Dear Friends,
Muppet saw this case while looking at daily chest radiographs and it caught his attention. We looked at the patient’s history and found that she was a 64-year-old female with back pain, who had a well-differentiated liposarcoma removed from her right thigh seven years earlier.
Do you see anything?
What do you think it is?
Check the images below and leave your thoughts in the comments section. The answer will be posted on Friday.

64-year-old female, PA chest

64-year-old female, lateral chest
Click here for the answer to case #78
Findings: the PA radiograph shows a double contour of the aortic knob (arrows). It does not obliterate the aortic contour, indicating a mediastinal mass in front of or behind the aorta. The lateral view shows increased opacity over the middle vertebra (circle), suggesting a posterior location.
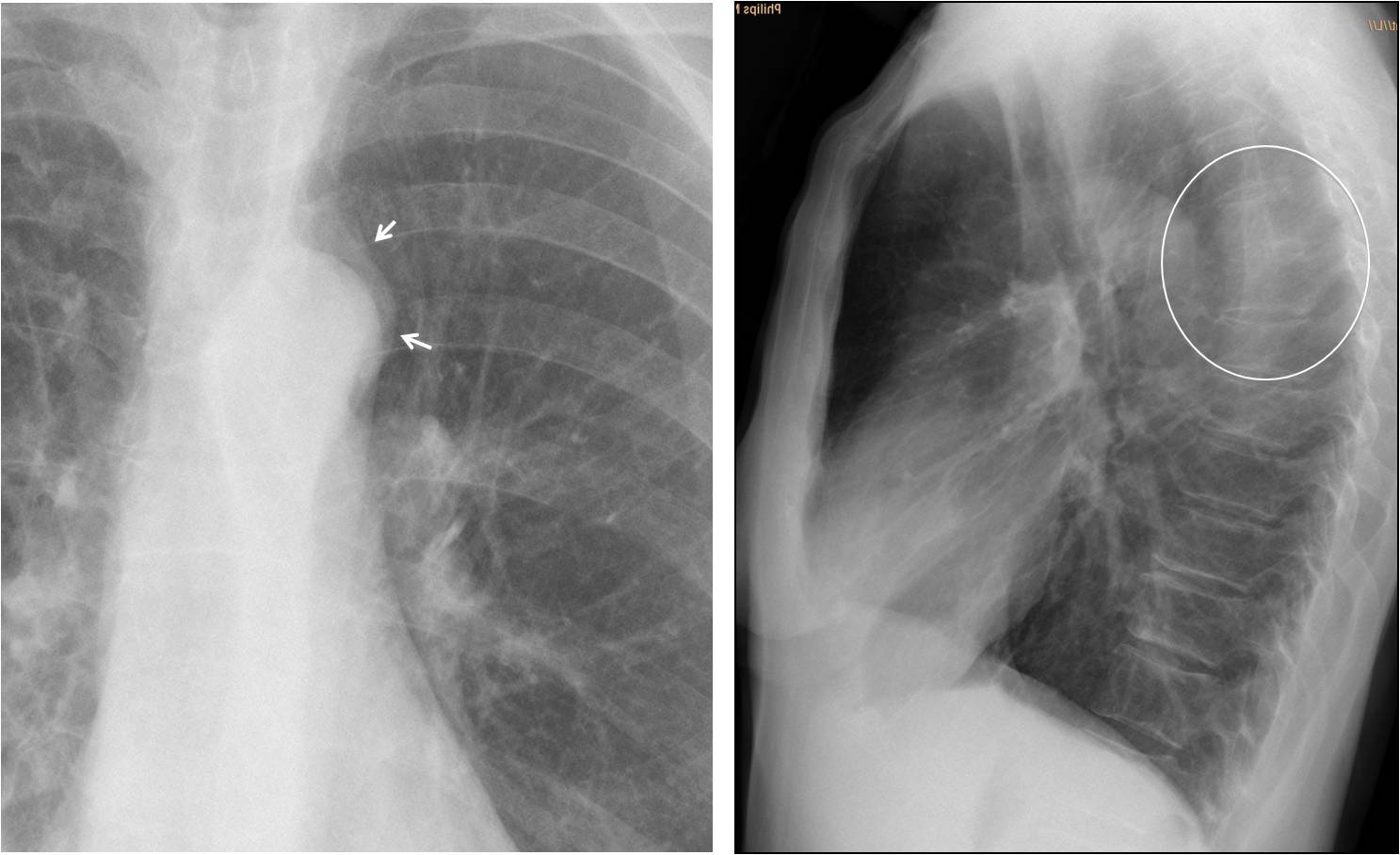
Fig. 1
Coronal and axial CT demonstrate a posterior mediastinal soft tissue mass (arrows). Without the clinical history I would have suspected a neurogenic tumour. However, MRI shows involvement of the adjacent vertebra, making metastases more likely.

Fig. 2
Final diagnosis: vertebral metastases from liposarcoma, surgically proven.
Congratulations to Martita, who made a brilliant diagnosis. Muppet elated!
Teaching point: it is my impression that the majority of us look mainly at the lungs and forget about the remaining structures of the chest (not Muppet, though). So, remember to look carefully at the whole chest. This case was discovered because the plain radiograph looked abnormal.


There is a density in the right apex (paratracheal region). It could be a metastasis. Thorax ct would be the next step.
There is a density in the right apex on tha frontal view but nothing on the lateral view.
1 i see conection between density and clavicle, could be a normal variant mimicking pathologie (accessory rib for example)
2 could be a soft tissue metastasis. i see a soft tissue density on the upper posterior thoracic wall but we can t see it very well (only a portion)
A cervical spine Rx and physical examination is recommended.
or sternocleidomastoid muscle in my first choice.
Bone met? Highly calcified lesion at LSB
– It seems to me that there is a nodule in the AP view projecting over the posterior part of the 8th right rib, which I can’t discern on the profil view (liposarcoma metastasis?).
– Breast asymmetry (previous left breast surgery?).
– The first density on the right apex must be due to the sternocleidomastoid muscle although unilateral and the second density (paratracheal region) must be of vascular origin.
Saggy breast may became asymmetric when pressed against the X-ray plate.
There is no nodule in the right lower lung.
Professor i see a tubular structure with air pericardiac on the right it looks like bowel. is mine imagination? morgani?
Your imagination. Don’t insist in the right apex. There is nothing there.
I think osteoporosis can explain the pain. Osteodensitométrie and CT should be next step
The dorsal part of the 9th rib on the right side doesn’t show the same continuity as the 9th rib on the other side.
With the history of liposarcoma the back is a typical location for that tumor.
Where exactly is the back pain located?
I would perform an ultrasound of this region – if inconclusive CT of the thorax.
dense descending aorta could be due to atherosclerosis plaques
I can see a double outline at aortic arch in PA projection and a density on some of the dorsal vertebra, behind the aortic arch in the lateral view. The density is suggestive of fat because it’s lower than the typical soft tissue density. So, i think it is most probably related with her history of a removed liposarcoma 7 years ago.
Excellent! Muppet loves you!
Only one comment: I don’t believe it is possible to see fat density in the chest. It does not mean that you are wrong, though.
Hmmm…i dont like the upper third of trachea and retrotracheal space :/
So far, nobody has noticed the finding that called Muppet’s attention. You have two more days until Friday. Keep trying!
The heart size is normal but we can see dilatation of the hilum pulmonary arteries.(emphysema?-Pulmonary hypertension?)
There is posteriolateral shift of the trachea on the right that means there is a stucture on the anterior space of the trachea.
– dilatation of pulmonary arterie for some reason?
– Ascending aorta dilatation?
– metastasis of pericardium?(history of well-differentiated liposarcoma rearly metastasis in general…)
-i feel stupid.
Only one and a half days left. Has anybody looked at the aortic knob?
In AP vi è un cappuccio rx-opaco, sopra l’arco aortico;inoltre allo stesso livello la trachea è improntata sul lato sx e sospinta leggermente verso la linea mediana.In LL si coferma allo stesso livello una impronta posteriore sulla trachea, anche lievemente anteriorizzata.Diverticolo di Kommerell?
Paraspinal/mediastinal soft tissue density overlying aortic knuckle – may represent neurogenic neoplasm /metastasis/aortic aneurysm.
Good reasoning. Pity you are late. Still, congratulations
aberrant artery in the left? 🙂
Excellent case Professor !!!!
There is a mild anterior wedging of dorsal vertebra D5