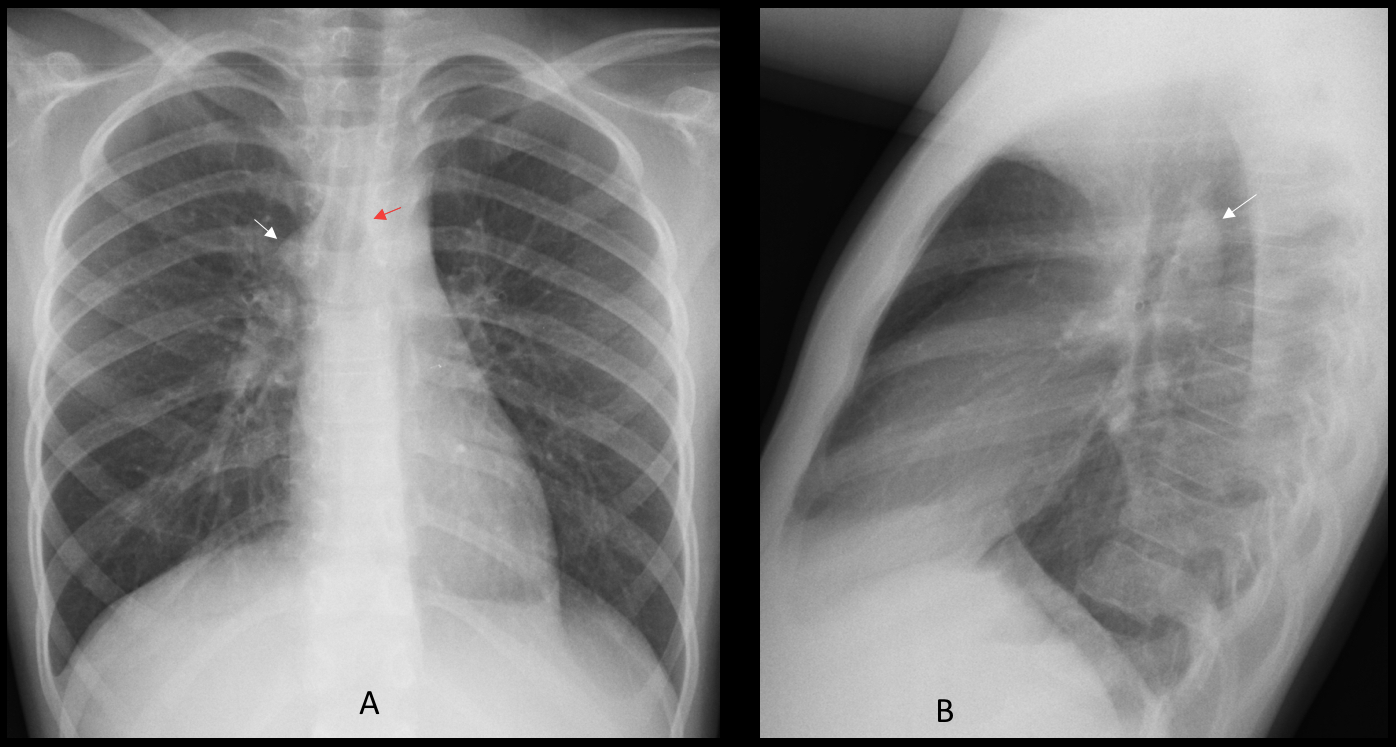
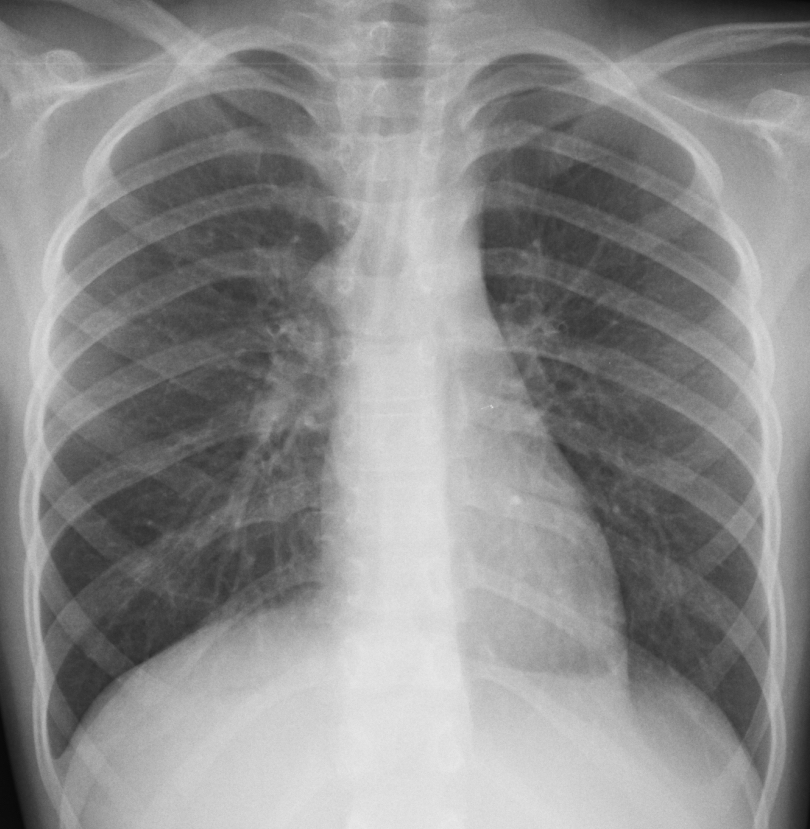
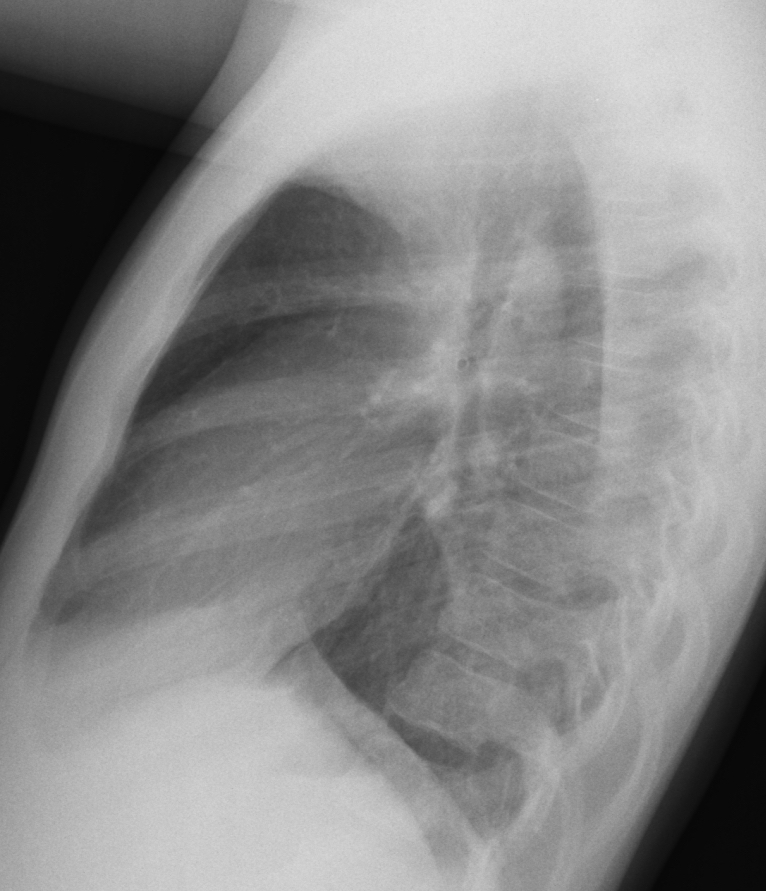
Findings: PA radiograph shows a rounded right mediastinal prominence at the level of the tracheal bifurcation (A, arrow). It could be either a lymph node or an enlarged azygos vein. The retrotracheal location in the lateral view (B, arrow) points to an azygos vein.
The aortic arch is located in the left side, as evidenced by the discrete imprint in the left tracheal wall (A, red arrow).
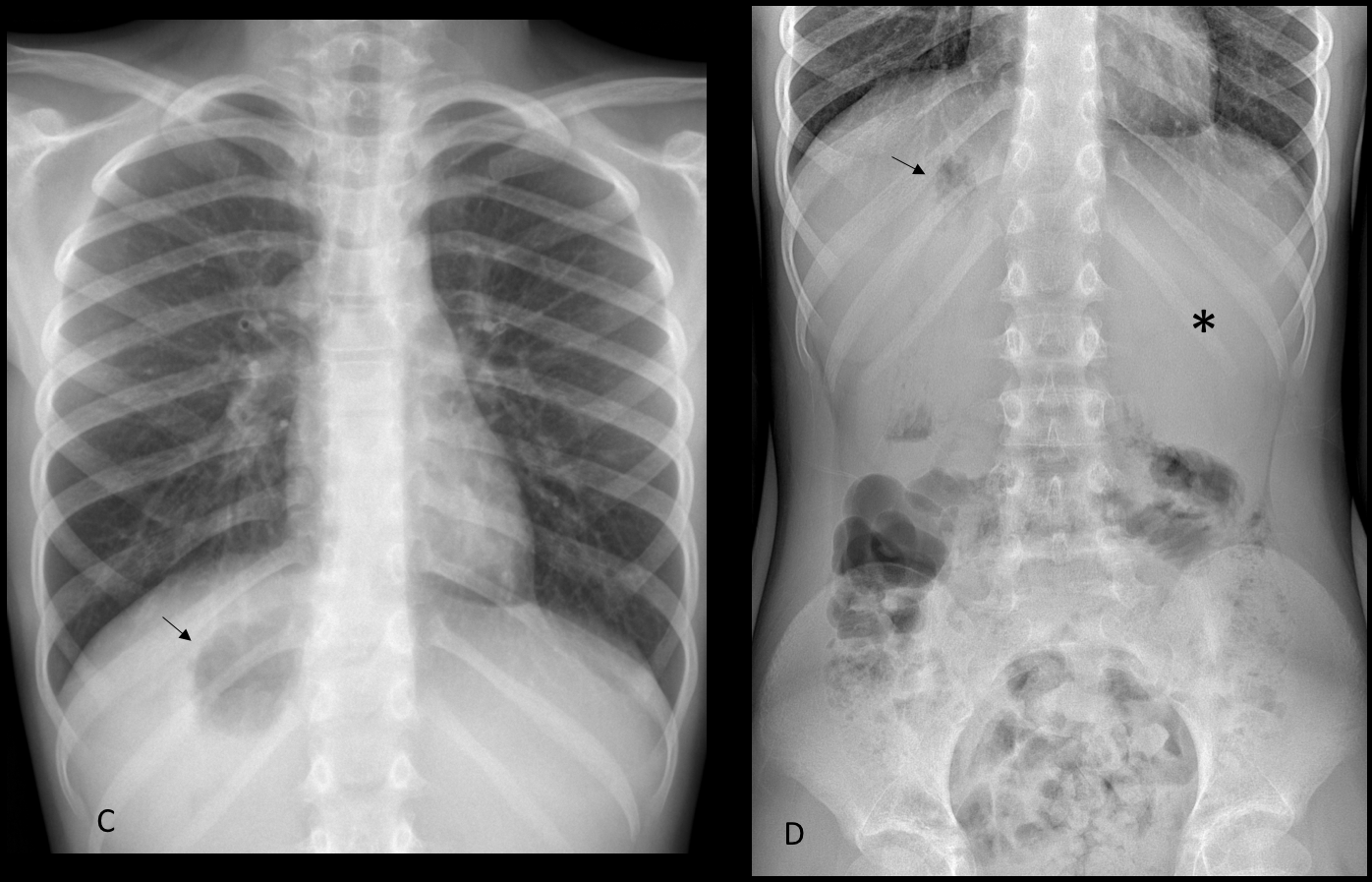
PA radiograph taken one week later demonstrates air in the gastric fornix, which is located under the right hemidiaphragm (C, arrow). It is confirmed by a supine film of the abdomen (D, arrow), which also shows the liver in the left upper quadrant (D, asterisk).
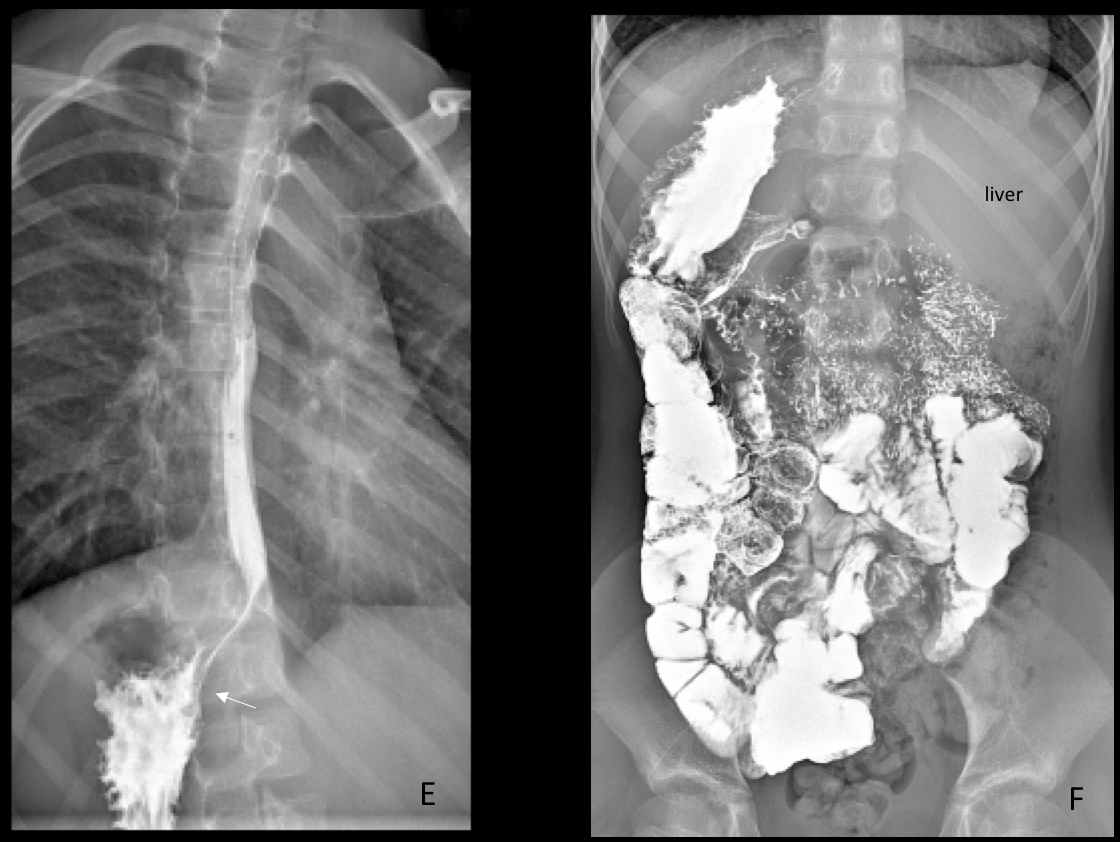
Barium study confirms the right-sided stomach (E, arrow) and malrotation of the bowel, mostly located in the right side of the abdomen (F).
The patient was diagnosed with whooping cough with positive serology to Bordetella Pertussis. The isolated abdominal malrotation was an incidental finding
Final diagnosis: Levocardia with abdominal heterotaxia and azygos continuation of IVC
Congratulations to MK and S who were the first to make the definitive diagnosis.
Teaching point: Sometimes, the unusual is more usual than expected. This is our third patient with levocardia and abdominal heterotaxia seen in the last four years (see Caceres´ Corner Case 194 and Dr. Pepe´s Summer Case 1). It may not be as rare as the textbooks state!



There appears to be a cut off sign of the right main bronchus with hyper expansion of the right lung. Possible that there is a foreign body in the right main bronchus.
To be honest with you, I don’t see hyperlucency of the right lung (look at the vessels).
Try again 🙂
Right paratracheal lymphadenomegaly and blunting of the right costodiaphragmatic recess (suggesting small amount of pleural fluid).
Tuberculosis is my best guess in this clinical scenario with that radiographic appearance. It could also be sarcoidosis but less likely.
wedge-shaped opacity seen on the lateral view over the anterior costophrenic recess, could not find a corresponding findings on the AP view.
Forget about it. It’s not important
I would say there are thickening of the posterior junction line and a small left pleural effusion.
What you call the posterior junction line is probably the esophagus. No clear signs of pleural effusion.
Tip: look at the mediastinum
Small hyperlucent finding on the left , probably lower bronchus ( retroscardial).tiny foreign body.
And remnant of thymus on lhe right
I’m not sure I can clearly see the aortic knuckle on the PA, even though the mediastinum on the left seems prominent – could be due to rotation to the left.
On the right there seems to be a round opacity just caudal to the right paratracheal stripe – it might be a slightly enlarged azygos vein, but it might be that the vein is denser and either behind or in front of this slightly more lucent round structure.
On the lateral I cannot clearly visualize the IVC shadow near the posterior-inferior heart border.
Could there be some problem with the IVC and subsequent azygos enlargement?
Good thinking! Now you have another chest radiograph to complete the findings
Good morning,
Occupation of retrotachel space by nodular opacities. Adenopathy? mediastinitis? oesophageal disease? a vascular malformation is less likely, as the patient has acute symtoms.
On the PA chest film there is a well shaped right paratracheal mass.
The differential diagnosis can be aortic arch anomaly (right arch, aberrant right subclavian artery), adenopathy or tumor.
Where is the aortic knob?on the right side?
And the gástrico bubble?
You will see the gastric bubble tomorrow 🙂
A right aortic knob is visible on the PA view. Left aortic knob is not seen. Do CT to look for aberrant left subclavian artery with possible compression of esophagus.
Forigen body in trachea
There’s a enlarged azygos vein in the PA view, and i can’t see a triangular density behind heart in the lateral view, representing vena cava. I think that azygos continuation of inferior vena cava is a possibility.
Good description. Look at the new chest radiograph
1) there is a tubular foreign body with central lumen-? toy in line with tracheal bifurcation and into rt main bronchus producing partial obstruction with obstructive emphysematous changes in rt lower zone, with mild widenind of lower intercostal spaces.
2) ?suggestion of rt aortic arch or aygos continuation in case of ivc interuption
3) medial half of left dome not seen clearlyseen with gastric fundus fluid level close to it-? hiatus hernia
4) ivc shadow not seen clearly in lateral view
i think i will stop here my imagination running riots
I think part of your imagination is running wild. On the other hand, part of it is thinking straight 🙂
Rt hilum uplifted. Follow the old man’s advice!
is there a small air-fluid level on the pa film just above the carina? I do not see it on the lateral view, though.
No air-fluid level. Sorry
Gastric bubble on the right side!!
Abdominal situs inversus with an enlarged azygos vein secondary to interruption of the IVC?
Azygos continuation of the IVC and abdominal situs ambiguus (right sided gastric bubble and possibly midline position of the liver) would suggest polysplenia syndrome due to partial absence of right-sided structures (such as the IVC) and predominance of left-sided structures.
In that case the right lung might have only two lobes, and both sides of the bronchial tree might have left-sided morphology.
I’m not sure if this is present in this case – the right bronchus seems normal to me.
You are correct in your diagnosis. Cannot tell about the bronchial distribution because a CT was not done
latest x -ray chest shows
azygos continuation with ivc interuption
retro cardiac density -mucus plug in bronchi or sequestration
eleven pairs of ribs
stomach on rt side
liver on left side
Only eleven ribs. You are right. I missed that! 🙂
altreation in azygoesohageal line and fundal gastric shadow in right