This week I am showing you a case provided by my good friend Dr. Jordi Andreu. The radiographs below belong to a 39-year-old woman with increased shortness of breath for the last three months. Leave your thoughts and diagnosis in the comments section and come back for the answer on Friday.
1. Bullous emphysema
2. Tension pneumothorax
3. Adenomatoid malformation
4. None of the above
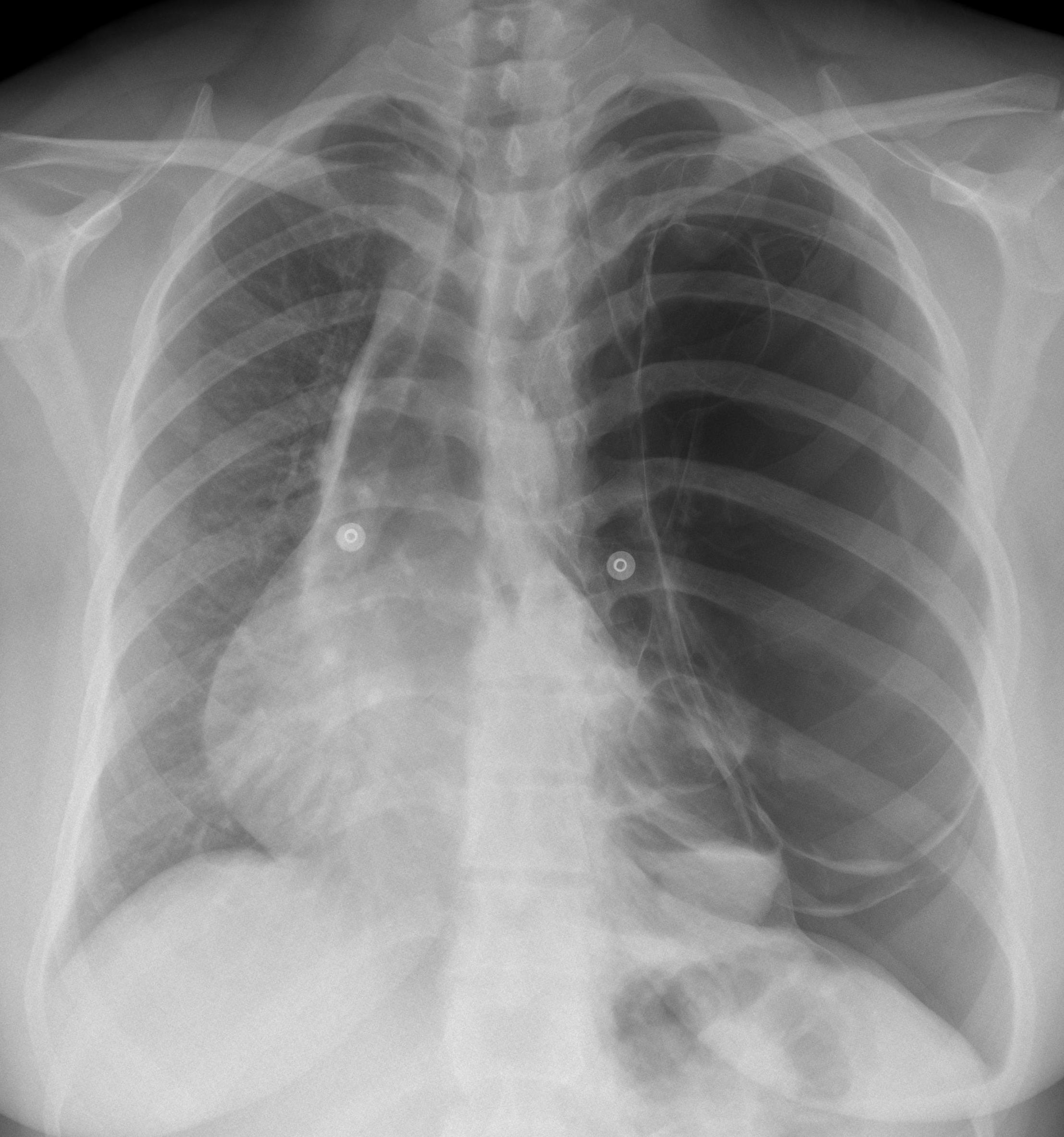
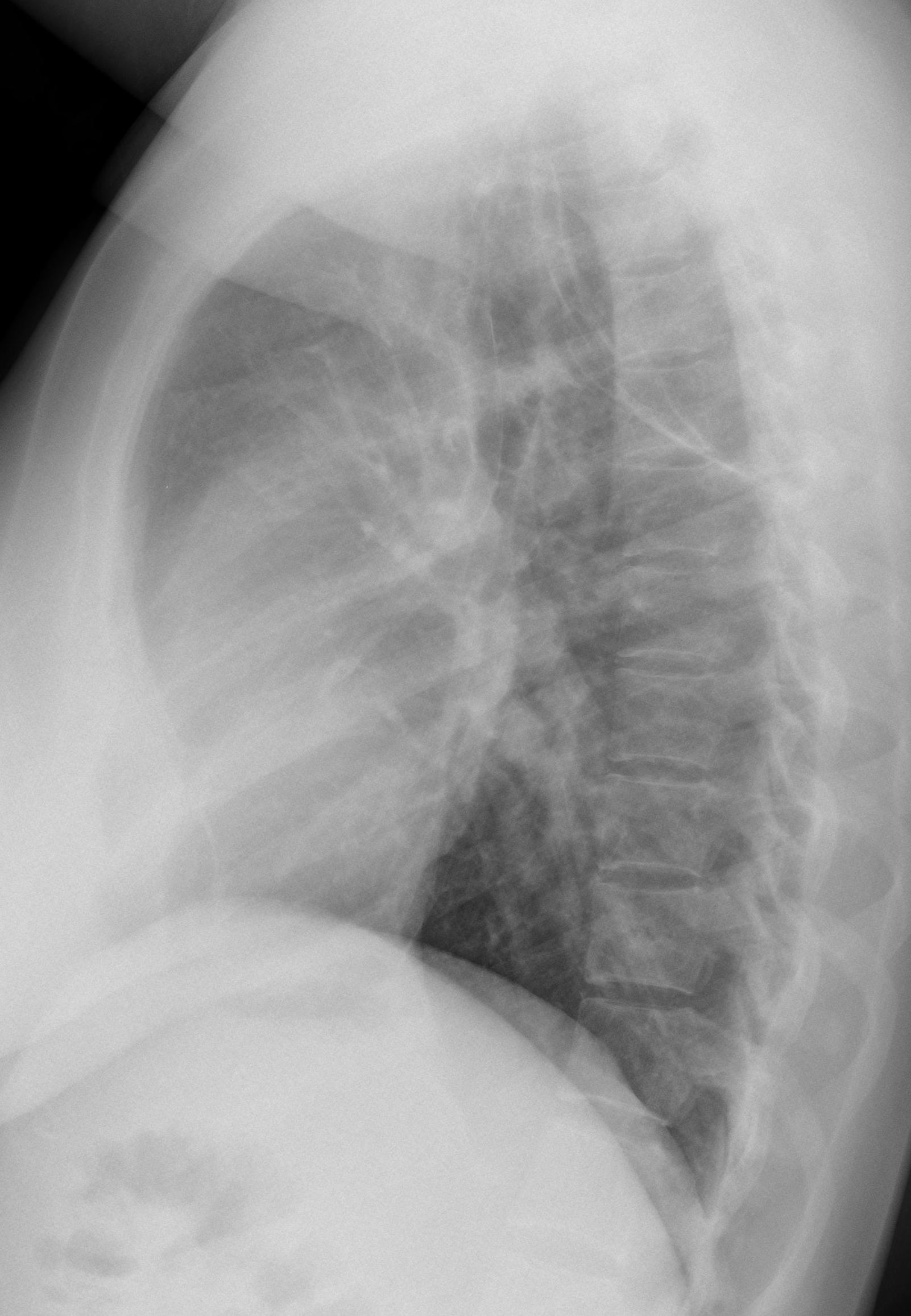
Findings: PA chest shows an expanded hyperlucent left lung with displacement of the mediastinum towards the opposite side. The left hemithorax is occupied by several thin-walled cavities (arrows), one of them with an air-fluid level (
red arrow). The lateral view does not provide any additional information.
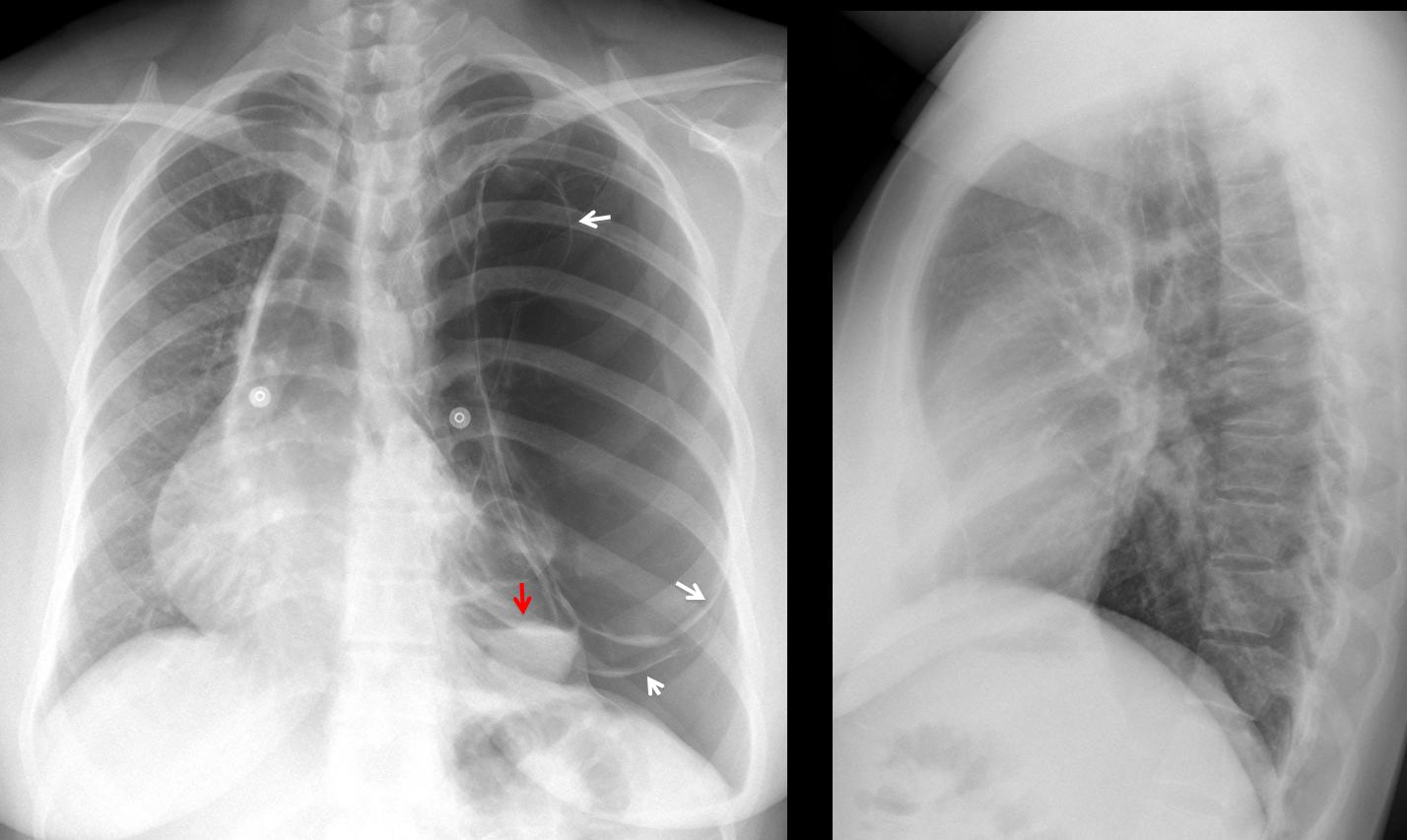
Fig. 1
Axial and coronal CT show several thin-walled large bullae; one of them with air-fluid level (Fig 2, red arrow). There is a small pneumothorax with some fluid as well. The left lung is collapsed (ryellow arrows). The right lung looks normal.
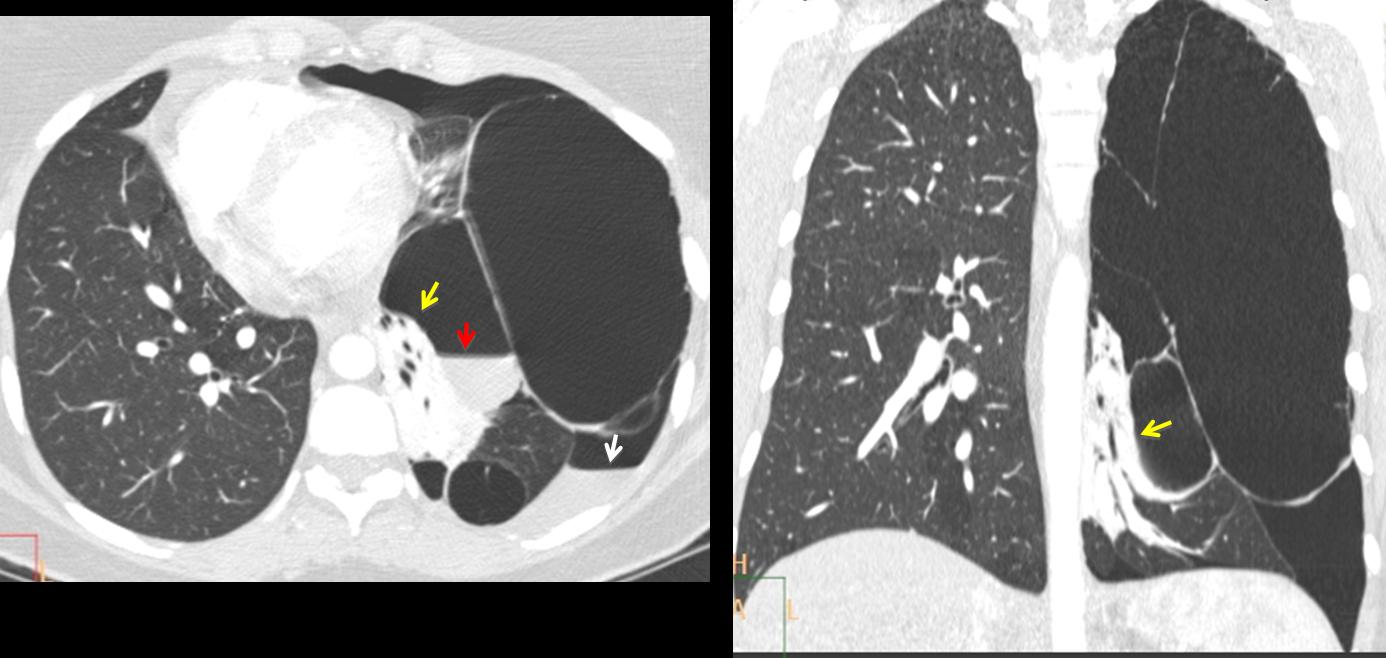
Fig. 2
This is a difficult case and the main differential diagnosis is between giant bullous emphysema and congenital cystic malformation. I consider tension pneumothorax very unlikely because the walls of the bullae are rounded and not flattened. The patient was operated on and the final diagnosis was unilateral giant bullous emphysema (vanishing lung syndrome). Post-op radiograph shows a near-normal appearance of the chest (Fig. 3).
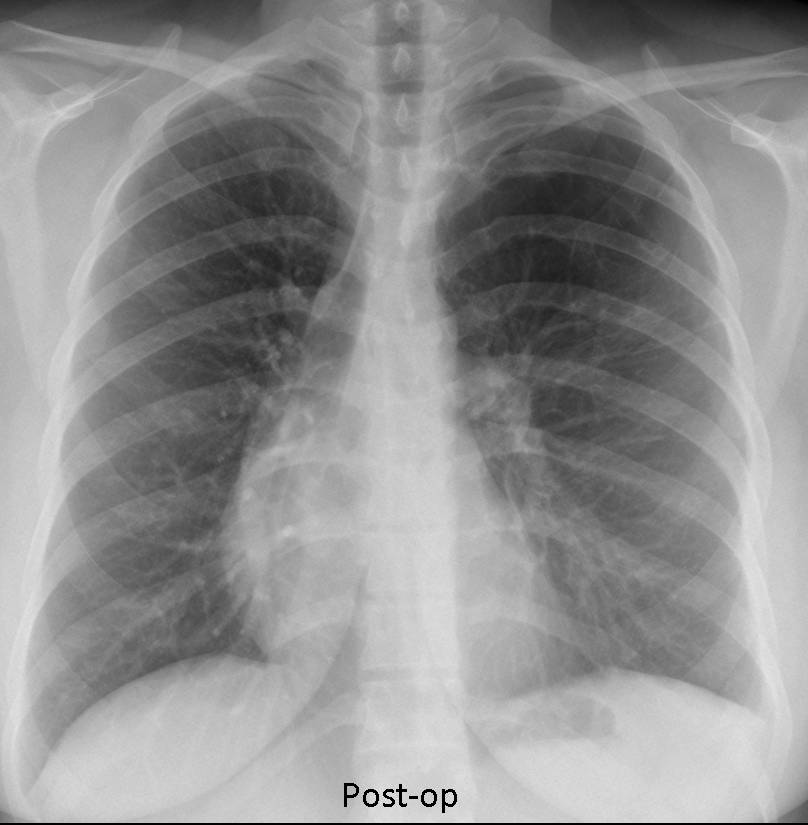
Fig. 3
I think most of you contributed with excellent discussions, but I will single out Dr. Sameh Khodair for his prompt and accurate answer.
Teaching point: this case represents an unusual cause of unilateral hyperlucent lung and complements case 47 of Dr. Pepe’s Diploma to be posted next Monday. Interesting to note that young patients with giant bullous emphysema are predisposed to lung cancer. I have personally seen three cases.


Nice to see you Dr. Jordi Andreu
I see a large emphysematous bulla crossing the mid line superiorly with another small one in the lower left hemithorax, associated pneumothorax with underlying segmental collapse as well as shifting the mediastinum to the contralateral side ( tension pneumothorax )
Don’t you think that a tension pneumothorax would collapse the bullae?
Its wall may be adherent the lateral chest wall
You don’t really believe that, do you?
really I cant believe…:)
but in the same time I had no previous chest imaging for that patient, I dont know if he submitted before for surgical interference as pleurocentesis, However, I see multiple emphysematous bullae of variable sizes with contralateral mediastinal shift, but i am not sure about pneumothorax, but still expect it in the subsequent CT chest of this patient
LARGE BULLOUS EMPHYSEMA
Carissimo professore. Non può essere una bolla enfisematosa, perchè l’enfisema polmonare è bilaterale ed in questo caso il polmone dx è sano.Certo vi è un pn-torace( e pn-mediastino)ipertensivo per lo shift a dx dell ‘ombra cardio-mediastica, l’abbassamento della cupola diaframmatica sx e l’allargamento degli spazi intercostLI, MA TUTTO QUESTO è DETERMINATO DALLE CISTI(NON BOLLE, A CAUSA di una parete spessa) di cui almeno una in basso presenta un livello idroaereo, segno di infezione sovrapposta ) per cui penso ad una MACC tipo 1 di Stolker) , complicata da infezione e rottura di una cisti.La MACC è tipica dell’epoca fetale neonatale, ma talvolta, perchè asintomatica, può presentarsi in età adulta a causa di una complicanza.Con la stima di sempre.
…ad una revisione critica,lo shift cardiomediastinico verso dx, potrebbe essere dovuto ad un enfisema ” lobare congenito”, che nel corso degli anni, iperinsufflandosi, con un meccanismo a valvola ha condotto ad atelettasia del lobo polmonare omolaterale e spostamento del mediastino .La patogenesi dell’enfisema lobare congenito riconosce cause che sono del tutte “differenti” da quello acquisito:ecco perchè, il dosaggio dall’a 1 tripsina può essere nella norma.
Multiple Left emphysematous bullae shift of mediastinum to right. One of the bullae is infected with air fluid level.
Bullous emphysema
Bullous emphysema-tension pneumothorax
Congenital pulmonary airway malformation type I
(involvement of an entire lung in an adult is extremely rare.)
Adenomatoid malformation
3 Adenomatoid Malformation
an other hypothesis is, Giant Bullous Emphysema (Vanishing Lung Syndrome)but these is bilateral,usually asymmetric lung involvement and often seen in young men.(fit in with age)
maybe there is a small bullae on the right lung that we can’t see.
A CT is necessary.
Can vanishing lung syndrome be unilateral?
CT will be shown Friday
yes professor it can be.
The patient’s alpha-1 antitrypsin level was normal?
I believe the alpha-1- antytrypsin was elevated. Will check the chart and get back to you.
Large emphysematous bulla with contralateral mediastinal shift
There are multiple wall thin cystic lesions, some of then have air-fluid levels. It is causing mediastinal shift toward the right side. It call my attention, that the right hemithorax is almost normal.
It has to be either a unilateral pathology as Adenomatoid marformation or a pulmonary sequestration, which are rare at this age, usually they are diagnosed in childhood. OR ,I would say that maybe this patient had undergone to right lung transplant, and what we see is sequela of a bilateral patology as cystic fibrosis, alpha 1 AT deficiency, etc
No previous surgery
Bolous emphysema
Another Vote for Bullous Emphysema, vanishing lung syndrome.
Young patient, proggression in symptoms. It may be unilateral. Mediastinum shifted.
Am I correst seeing on lateral chest Xray that bullae are mostly in upper and anterior location of left hemithorax? (upper lobe – feature of vanishing lung)
Youu are correct
Professor, we are waiting for CT:)
Did I miss it?
We have 1) increased shortness of breath for the last three months. NOT A TENSION PNEUMOTORAX (rapidly instaured )
2) increased volume Left lung + costal spaces (non an acute process)+abbasament left hemidiaphragm
3) not so thin walled (less than 1mm air filled spaces).
NOT A BULLOUS EMPHYSEMA BUT A LATE PROGRESSIVE EXTENSIVE ADENOMATOID MALFORMATION ?
4) at the left paracardial-anterior space over the left hemidiaphram . INFECTED CYST OR INFECTED AIR CONTANING EXTRALOBAR SEQUESTRATION ?
5) conservation of the principal bronchs (smaller angle?
=rotation ? =pression oh trachea? ) and contralateral mediastinal shift. Shortness of breath caused not by vessels sofference but by expansive left lung process. Right lung has no signs of important sofference.
Einblutung in Emphysembulla links infrahilär und basal mit Spiengelbildung. Verlagerung der Trachea und des Herzens nach re..
Pneumothorax bei rupturierter Bulla.
air lung cysts and adhesive pleursy?