This week we’re presenting another case provided by my friend Jose Vilar: a 39-year-old woman with cough and moderate dyspnea.
1. Mediastinal fat
2. TB
3. LUL collapse
4. None of the above
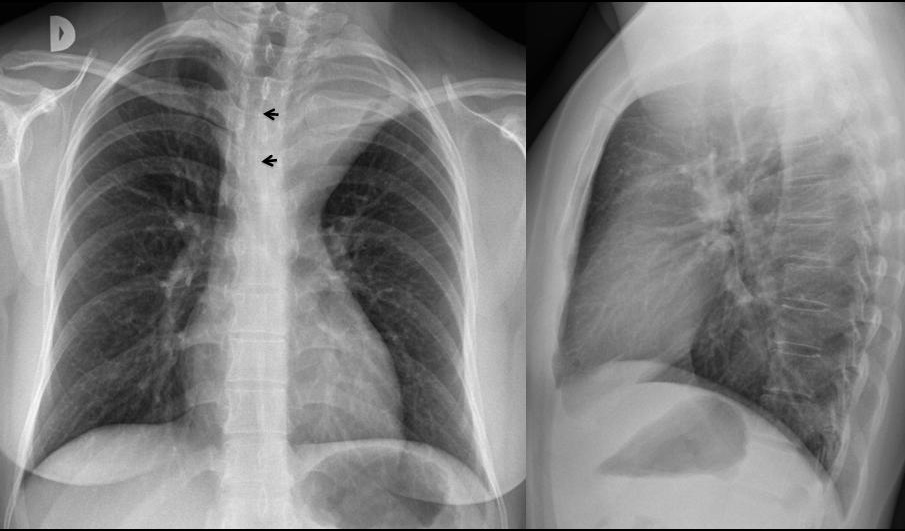
Findings: PA chest shows a well-defined left upper mediastinal mass. The mass is in the middle mediastinum and it is pressing against the trachea (
arrows).
It also extends into the posterior mediastinum as it reaches the top of the left apex.
The Lateral view is non-contributory.
A vascular origin for the mass would be a good guess, but there is another possibility: mediastinal fat, which is common, can appear anywhere, and can have a strange appearance.
Diagnosis is confirmed with CT, which shows that the findings in the plain film are due to mediastinal fat extending into the neck.
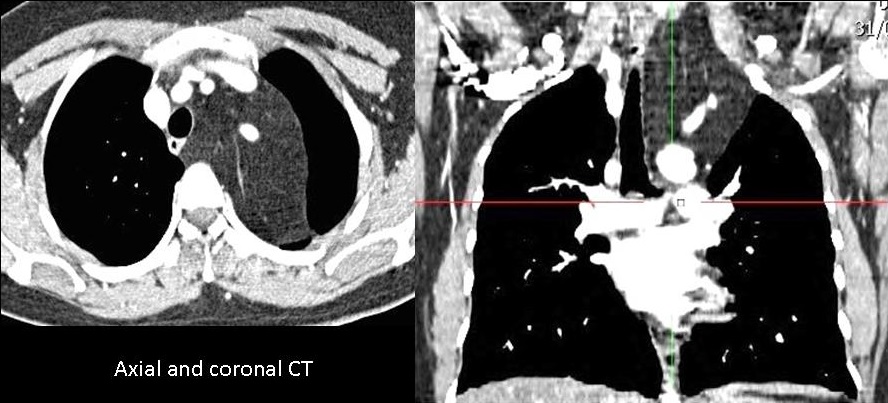
Final diagnosis: Mediastinal fat
Congratulations to Gus, who gave the correct diagnosis
Teaching point: Vascular lesions and fat may simulate other mediastinal masses. For this reason, all masses should be studied with enhanced CT.




chest x ray 2 views , tilted frontal view.
widening of the superior mediastinum , more to the left , there is a mass extending above the clavicle , so it is middle or posterior mediastinal mass , this mass is displacing trachea , silhouetting the aortic knuckle ,that is not seen in both views , i suggest this posterior mediastinal mass , vascular and high possibility of cervical aortic arch extending to the neck , rather than neurogenic tumor but i cannot explain sharp white line on the left margin of this mass , however CTA is advised to rule out aortic aneurysm on top of cervical aortic arch .
On AP view, there is widening of the superior mediastinum on the left with positive cervicothoracic sign and sharp borders suggesting a posterior mediastinal mass (neurogenic tumor? extramedullary hemopoiesis?). There is also obliteration of the aortic knob (positive silhouette sign) and deviation of the trachea to the right, suggesting middle mediastinal involvement.
On the lateral view, there is an opacity overlying the upper thoracic vertebrae and obliteration of the retrosternal clear space.
Hila and fissures in place. Does the patient has hoarseness? (left recurrent laryngeal nerve compression?). This could explain the symptoms (dyspnea and cough).
Cervical aortic arch is possible but I wouldn’t expect such a straight outer border.
I agree with you
We can’t identify aortic knob, what makes cervical aortic arch possible. Differencial diagnostics are posterior mediastinal masses as said above.
Extrapleural fat collection?
What makes you think it’s fat?
I am not sure if is fat.
I beleave is samething extra pleural on the left apical ,is not mediastinal lesion .
thyreoid mass
Opacità di massa, rotodeggiante ed a limiti netti (in LL) che impronta la parete posteriore della trachea , spingendola in avanti e verso dx(in AP). Data la sede di origine posteriore, io penso ad un ganglioneuroma. Per la DD,io avrei completato , in prima istanza, data la sede “accessibile” agli US con un ECD,escludendo così la natura liquida e-o vascolare della formazione..
Fat: not, because there is an important mass efect.
Tumor Thyroid not, too left and big, with out cervical mass. Lynphoma not. TBC not, to high. Aneurism: possible in the top of aortic arch. Thymoma very possible. Neurogenic tumor in adult I dont know.
Thanks Good¡ we have CT scan.
The only diagnosis I don’t like is thymoma. This lesion is not in the anterior mediastinum. All others are possible. Thanks God we have CT!
LUL collapse silhouttes aortic arch but the opacity here is extrapulmonary.
Nonhomogenous well defined rounded opacity noted on the lateral veiw projecting from the behind indenting the trachea & deviating it to the opposite side on the AP view. Slight scoliosis with convexity to the left also noted in the upper dorsal region.Not neurogenic tumor bcoz of absence of rib erosions or vertebral scalloping.
Possible diagnosis – extramedullary hematopoiesis / mediastinal fat
Good!
is there volume loss in the left hemithorax? if the answer is yes, maybe the left apical shadowing is due to partial left upper lobe collapse and the trachea is deviated to the right because the collapse is due to a bronchogenic mass causing mass effect. I don’t think the mass is posteriorly located as I think you can see an apical cup in the lateral radiograph.
don’t keep us waiting!!!!!!!!!
I believe the normal position of left hilum rules out LUL collapse. Apical regions are very poorly seen in the lateral view; the mass fills the apex of the left lung, which is evidence of posterior location.
Answer tomorrow. Can you wait?
Great case professor!! I have two questions.
1. Could we say that this looks more like a lipomatous tumor (lipoma?) than just mediastinal fat? (I would expect to see mediastinal fat also in the anterior mediastinum, the right apex, the costophrenic and cardio phrenic angles. )
2. Is mediastinal fat responsible for dyspnea and cough?
I believe differentiating mediastinal fat from a lipoma is a matter of semantics. Patients are not usually operated on and the lesion does not grow. The important consideration is that the lesion is benign.
As far as I know, moderate dyspnea and cough are mild symptoms, which may occur in many processes. Mediastinal fat (lipoma?) is not one of them.
Thank you professor.
golden reverse S sign… 3. probably there is obliterated bronshia by a santral bronch tm..