Muppet believes that the last week of the year deserves an unusual case. Images belong to a 61 year-old woman with frank haemoptysis for one week.
What would you say about the LLL lesion? Leave your thoughts and diagnosis in the comments section and come back on Friday for the answer.
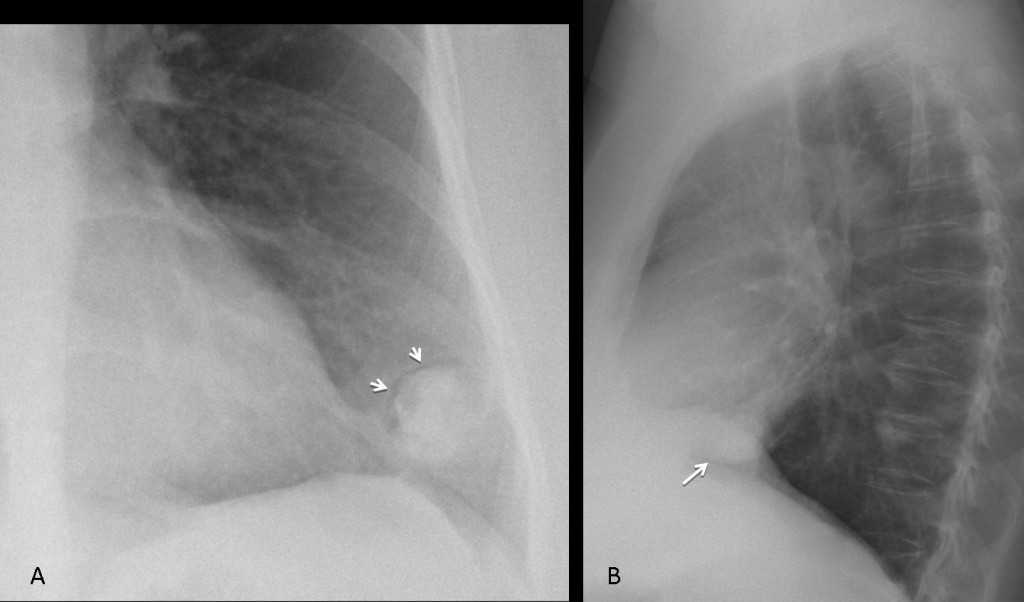
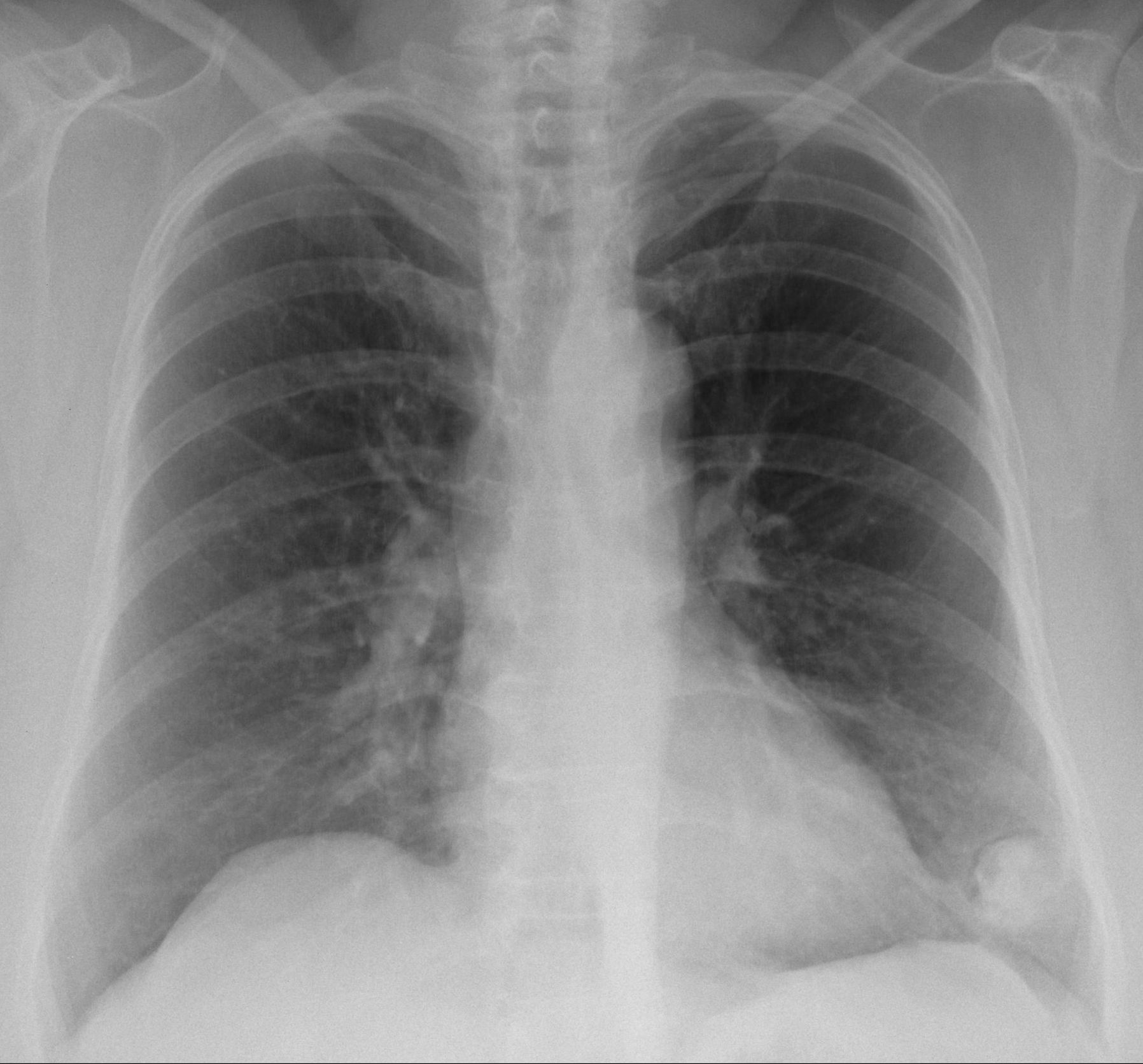
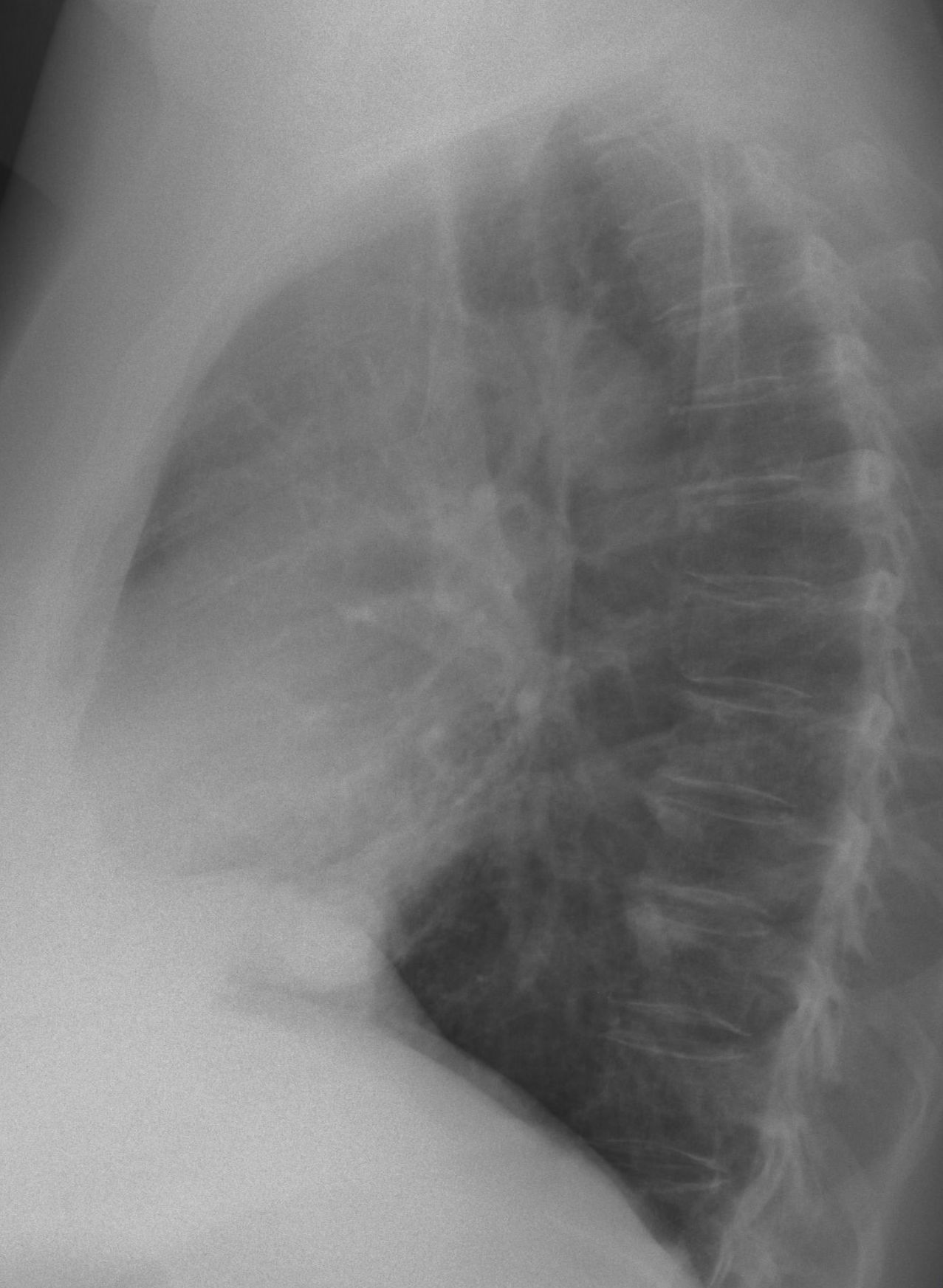
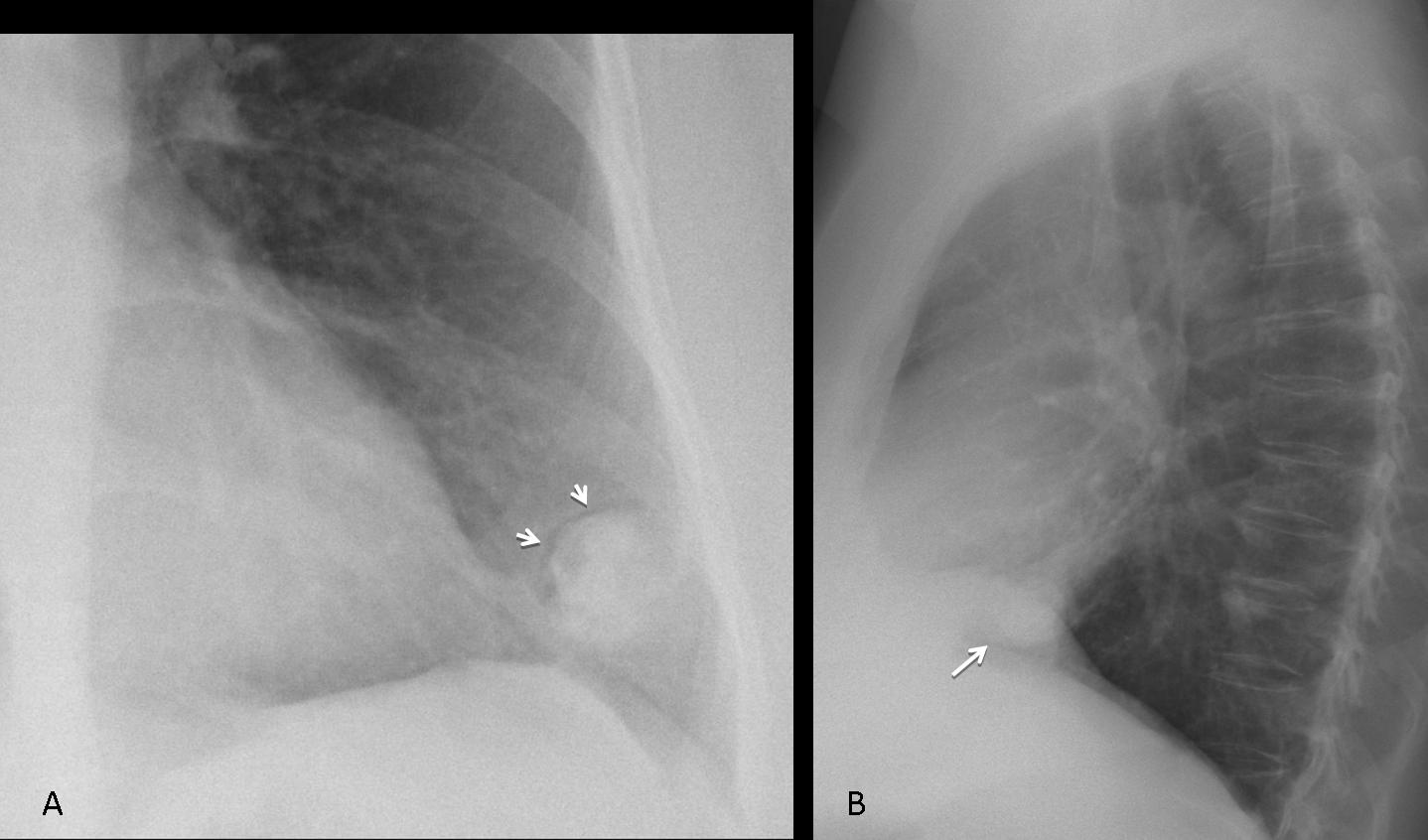
Findings: chest radiographs show a rounded lesion in the LLL with a visible crescent sign (A, arrows), indicating an occupied cavitary lesion. On close inspection, the cavitary content appears dense, suggesting that it may be calcified.
Coronal and axial CT confirms the air crescent (arrows) and a large calcification inside a cavity.

Final diagnosis: cavernolith
A cavernolith is defined as a calcified mass inside a lung cavity. Accepted etiology is a previous aspergillosis, which calcify with the passage of time. The pre-existing cavity is usually related to previous TB.
As you can imagine, this is my first and only cavernolith, which probably makes me an expert, since this is a rare finding. The interesting fact is that I saw this case four years ago, in 2009. The patient came to the ER with haemoptysis and the lesion was found. She refused surgery and was treated symptomatically. The haemoptysis disappeared and the patient has remained well since. A CT scan in 2013 did not show any change.
Congratulations to Lola la Piconera who made the diagnosis and to Genchi Bari, who pointed the way.
Teaching point: recognising the air crescent sign indicates a cavity with content and narrows the differential diagnosis. Perhaps in the future this sign will help you to diagnose your own cavernolith!



…”crescent air sign”:opacità polmonare contornata da immagine rx-trasparente a forma di mezzaluna.Si osserva nei processi di necrosi polmonare nelle fasi di risposta immunitaria al focolaio di necrosi, da parte dei granulociti.Aspergillosi invasiva e semi-invasiva, nonchè in altre condizioni più rare(TBC-Aneurisma di Rasmussen in tbc,ascesso polmonare ed infezione da pneumocistys Jrovenecj).Auguri di buon anno…..intanto il Bari vince in traferta per 1 a 0 a Novara…
You started all the young people thinking. Congratulations and Happy New Year.
…Galattico professore…il Bari non demorde….fallito l’attacco centrale ora si sposta sulle ali….grazie al tuo aiuto….la densità del nodulo …essa è alta e disomogenea….allora penso se i c-ANCA sono elevati ad una vasculite di Wageners….essa si manifesta con noduli polmonari, senza predilezione di sede, con possibile cavitazione del nodulo ed “halo-sign” alla TC.Deformato il soma di D12(x osteoporosi)
Ooooh!The shoot went wide…!
No goal this time!
…Happy new year…you’re simply the best, Professor!Mi dici se almeno il”crescent air sign” è esatto? Oppure devo rivedere la semeiotica di base….tra le altre cause, molto rare,del segno , ci sono la bronchectasia cistia e la plomonite, lipoidea circoscritta? Mando in campo le riserve?
Guessing…Pulmonary hamartoma or AV malformation?
Bad guess ;-)). I believe the air crescent sign (Genchi Bari dixit) eliminates AV malformation. Hamartoma cannot be excluded, but the last week of the year deserves a better diagnosis!
Av malformation?
See comment above.
DD: av malformation/pulmonary sequestration/hamartoma?
In the LLL there’s a nodule with “air crescent” sign, typical to a cavern with aspergilloma. The cavern might indicate the Tbc, but the location is wrong. There are larger lymph nodes in the left hilum. I can see 2 small nodules in the posterior segments of the LLL. I`m guessing that it might be metastases or sarkoidosis- but I suppose in these conditions changes should be bilateral…
Happy New Year Proffessor! Hope to see lots of unusual cases next year:)
Happy New Year. If you want unusual cases, wait until you see the diagnosis in this one!
i agree with mila and genchi bari italia
In the LLL there’s a nodule with “air crescent” sign the location is not typical for aspergilloma but it can be in any cavitation.
the location make’s my to think about aspergilloma in a pulmonary sequestration cavity or a pulmonary hydatid infection but first of all must to exclude the diagnosis of a bronchogenic carcinoma
Fair discussion. What do you think about the density of the nodule?
Air crescent sign can be seen in H. Cyst as well as in Mycetoma , the history of hemoptysis is suggestive of mycetoma , however .
i would like to ask something (may be is stupid)before descrip the density.
is intrapulmonary lesion?
Yes, it is intrapulmonary. You cannot be absolutely sure on the radiographs.
But I have a CT…
i think we have a mix ,high density node with (non central) coarse calcifications , well defined borders and “air crescent” sign in the LLL just behind the direction of the major fissure.
that exclude the hydatid infection (there is not calcifications)
professor i smell a very good case 🙂
Good. Thursday evening is your deadline (unless somebody else comes with the correct answer first)
AP and Lat views show a mass with an irregular border, inside a thin-walled cavity, located in the left lower lobe with an air-crescent sign. There are few ill defined area of low attenuation noted in the mass could be representing air bronchogram/hemorrhages. The location is atypical for Tuberculosis and Aspergilloma. the first line of thinking is Primary/metastatic carcinoma and a histopathology is strongly recommended, clinical history of frank hemoptysis and age of the patient well correlate with malignancy.
I agree with your interpretation, which would be adequate in your daily reading. Remember this is an unusual case, though.
HYDATID is another possibility as hydatid in lung do not calcify
I have never seen a calcified hydatid cyst in the lung. However, perhaps there is a report in some obscure journal about a guy who has two dozen of such cases!
I agree with your interpretation, which would be adequate in your daily reading. Remember this is an unusual case, though.
And what about somtehing calcified being inside bullae conected with a bronchus i.e a broncholith or “bullaelith”; or a foreing body. May we know if the patient suffered some previous procedure? i.e. bronchography or somtehing like plombage or surgery.
Bingo! You will be awarded the grat prize!
….GRAZIEEEEEEE!!!!!