This week I am presenting radiographs of a 78-year-old male with haemoptysis. Have a look at the images below and leave us your thoughts and diagnosis in the comments section. The answer will be added on Friday.
1. Hydropneumothorax in minor fissure
2. Tuberculosis
3. Carcinoma
4. None of the above
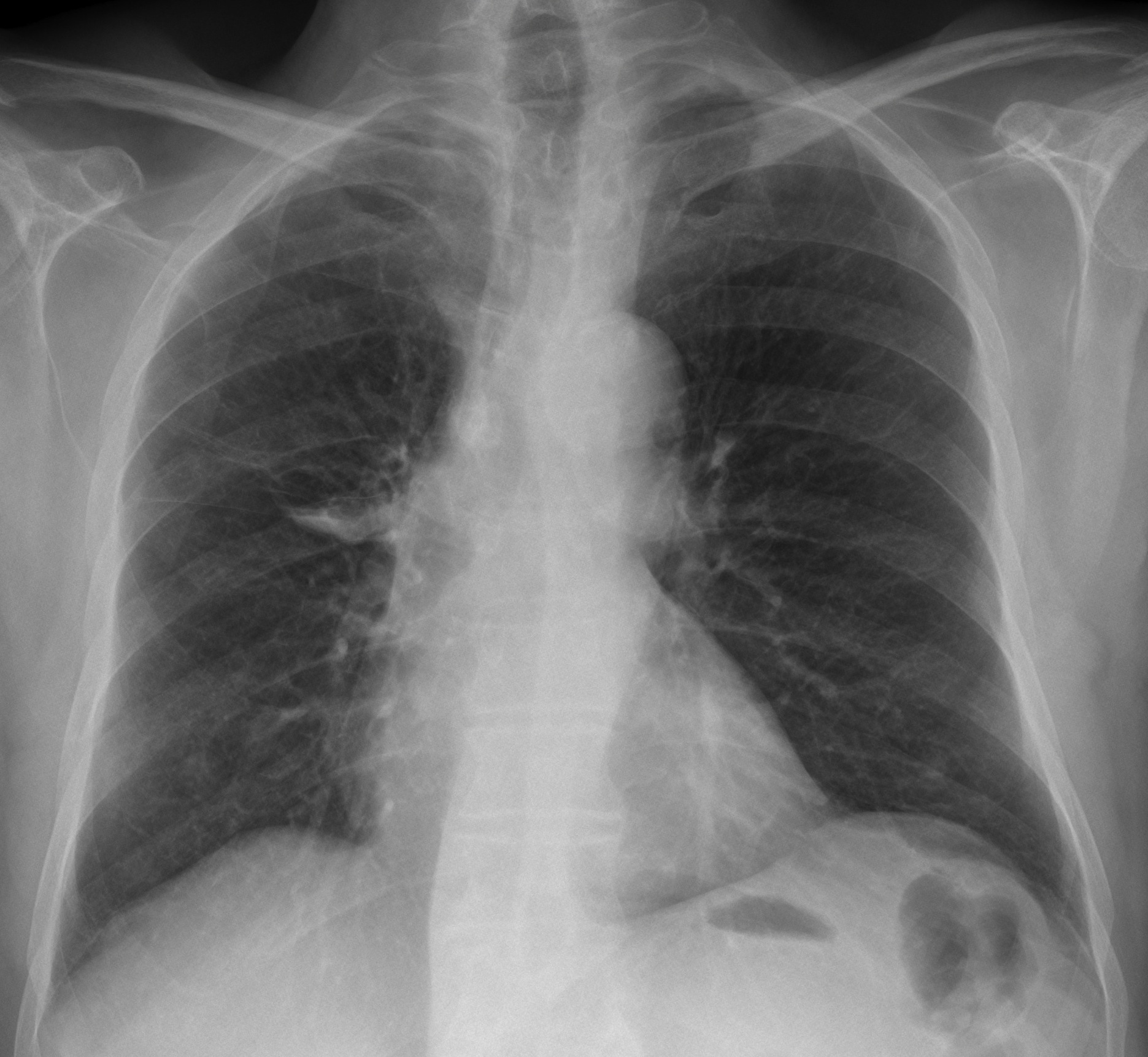
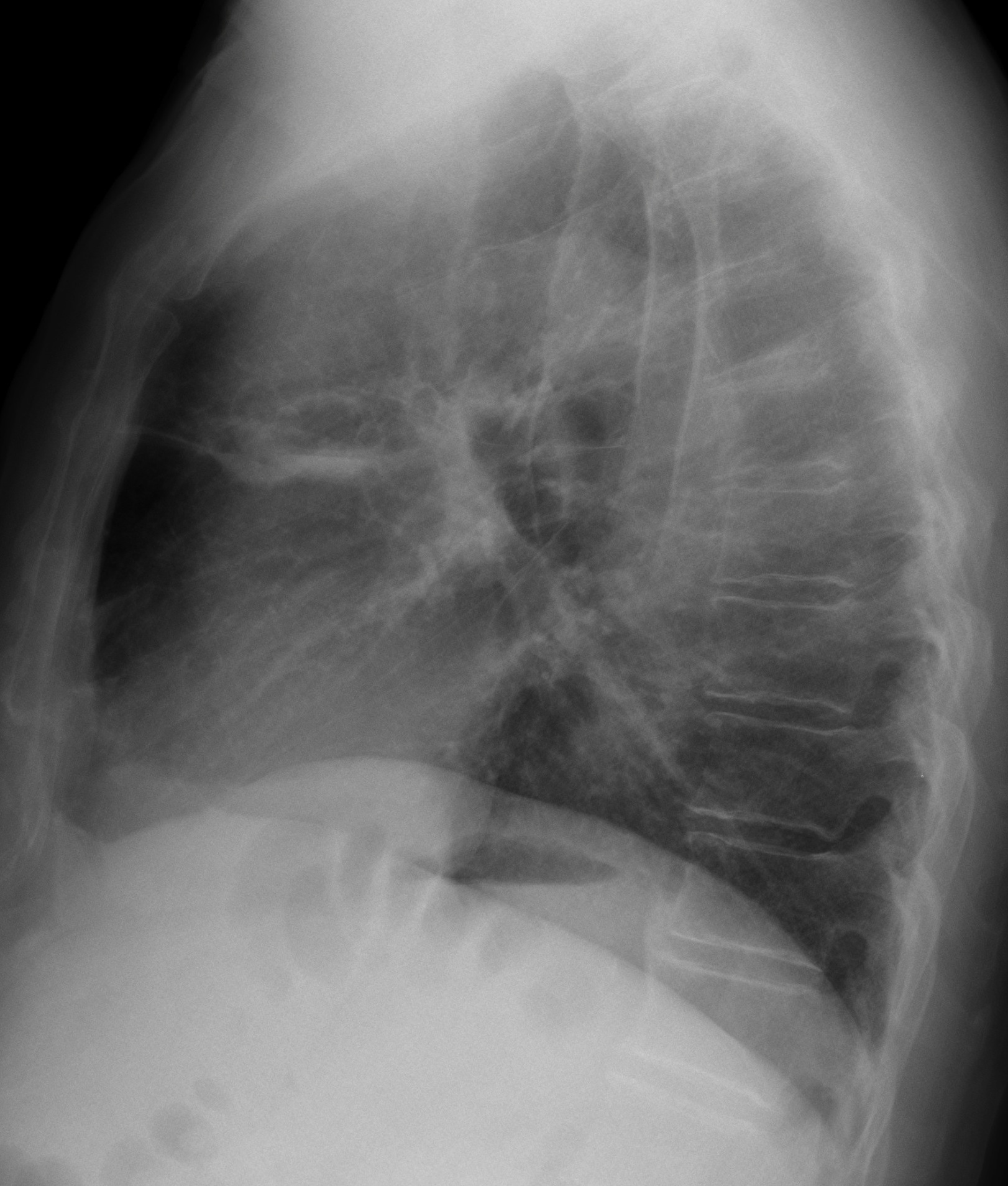
Findings: PA radiograph show a cystic RUL lesion with thin walls and an air-fluid level. On the lateral view there are several cystic cavities, at least two of them with air-fluid levels (Fig. 1, arrows).
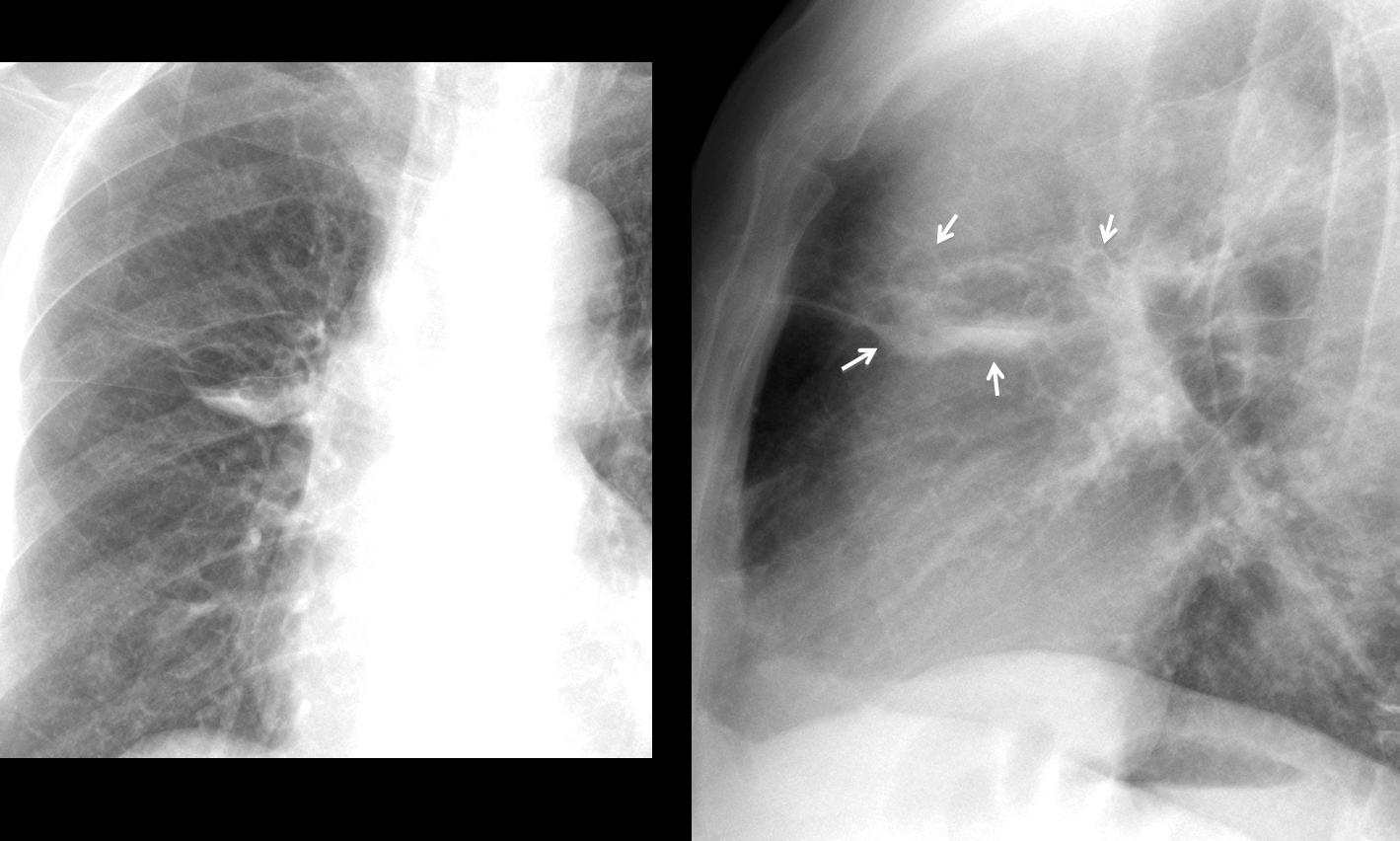
Fig. 1
The thin walls and the multiplicity rule out carcinoma and it is obvious that some lesions are outside the minor fissure, which excludes option one. The radiographic appearance suggests bronchiectasis, confirmed with axial CT (Fig. 2a, arrows) performed two years earlier. At that time, bronchiectasis were partially fluid-filled (Fig. 2b arrow), simulating a pulmonary nodule in the chest radiograph (Fig. 3, arrows).
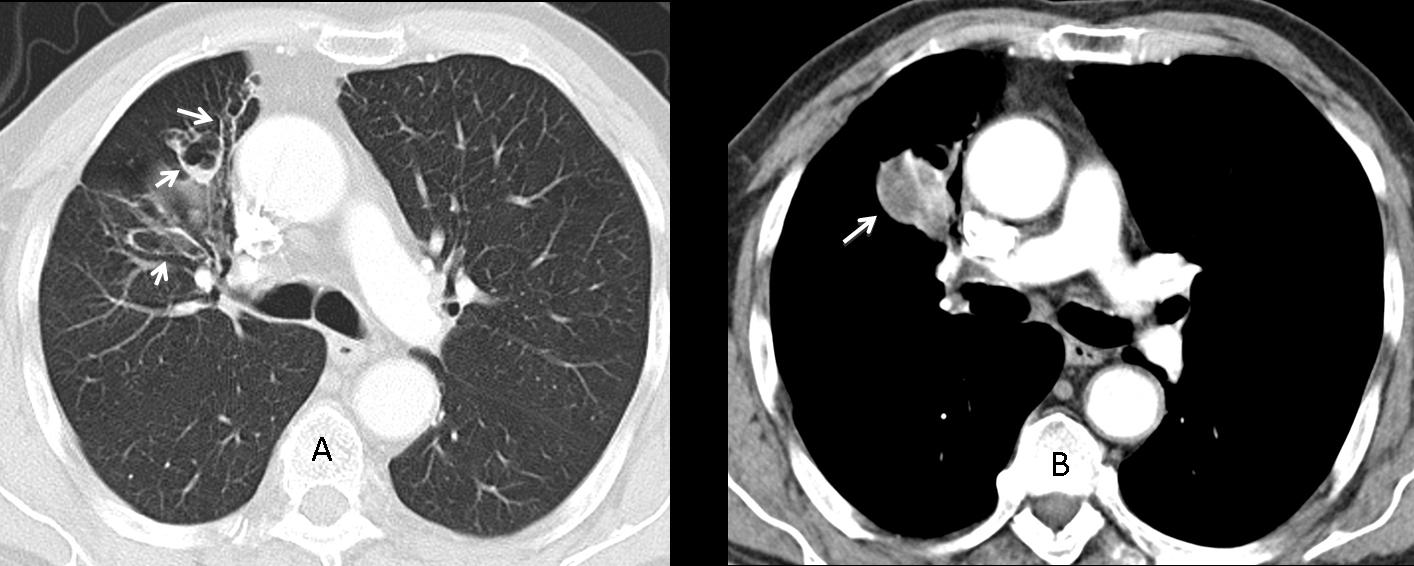
Fig. 2
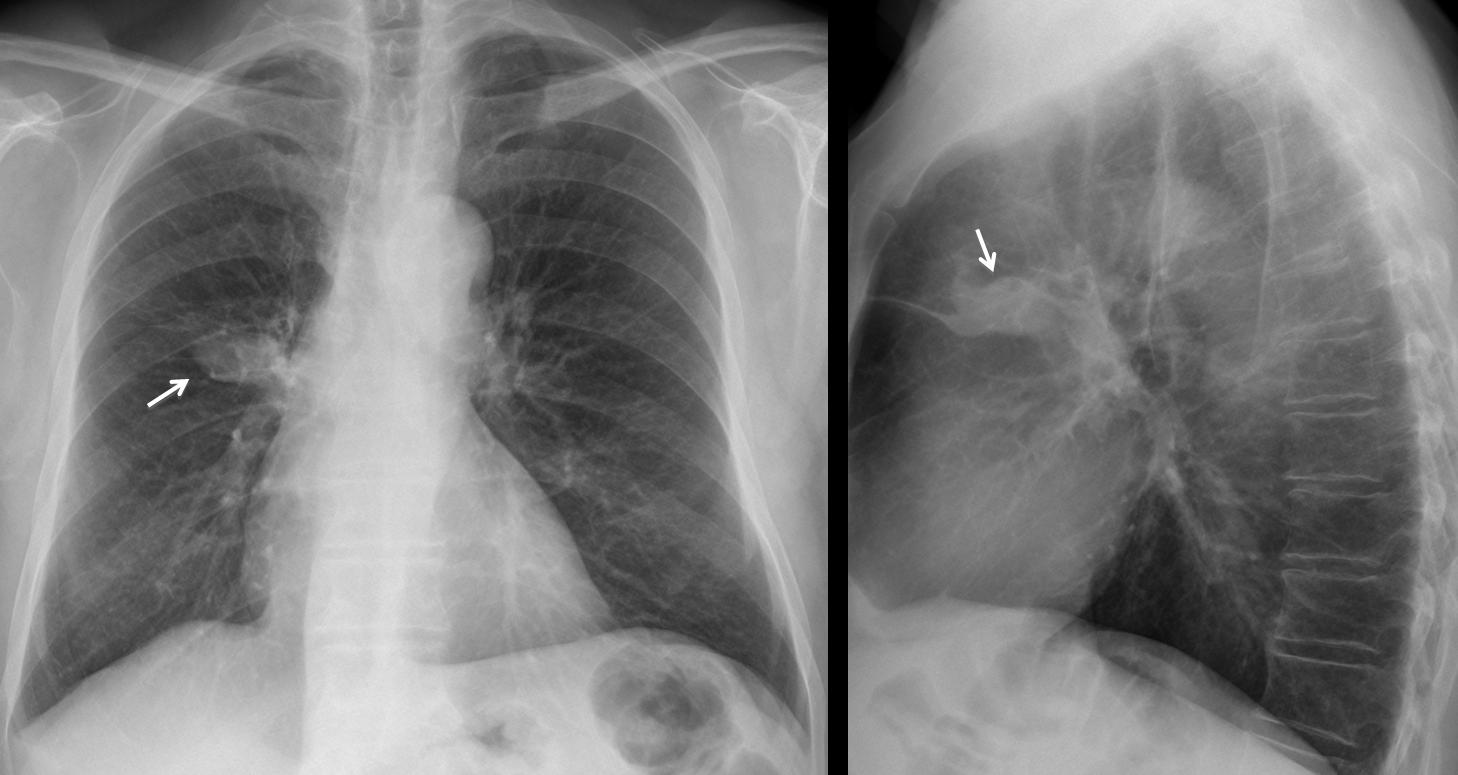
Fig 3. Two years earlier
Congratulations to Gus, who was the first to suggest the diagnosis, with Marcy as a close second.
Final diagnosis: cystic bronchiectasis, probably secondary to previous TB (not confirmed).
Teaching point: pay attention to details. In this case, the presence of several thin-walled cavities in the lateral view helped to rule out some of the proposed diagnoses and suggested the right one.


La cavità, con livello idroaereo ha sede intrapolmonare( si esclude il versamento pleurico saccato).Le pareti della cavità sono regolari e sottili( si esclude un CR-cistico).Non immagini adenopatiche ilo-mediastinic he( si esclude TBC). Potrebbe essere, in ragione dell’emottisi, un pneumatocele, post-polmonitico.
None of the above.May be Echinococcus cyst….
I think is more than one cavities with and with out air fluid levels. Pulmonary cavities may be the result of malignancy, infection, inflammation or be congenital
The frontal chest xray shows mild hyperinflation, and a coarse pattern in the lower lung fields consisting of reticular interstitial markings and central thin wall ring shadows with and with out air fluid levels suggesting cysts.
Apical pleural thickening.
I can’t observe mediastinal lymph nodes.
i think the cysts is bronchiectasis.
None of the above..it looks an intrapulomary thin walled ruptured cyst (DD:hydatid,bronchogenic cyst )
There is upwards position of right hilum with atelectatic changes of middle lobe. There is also some obliteration of retrosternal space. There is thickening of interstitial space of RUL. I vote for carcinoma.
There is loss of volume of the right hemithorax, indicating that a cronic process could co-exist. Moreover I see some round lucent structures in the RUL, that could represent bronchiectasis , additionaly there are at least to cystic lesions which contains air-fluid level in the upper lobe, contacting the minnor cisure , in my opinion due do bronchiectasis in the setting of a TB infection (because the location). As complication this patients could manifest with hemoptysis
cysts with airfluid level in rt parahilar region,
?complicated bullae / central bronchiectasis/ cavities
Non of the above , most likely Lymphangitic carcinomatosis .
Most likely Lymphangitic carcinomatosis .
Non of the above
There is loss of volume of the right lung, with the fibrous changes in the RUL which pull up right hilum. The right apex is blurred. Two cysts with air-fluid level are also prezent in RUL near hilum. The heart siluette seems bigger. I vote for Tbc (coexisting with cardiac insuffitiency)
There’s right fissural effusion (at right transverse fissure)with an atelectatic band is seen superior to it at the middle lung zone. Left pleural capping at left lung apex is also seen. I would go for TB suggestion. However, I recommend further investigation to rule out possibility of pulmonary embolism as I can notice subtle lucency difference between both hemothoraces.
How difficult is the chest radiograph¡¡
If you know the basics, not really!
Ok
Encysted hydropneumothorax in the transverse fissure
Encysted hydropneumothorax in the transverse fissure, i think so
ruptured cyst with air-fluid level associated with fissural effusion. i vote for TB