Dear Friends,
The Muppet is very happy with your responses to the previous case. As a prize, he wants to show you the following case that we saw together this July before he went on vacation with Miss Piggy (and left me working). Radiographs belong to a 46-year-old woman, with pain in the chest.
Leave your thoughts and diagnosis in the comments section below, and come back on Friday for the answer.
Diagnosis:
1. Empyema necessitatis
2. Chest wall tumour
3. Metastatic disease
4. None of the above

46-year-old woman, PA chest
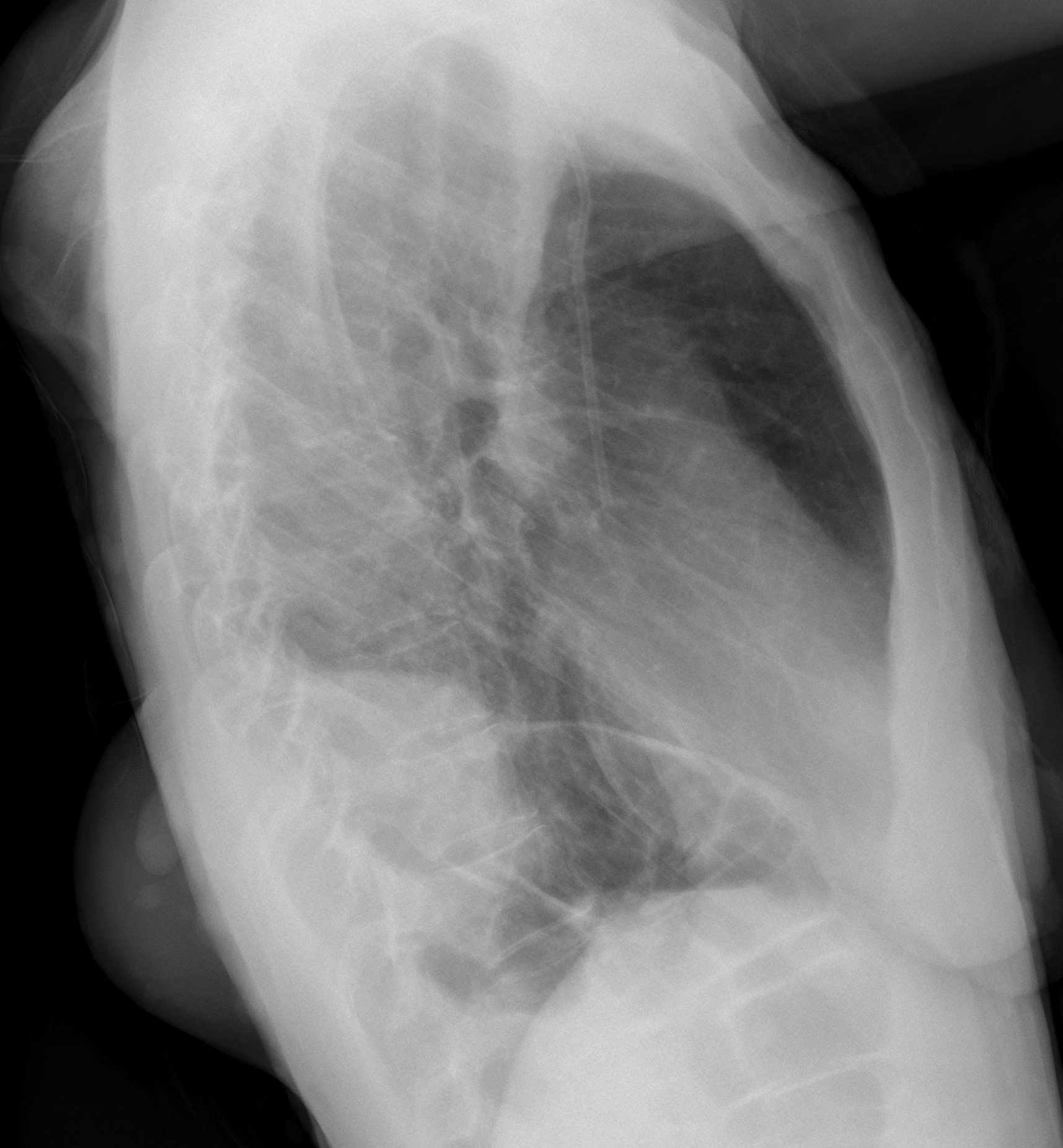
46-year-old woman, lateral chest
Click here for the answer to case #75.
Findings: lateral chest shows an inferior-posterior mass invading the soft tissues of the chest wall (arrows). There is a false mass above, which corresponds to the scapula (
yellow arrow). The PA view barely demonstrates the lower mass, hidden behind the diaphragm (arrow).
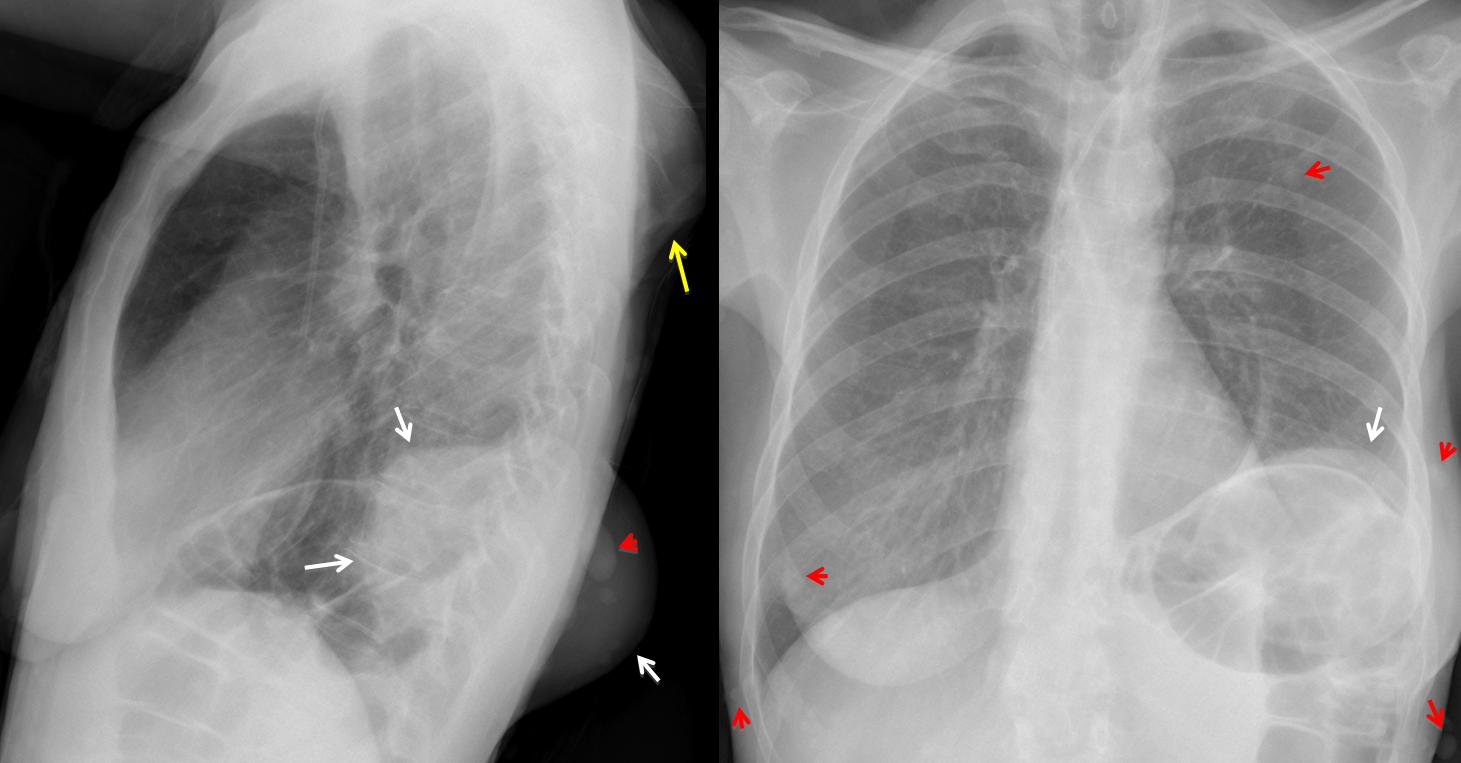
Fig. 1
The clue to the diagnosis lies in the numerous soft tissue nodules (red arrows), some of them projected over the lungs, simulating lung metastases. Findings are confirmed with CT (Fig. 2, arrows). This combination of skin nodules and a large chest wall mass is highly suggestive of neurofibromatosis with associated tumour.
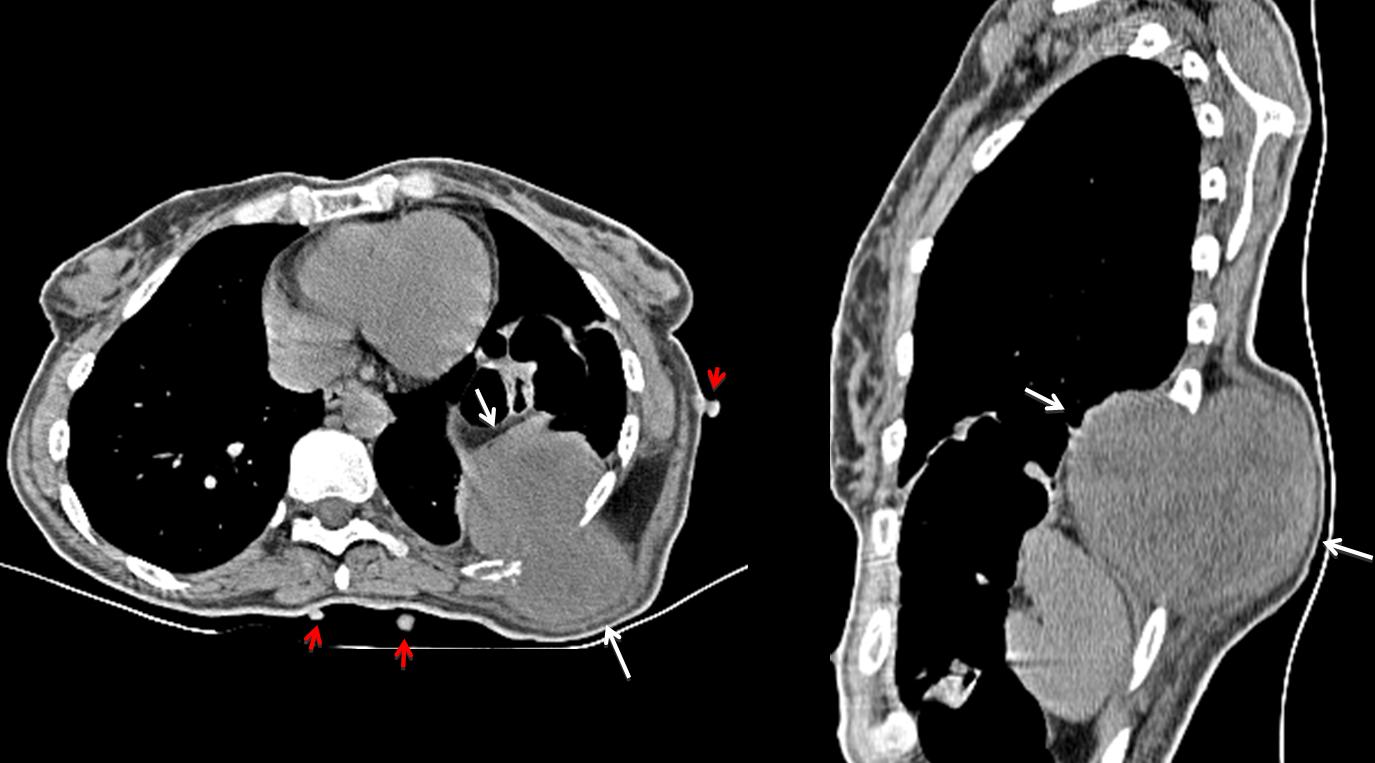
Fig. 2
Final diagnosis: Neurofibromatosis with neurofibrosarcoma of the chest wall.
Congratulations to Gus, who was the first to answer and to suggest the correct diagnosis.
Teaching point: always look beyond the obvious. Subtle findings may point towards the right diagnosis.


Chest wall tumor
We can see 2 masses in the posterior thoracic wall. one of them (inferior mass)is extending endothoracic.we can see also
(masses in the mass)and subcutaneous lesions.i can’t see very well the 9th posterior rib on the left (could be infiltrated? )
Port catheter. elevation of the left hemidiaphragm and the left hilum too.i think the hemidiaphragm is compressed from colon dilatation or from a peritoneal mass (both of them).
Scoliosis if the thoracic vertebrae. i can se a nodular lesion on the uper left (could be from the skin lesions). diagnosis later..
eventrated left hemidiaphragm..
the lower mass is finger like (!!!)is it a congenital anomaly..
The upper is bony but can be the same pathology as the lower one..( failed attempts of fetal formation )
NF-1?
A metastatic tumor ? I see a CVC, though I don’t see left rib anomalies…
NF1
2.chest wall tumor
Mmm..i think its multiple metastasis(breast ca?). I dont see the breast shadow in the left, there is pathologic IX rib fracture in the right, chest wall infiltation in the left and rib destruction. I can’t see very well, but i think there are met’s in the LUL; VII rib in the right ( it dosnt look like a nipple).
….nessuno si fa avanti….tutti aspettano le mosse dell’avversario per non scoprirsi e colpire in contropiede:sembra una partita di calcio contro i Blau-grana!!!! IO un’idea c’è l ‘ho…..attendo il 90!No, mitico professore, non ti abbandono!
Where is my answer??? :/
Sorry, I just got your previous answer five minutes ago. Problems with the server, I imagine.
I cannot give you specific leads; except that you did not mention the nodules in the soft tissues.
Im so sorry 🙂 its really something wrong with server.
P.S. I mention the nodules in the soft tissues in the next answer, but icant find it there 🙁
Don´t worry. The important thing is to have a lively change of opinions.
Exchange of ideas,sorry
I agree with the description of Gus.
I think that the destruction of the posterior part of the left 9th rib by the chest wall soft tissue mass is more suggestive of a malignant process.
In the diffential diagnosis we must also take into account the multiplicity of the lesions and the presence of round or oval dense lesions (calcifications?), both inside the lesions and subcutaneously all over the chest wall. They are seen in the posterior chest wall in the profil view and in the lateral chest wall, especially in the lower corners of the AP view, where we can also see bilateral fractures of the anterior part of 9th ribs (may be that’s why she is in pain).
A possible diagnosis is NF1 with malignant tranformation of the bigger soft tissue mass, but I think that soft tissue metastases cannot be ruled out.
Trying to figure out other possible diagnosis too …..
I would like to see the uncropped AP view to figure out what is the origin of the air collection that seems to be superimposed to the uppermost visible part of the trachea.
Dear Keterina, welcome back! The air that you refer to is between the sternocleid muscles (prominent in thin persons). The nodular lesions do not look calcified to me.
Otherwise, your discussion is excellent. Thanks. Muppet loves you.
I love the Muppet too !!!
Can you give us some more help to get closer to the diagnosis? Maybe another symptom?
Sorry. Only 24 hours more
Galattico, io penso che la risposta esatta sia la 3:malattia metastatica. La presenza del CVC e di metastasi(polmonare superiore sx e costali dx 7 e 9), nonchè la mastectomia sx, non lasciano presagire nulla di buono.Rimane quella massa della parete a sx: potrebbe spiegarsi con una recidiva metastatica della precedente costotomia della 9 costa ovvero un cattivo funzionamento del reservoir del CVC.Avrei subito completato con una eco(solido-liquido), lasciando ovviamente alla TAC la risposta finale.
…grazie professore per l’eccellente lezione….posso avere almeno le attenuanti generiche? Mi aveva fuorviato l'”apparente” mastectomia a sx- Barcellona -Bari 1 a 2…..alla prossima!
QX