Dear Friends,
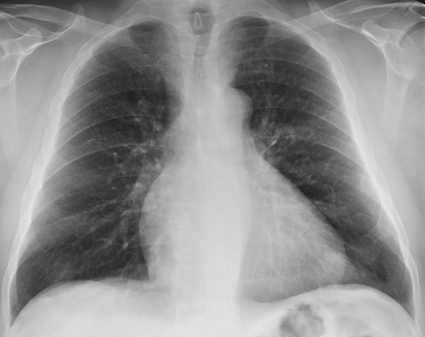
Our next case is that of a 60-year-old male with intermittent chest pain for the last year. If it is of any help, Muppet made the wrong diagnosis in this case. His mind was probably still in Mexico.
What do you see? What would be your diagnosis? Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.

Click here for the answer to case #87
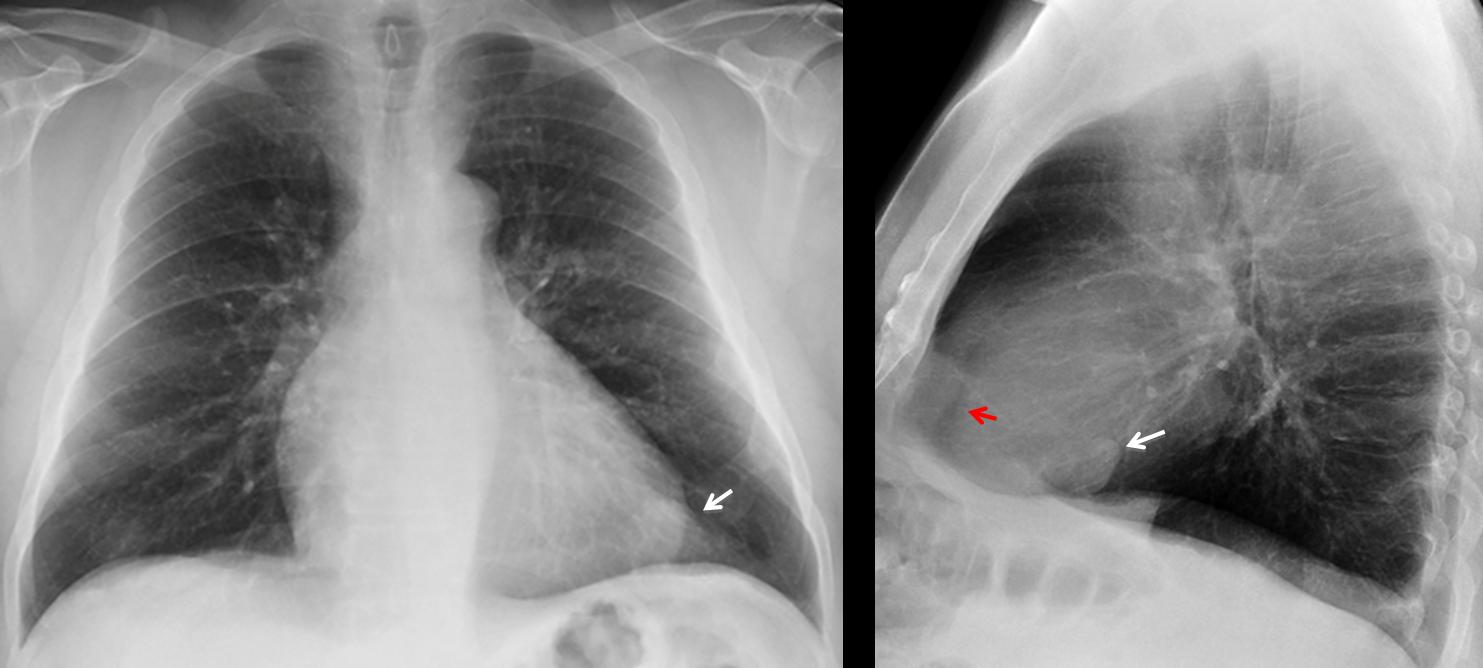
Findings: chest radiographs show a nodule adjacent to the cardiac silhouette (arrows). The epicardial fat is displaced posteriorly in the lateral view (red arrow) suggesting pericardial effusion.
With these findings I made a brilliant diagnosis: fibrous tumour of pleura irritating the adjacent pericardium and leading to pericardial effusion. CT proved me wrong, because the nodule was intrapulmonary (coronal CT, arrow). CT confirmed the pericardial effusion (sagittal CT, arrows) and the epicardial fat surrounded by it (red arrow).
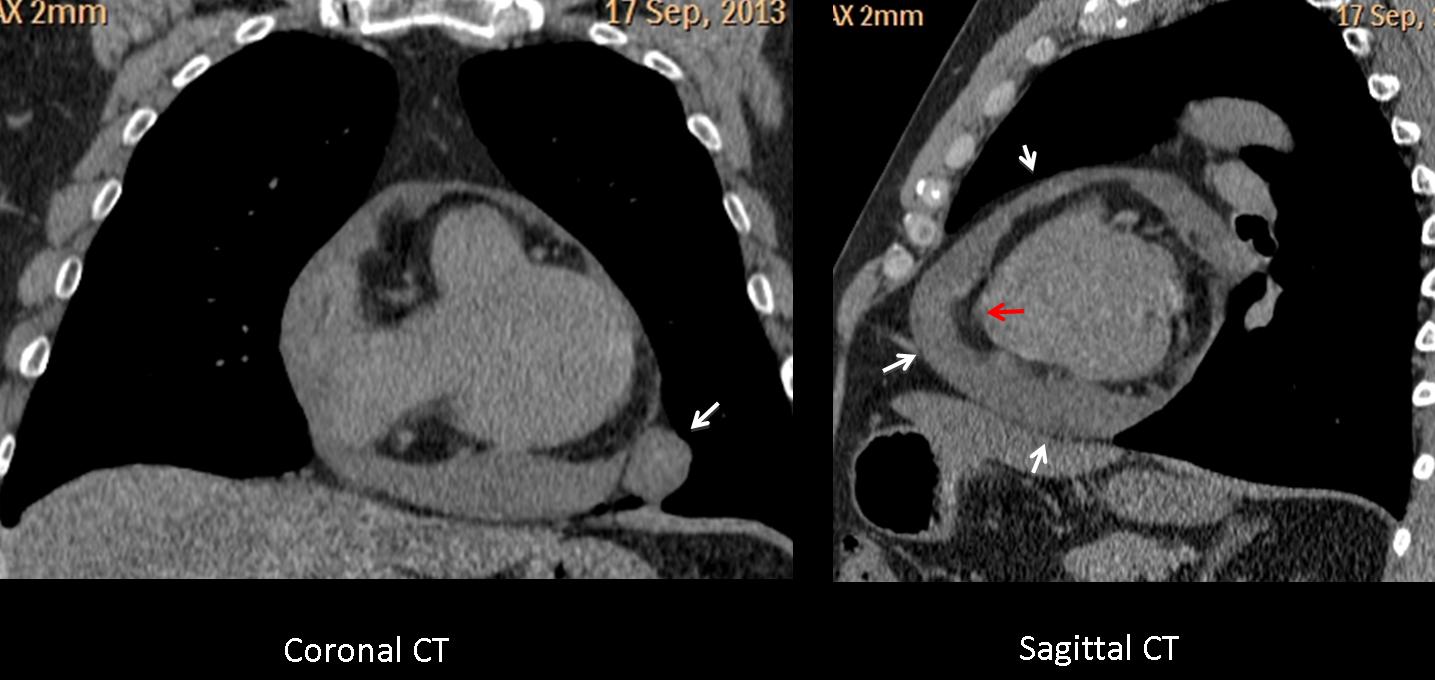
At surgery a benign hamartoma was found.
Final diagnosis: lung hamartoma with co-existing pericardial effusion.
Teaching point: This case is a good example of satisfaction of search: discovering the pericardial effusion raises the possibility of malignancy/ aggressive nodule. Pity I was wrong! To increase my misery, when I told one staff member that I had never seen a hamartoma with pericardial fluid, his answer was: “Now, you have”.


well defined radiodense opacity in retrocardiac area without calcification cavitation or spiculated margins. lesion appear to be intrapulmonary benign lesion. ?round pneumonia ? sequestration (less likely with given history)
Is there second lesion in retrosternal area in lateral view? pictures are small 🙁
Gozzo tiroideo immerso.
The aortic arch prophile appears “doubled” suggesting a vascular pathology…aneurismatic…
Pericardial cyst? Pericardial lipomatosis?
There is an oppacity in the posterior region of the left cardio-phrenic angle. Actually I do not know if it is intra or extrapulmonary in the PA view, but the fact that it is partially very well defined and I think there is a kind of MAG effect in the lateral view favours an extrapulmonary origin. I would say the double aortic arch could be because of elongation itself.
My initial differential for a well defined cardio-phrenic angle mass would include pericardial cyst, lipoma-epicardial prominent fat and small morgagni defect-hernia. These entities are usually asymptomatic.
The clinical scenario and the fact that it is a “Caceres’Corner Case” make me consider at least two other possibilities: the first would be an epicardial fat necrosis (even if I would expect more hyperacute presentation and we have already seen a case of this entity); the second one would be a left ventricular aneurism- pseudoaneurism (even if we cant see the quite typical laminar peripheral calcifications).
The latter (ventricular aneurism-pseudoaneurism) is my choice for the diagnostic orientation. I will be looking forward for the CT.
….mitico Professore può il Bari( in fallimento) battere lo stellare Barcellona? Posso io dare la risposta giusta laddove tu hai sbagliato? “mission impossible”….proverò a dare la mia risposta …”sbagliata”….una opacità a livello dell’angolo cardio-frenico sx, che fa corpo con l’immagine cardiaca in una storia sospetta per angina sarebbe compatibile con uno pseudo-aneurisma post-infartuale( Eco-cardio)…ma tu dici di aver sbagliato….allora proporrei per una necrosi del cappuccio adiposo pericardico(TAC)….
…il tuo “silenzio” professore mi fa capire che ho sbagliato la “prima” palla-goal…..riproviamo( con quella a cui avevo pensato per prima e che”meglio” va’ con la clinica di dolore toracico intermittente da un anno)…l’ipotesi di una “duplicazione” del profilo dell’arco aortico e del suo tratto discendente e, probabilmente della arteria succlavia sx, può deporre per un aneurisma aorta toracica del I tipo…resta immutata la patologia, occasionale, dell’apice cardiaco a sx…
Sorry, ball went out!
See the comment by Gus
…grazie per il suggerimento…..lieve cardiomegalia, da miocardite(misconosciuta), con versamento pericardico che si “raccoglie” in maniera “sacciforme”,all’apice cardiaco.
Dear Profesor Caceres,
thank you for interesting case of a male or women after billateral mastectomy, in age 55-65.
I almost agree with Albert, but there is something more on PA chest image. Namely the upper mediastinum in bilateral enlarge what suggest retrosternal mass. Perhaps it is goitre.
The mass in the anterior costo-pherenical angle looks more origine from the pleura as proven of the relative obtuse angle and long broad base of the leasion (A/B ratio). This leasion is also less dense then the secound ( more fat component ?).
The secound lesion is well define, sligtly lobulated, without any spicules, scars, calcifications and cavitation ( of course visible on ct) and its look its realeted to left lung.
In relation to last case and poor clinical information such a leasion can be:
– pulmonary hematoma
– round pneumonia
– round atelectasia
– primary Tu
– metastasis.
but it can be also a fat necrosis ( I remember we have such a case in last mounth ) with supleural lipoma.
But in this case is something more, like the vascular pedicule, which size looks enlarge. It s has round prominent margines on the right side what suggest to me a dillattaion of azygos vein – its only a first thought becouse I can pure distinguish right bronchus margines…The cardiothhoracic ratio is also enlarge. That mean that the ppatient has na cardiovascular problems what can suggest :
ddx :
– cardiac fat necrosis and hampton hump (both of them can cause chest pain)
– fat necrosis(I remember we have such a case in last mounth) with supleural lipoma.
I d like to compare present xray with past imagies….
now i must back to study 🙂
You presented an impressive discussion, but you misinterpreted one finding. Keep thinking.
(And the finding is not the possible goiter, which has no significance).
Dear Profesor Caceres/Dr Pepe,
thank you for prise, but its not enought for dgn.
Dear Profesor If you dont mind, I have a question. Is there somehow a possibility to dwoload xrays in dicom ?
That will help to distinquish subtle.
DICOM is an interesting possibility. Will check with informatics.
thank, you! That would allow higher specify and sensivity of imagies analisys.
thickening of the pericardium?
Either that or pericardial fluid.
ok the well defined mass on the right cardiophrenic angle is a rounded of incomplete radiolucent border (fat between heart and pericardium). that means the mass is cardiac …no?
the other hypothesis is pericardial recess as a normal appearance because of the pericardial fluid .
i don’t know….. we will see on friday 🙂
Don’t despair. Remember I too missed this case.
Nice and “sipmly” diagnosis 🙂