Since I am an old codger, I am only allowed to look at pre-op chest films. As one young member of staff told me: you may be better than us, but we are faster because we read all of them as normal!
Today I am showing two pre-op chests. Would you read them as normal? If not, what do you see? Leave your comments below and come back for the answer on Friday.
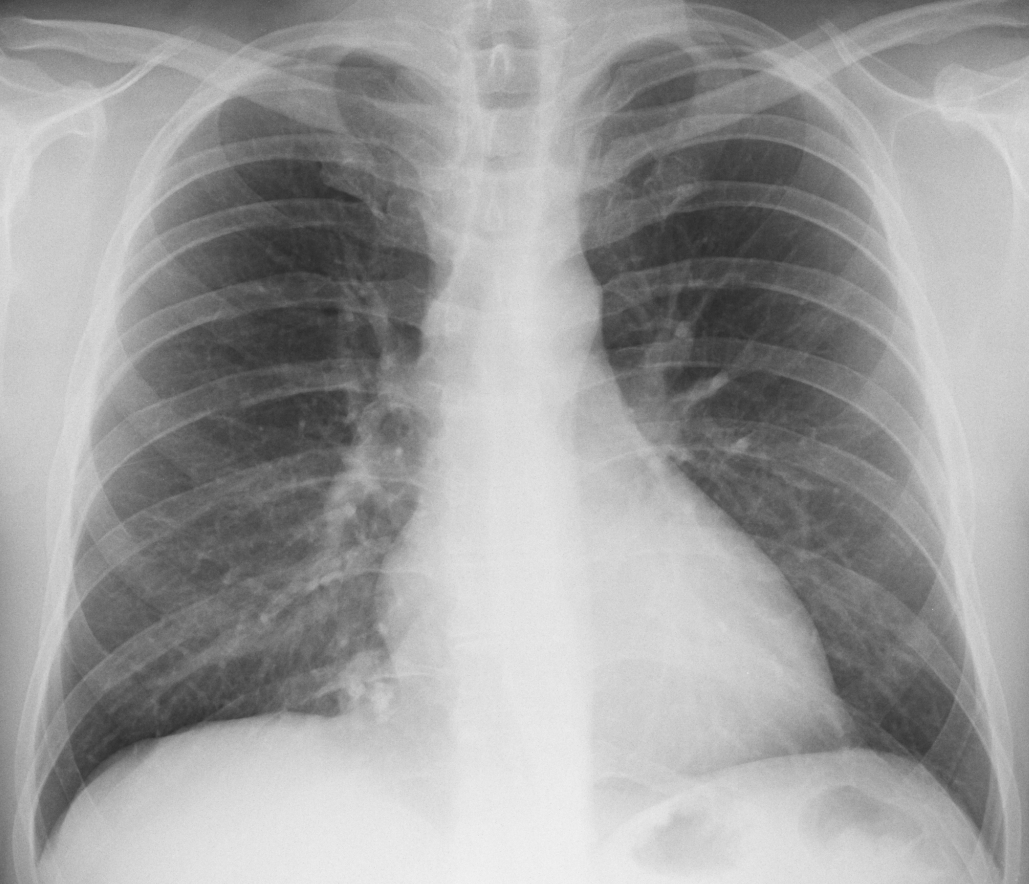
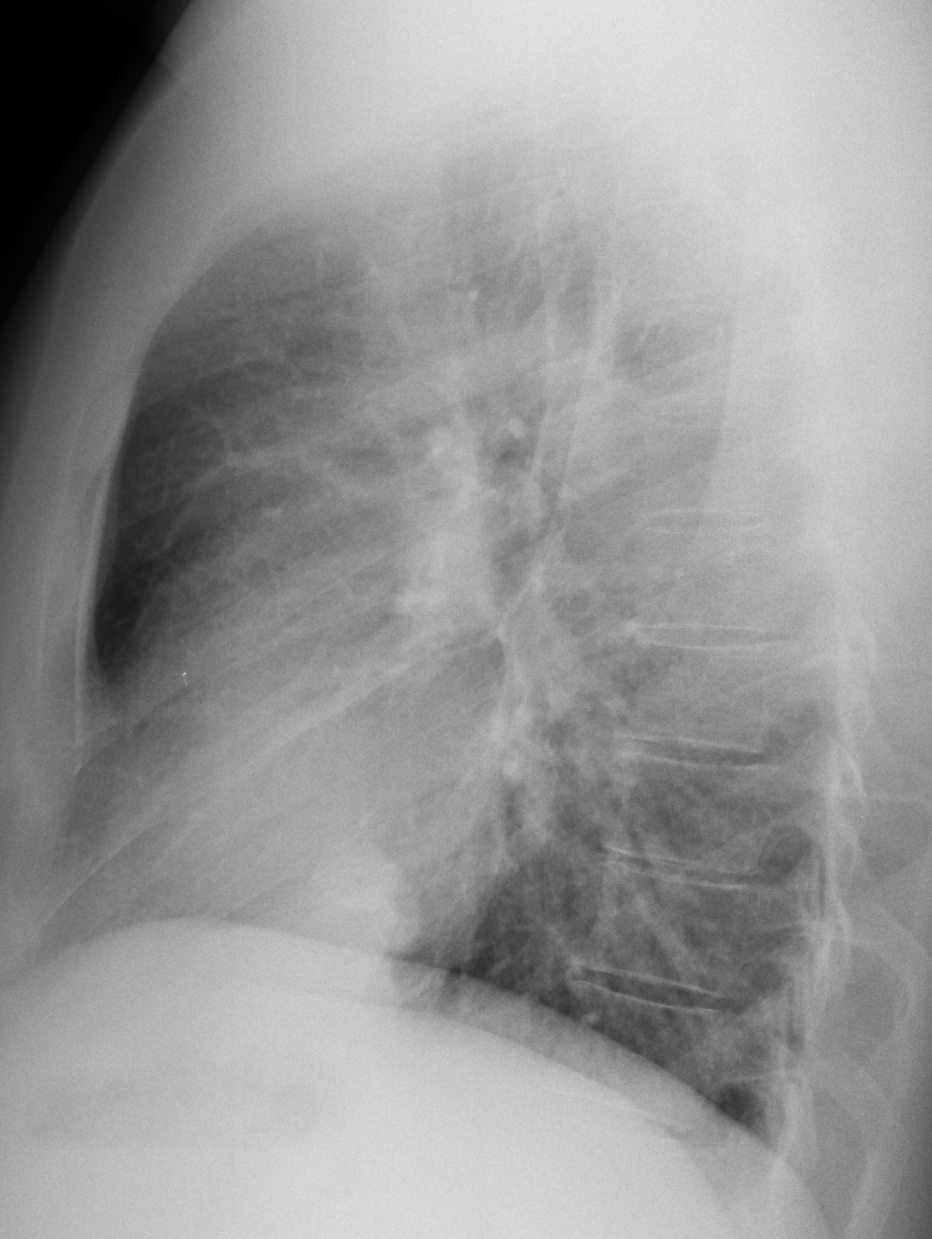
Patient 1 findings: there is a round pulmonary opacity at the right costophrenic angle (Fig 1 A,B arrow) with popcorn calcifications inside (A, red arrows).

Fig. 1
The appearance is very suggestive of hamartoma, confirmed with axial and sagittal CT (Fig 2, arrows).

Fig. 2
Diagnosis: hamartoma of right lower lobe
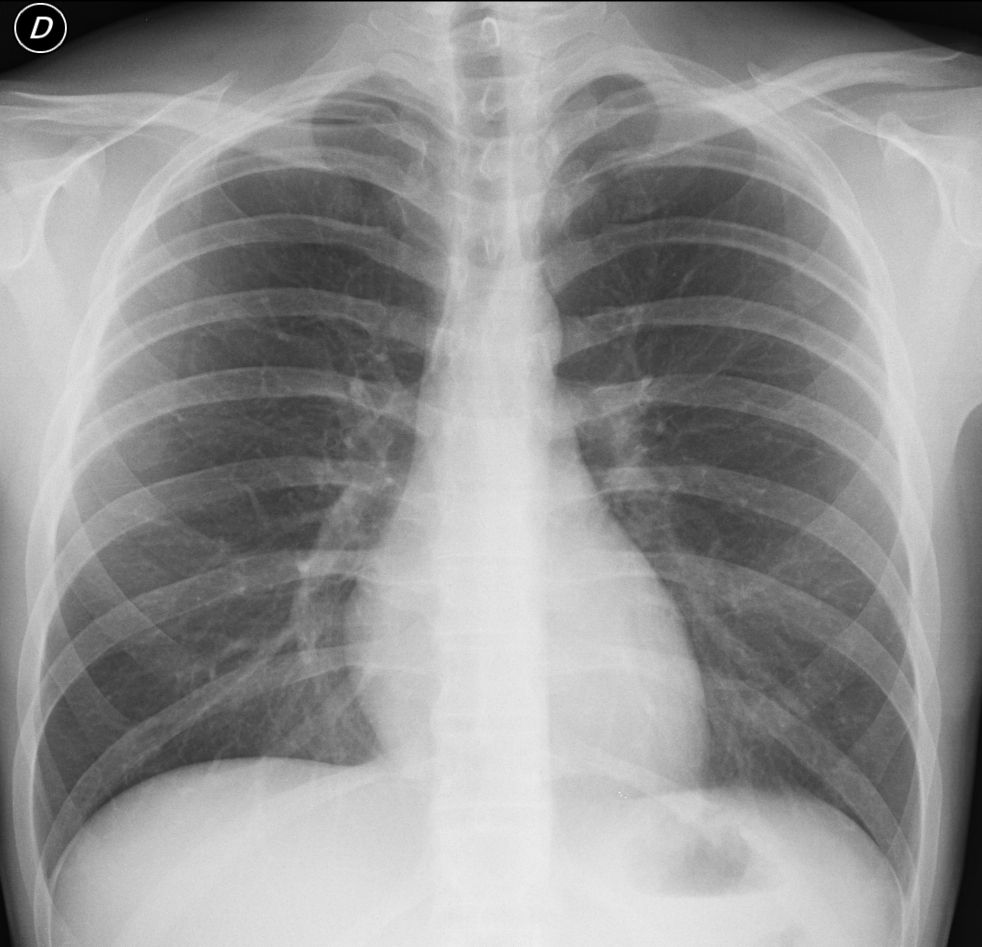
Patient 2 findings: PA chest shows a ribbon-like structure (A, arrow) arising from the undersurface of the right tenth rib. It is barely visible in the lateral view, coursing anteriorly to the rib (B, arrow). The density of this structure is similar to that of the rib and, on close observation, cortical bone is visible.

Patient 2
Diagnosis: intrathoracic rib. Because this entity has no clinical significance, no further studies were done.
Case 1 was reasonably easy to get. Case 2 was also easy if one recognises the density of the abnormality. As a matter of fact, several of you saw it, but confused it with an anomalous vein. Intrathoracic ribs are uncommon, more so if we fail to recognise them.
Teaching point: even apparently normal pre-op films may hide interesting findings. These two patients were seen last year.



Patien1: nodular expansion in right cardiophrenic angle, which is not mediastinal lipomatosis because of its shape. It may be atypic lymph node or expansion of right atrium or atypic axial hernia or mediastinal expansion.
Patient 2- norma.
Patient 1 . on the medial sinus there is intense round opacity-suggested lipoma
Patient 2. i think there is norma
Patient1: well defined oval radio dense opacity in right cardiophrenic angle with coarse calcification in centre and no cavitations.no effusion or hilar LN. Lateral film confirm the intra pulmonary location (solitary pulmonary nodule- most likely benign) 1st d/d hamartoma.
Patient 2: increased translucency in rt lower lobe at cp angle area and reduced vascular markings – may be due to emphysematous changes
Case 1: right lower lobe, paramediastinal round opacity – lung node, sequestrum
Case 2: left parahilar irregular opacity – lung node, lymphadenopathy
patient 1-solitary pulmonary nodule in right cardiophrenic angle on PA, with calcifications, probably benign-hamartoma, but need previous films for comparison. Patient 2 has a straight back syndrome, otherwise normal
Patient 1: Solitary pulmonary nodule in right cardiophrenic angle, with calcifications, probably hamartoma. Patient 2: Lineal imagine at right pulmonar base, below 10º costal arch that remember me “cimitarra sign”.
1. R cardiophrenic angle mass/nodule.
2. Focal opacity along posterior aspect of the trachea on lateral at the level of RUL bronchus. Hard to see on PA view; perhaps in L hilar region?
1. as colleagues said right cardiophrenic nodular opacification with calcification (calcified lymph node? hamartoma? pericardia cyst with wall calcification? pericardial fat necrosis with calcification?- long ddx)
2. right cariophrenic angle tubular opacity- it is agled the other way around compared to scimitar syndrome (no cardiac shift, no lung hypoplasia) i would consider a. rare PAPVR drainage with hepatic vein b. some king of a shunt or by-passing vein consisten with portal hypertension or Budd-Chiari
Any important clinical issues? Were the changes seen in chest radiographs reason for operation?
No
@1. after thinking a while i think in the mas i can see some lucencies maybe consistent with fat heavily pointing to hamartoma.
Hi Dr. Caceres
I understand you are getting older
Case 1. Right costophrenic angle nodule. Well delimited, pop-corn calcifications. My diagnosis, hamartoma.
Case 2. More difficult. Left lower lobe nodule, retrocardiac. I cannot see any calcifications. May be fat containing?
Getting older and not any wiser
Case 1. Hamartoma
Case 2. Retrocardiac opasity (bronhiectasia)
patient 1-solitary pulmonary nodule in right cardiophrenic angle( pericardial cyst,pericardial fat necrosis,lymphadenopathy,
fibrous tumour of the pleura,Morgagni’s hernia, Hamartoma)
patient 2- bronghiectasis
In my opinion, it’s difficult to diagnose bronchiectasis in the plain film, unless they are very obvious.
…Sidereo professore, entrambi gli rx-torace, sono anormali.1° abbastanza facile per la presenza di una opacità nodulare, a limiti netti, con grosslane calcificazioni nel contesto, come da amartoma(dd con il condroma polmonarwe).2° , piu’ difficile, dimostra uno spostamento a sx , della linea paratracheale sx, con opacità triandolare sottostante, e che impronta la colonna d’aria tracheale.In quello zona ci sono linfonodi, nervi s strutture vascolari….non sappiamo che tipo di intervento chirurgico il paziente dovrà fare….se x processo maligno dovremo pensare ad una linfopatia…se benigno a patologia delle restanti strutture….venerdì la TAC ce lo dira’!
Sorry, no TAC in patient 2
….se non c’è stato bisogno della Tac e,grazie al suggerimento del PROF., pensiamo ad un dismorfismo , ad Y. dell’arco posteriore della x costa di dx.
You are getting warmer…
pt1, hemartoma.
pt2,straight back syndrome.
ok i think patient 2 is normal. is a pre-op chest film but not for chest operation.
Sorry, I never show normal films. It is a disrespectful.
A different thing is showing an abnormality that may not be significant if properly interpreted.
What do you think of the lineal density at the right base mentioned by Adela? What does it look like?
it looks like osseous structure.
Good. All you need now is a name, to impress me!
1. R paracardiac mass
2. Intrathoracic rib
Hurrah! You mentioned the right diagnosis.
Apologies for not giving you credit in the official answer; was sent this afternoon.
I will give here your well deserved recognition!
Nel paziente 1 penso ci sia una cisti percardica., mentre nel paziente 2, davvero non trovo nulla!!!!
1. hamartoma?
2. scimitar sydrome.?
AV Malformation