Caceres’ Corner Case 195 (Update: Solution!)
Dear friends,
Today, I am presenting a case of my friend, Alberto Villanueva.
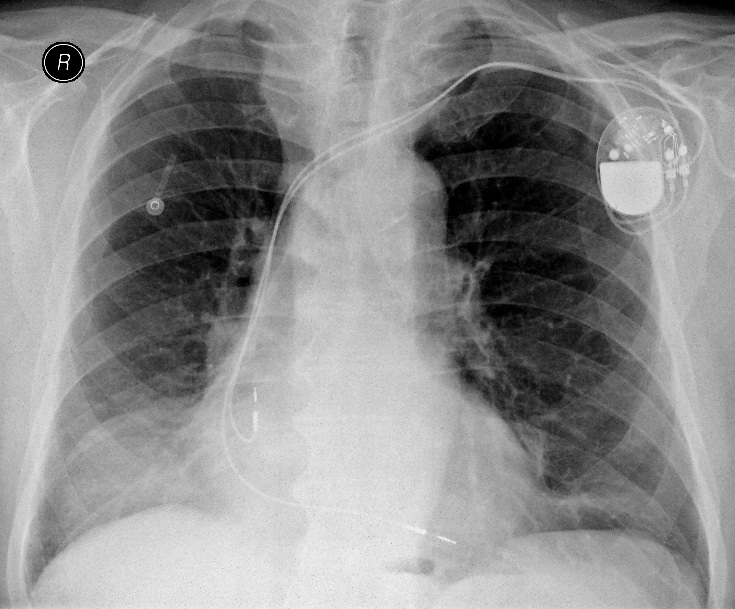
The radiographs belong to a 76-year-old man suffering from back pain.
What would your diagnosis be?
1. Loculated pleural fluid
2. Fibrous pleural tumor
3. Diaphragmatic hernia
4. None of the above
This is the last case of 2018. I am taking a short Christmas break and in 2019 I will be joining my friend, Dr. Pepe on the EBR Blog. New Caceres’ Corner cases will be posted in 2019 under the following link: blog.myebr.org.
Have a nice Christmas!



Good morning!
Bicameral pacemaker.
Loss of volumen of the right hemithorax with slighly tracheal displacement.
Well defined high density (extrapleural lesion) proyected over the RLL.
I dont think in diaphragmatic hernia. Option 1, 2 or extrapelural haematoma
I prefer the term “extrapulmonary lesion” rather than extrapleural. I believe it’s more accurate 🙂
PA: Opacity in the lower lung zone with a well-defined superior border. Right superior mediastinum seems widened, most likely due to vessels.
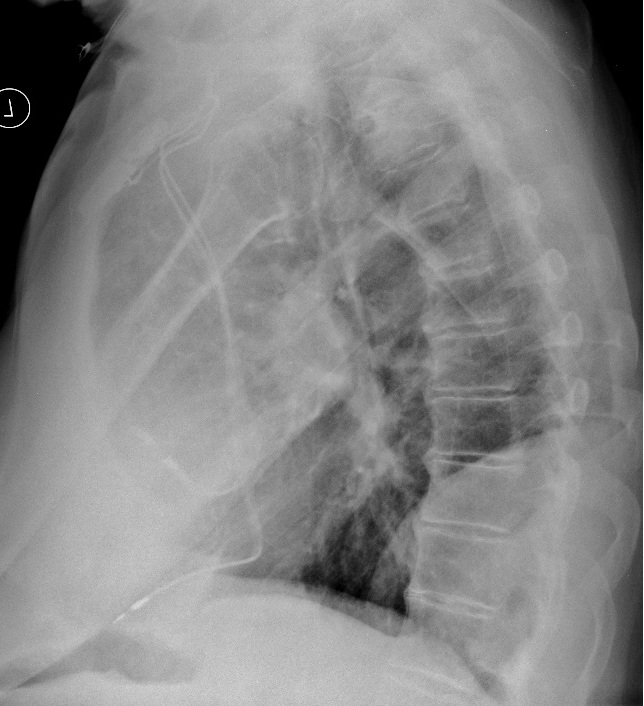
Lateral: confirms well-defined lower zone mass location posteriorly, with an obtuse angle superiorly, making extrapulmonary origin most likely. Anterior costophrenic angle seems blunted by a pleural effusion.
Given that the patient has a pacemaker, heart failure seems probable, so right sided loculated pleural effusion would fit the picture. However, round atelectasis could also be a possibility if there was pleural thickening together with fluid (however no visible converging vessels argues against this).
Presenting complaint was back pain, which could be explained by degenerative changes in the spine which are visible here in the thoracic spine, and likely present in the lumbosacral region.
I’m not sure what to make of the anterior-superior border of the T4(?) vertebra, which looks deformed with an arc-like sclerotic border, and in the region of the lower zone mass one of the vertebral arches seems sclerotic – perhaps just my imagination.
Good morning!
Bicameral pacemaker in situ
Wedge shaped density projected over the RLL.not silhouetting right hearst border or diaphragm. Well defined upper margin ill-defined lateral margin(extrapleural sign). Extra pulmonarylocation confirmed on lateral view.
morphology wise 1 or 2 but not very high density so can’t stop wondering whether 3
Will you say that it is correct to say “any of them?”
Hazy ill-defined opacity over the right lower zone on the PA view with thickening of the anterior pleura on the lateral view.
the findings are probably consistent with loculated anterior plerual effusion.
Widened upper mediastinum on the right with opacified retrosternal space in the lateral view, ddy anterior mediastinal mass. CT next.
Hello!
Since patient had a medical history (pacemaker) I would like to see previous X rays.
The mass is extrpulmonary and could be either a,b or c, but to me none of that explain the volume loss, so I’d go with d and suspect either sequestration or (less likely, because I don’t see pleural thickening) round atelectasis.
Either way I don’t believe it’s his first X-ray and I want to see the previous one!(either that or we’re doing CECT)
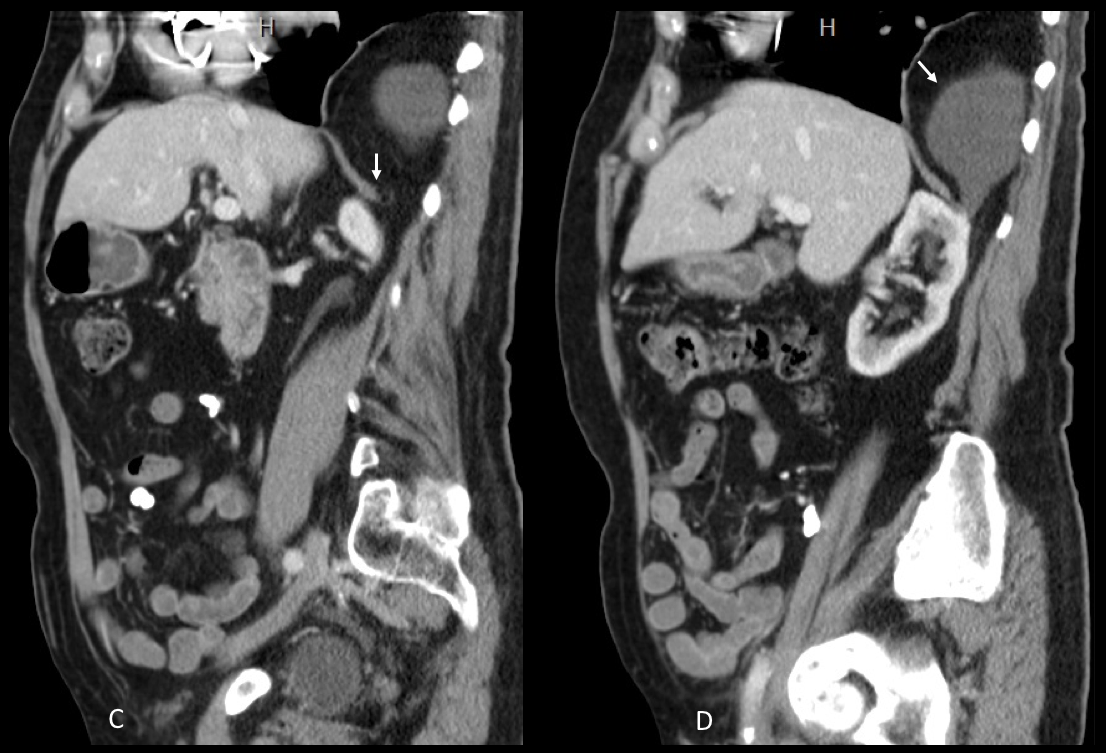
You are right about the diagnosis being a,b, or c. Need a CT to demonstrate the etiology.
I disagree with you about sequestration and rounded atelectasis: both of them are intrapulmonary and don’t have sharp borders (it could be an extrapulmonary sequestration, though, but they are infrequent)
Hi…this is my first time to participate in your intesting blog,…and here is what i see:
The right lower lung zone show relatively well defined radiopacity seen with well defined upper border and showing negative silhuoette sign with the right cardiac border, also it is seen at the lateral film projected over the right loer lung zone and with well defined anterior superior border and with relatively obtuse angle with the plueral surface (extra pulmonary) and seprable from the hemidiaphragm….so it is wither of plueral origin ( answer 2) or a posterior mediastinal mass ( may be of spinal) or posterior chest wall.
also there is radiopacity seen at the right paratracheal region seen with correlation with a radiopacity seen anterior and superior in the lateral film…?? another mediastinal or plueral lesion Vs lymph node.
-also there is a linaer atlectatic band at the left lower lung zone….
so i think its either 2 or 4 (posterior mediatsinal mass)…
thank you
Welcome to the blog! The answer is already posted, so you know what the lesion is.
The right paratracheal opacity represents the brachiocephalic trunk. I don’t think that you can evaluate properly the lateral view because the arms are on the way.
Hope to have you again on January 7th. with the next case 🙂