This week we are presenting pre-op radiographs of a 71-year-old man with torn ligaments of the right shoulder. As you can see, an unsuspected abnormality was found. What would be your diagnosis?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
1. Hydatid cyst
2. Carcinoma of the lung
3. Fibrous tumour of pleura
4. None of the above
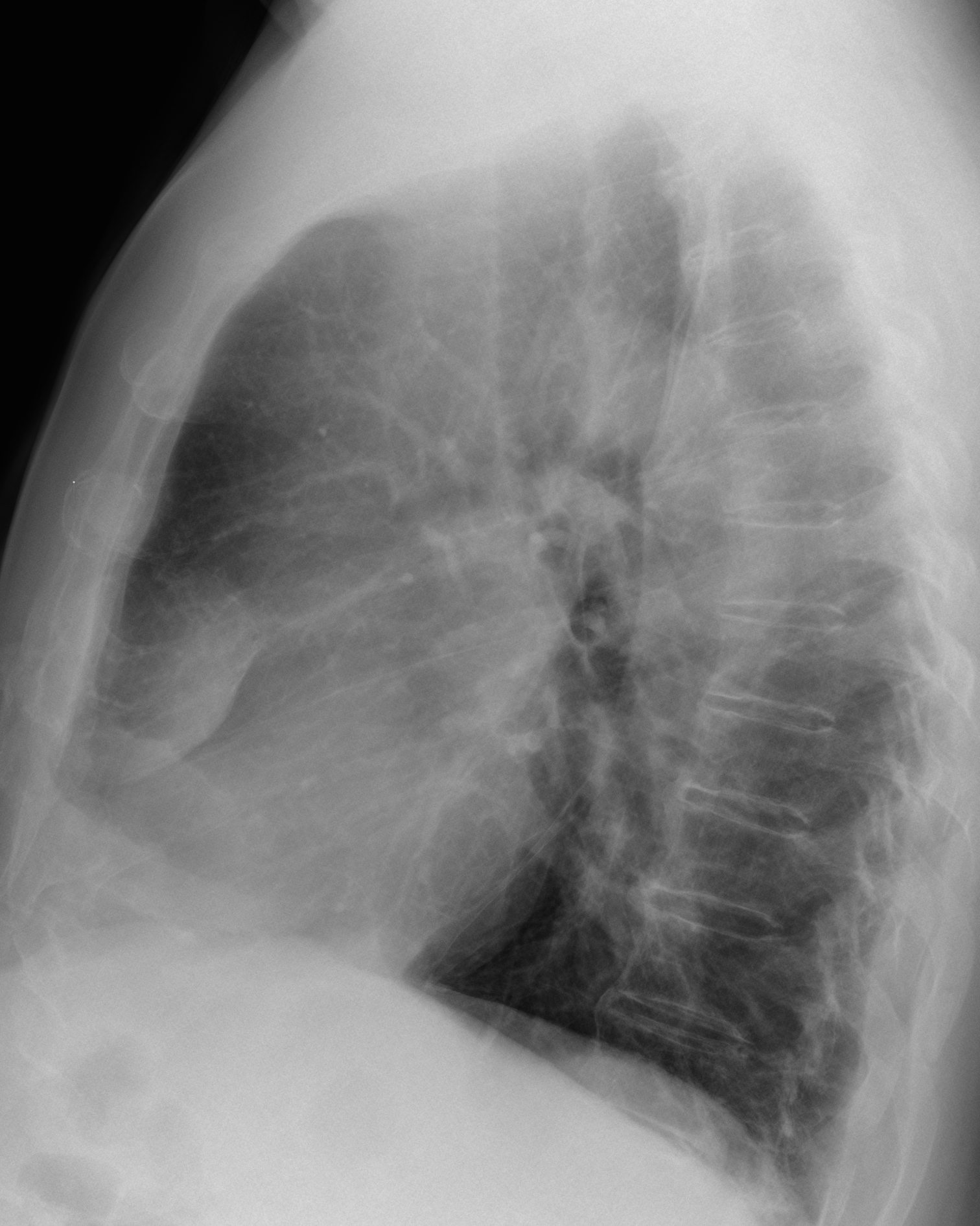
Findings: there is a round opacity in the right lower lung, which appears to be extrapulmonary in the lateral view (B, arrow). Close observation of the PA chest discovers a finely calcified rim around the lesion (A, arrows).
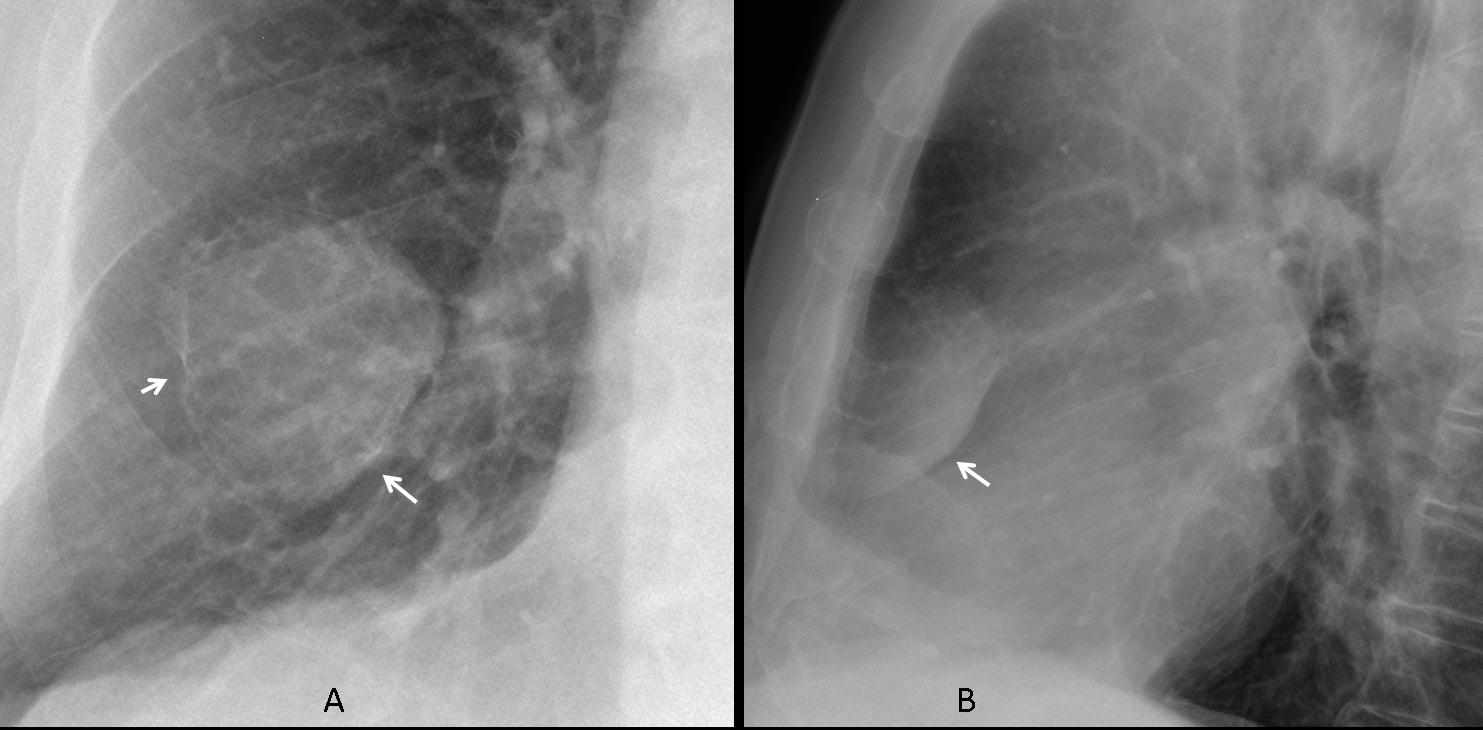
This finding excludes the three offered diagnoses and suggests a lesion arising from the anterior 5th rib which is poorly visualised compared to the one above and below.
Axial CT shows an expansive rib lesion with calcium inside (C, arrow) and a cortical break (D, arrow).
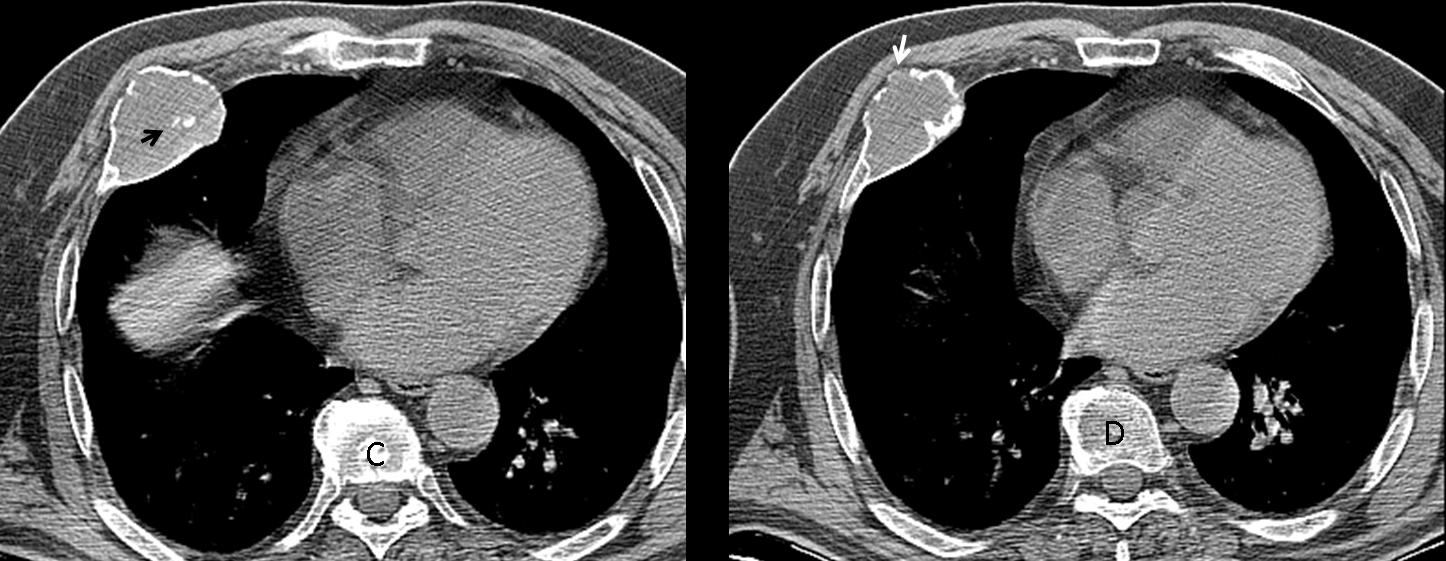
Final diagnosis: Grade II chondrosarcoma of the 5th rib.
Congratulations to Gus and Genchi Bari who, after some huffing and puffing, made the correct diagnosis.
Teaching point: When discovering an extrapulmonary lesion, always look at the underlying rib. In this particular case there was enough evidence to suspect that the lesion was originating in the rib.



The lesion is extrathoracic .
(gynecomastia – breast ca? or rib tumor?.
Well circumscribed pleural based lesion..my answer is 3
I think: PHANTOM TUMOUR (bounded fluidothorax) ventral right
I think it is a fibrous tumor od pleura…
It is Well defined, on lateral view adjacent to anterior chest wall and lung inrrrlobar oblique fissure…
Last one before the Warsaw approach…
Good luck with the examination. You will pass. I have no doubt.
I can’t say thank- don’t want to jinx it however it’s nice to have your support…
If I were an examiner I would ask you to take a closer look at the lesion
I totally agree with gus!
Gus offered three diagnosis.Do you agree with all three?
never totally 🙂
I think it is extrathoracic. I would consider a benign tumor as a subcutaneous lipoma or fibroma or even a neurinoma.
Inter lobar fissural in origin like encysted fissural effusion or fibrous pleural effusion
There is a positive incomplete border sign which is usually seen in extrapulmonary lesions, I agree with fibrous tumour of the pleura.
Thanks…
….sì è un tumore fibroso della pleura…..è sul “decorso” della piccola scissura interlobare …opacità omogenea, a margini netti, extra-polmonare( le diramazioni vasali sono conservate)ed intra-pleurica…..può sorgere in qualsuasi punto della pleura, da quella mediastinica a quella periferica, nonchè sul decorso della pleura scissurale….ne ho visto tanti nella rubrica “Weekly chest cases Korean”….Professore questa volta in tanti ti hanno fatto goals……Il Barcellona è in difficolta’ in Champions league!!!!!Il Bari vola!!!!!
Koreans are many and I am alone.
Wait until the end of the game to see who won. You may be surprised!
….e se fosse un condroma polmonare?
It is not a pulmonary chondroma (remember that the lesión is extrapulmonary). But you are getting closer.
….allora condroma costale….
Well defined round lesion seen in the right lung most probably has pleural origin and placed in oblique fissure. Because patient has no symptoms such as cough or shortness of breath and pleural effusion is not revealed, mesetelioma is unlike diagnosis. Fibrous pleural tumor is much possible. I could also include in DDs round atelectasis and vanishing tumor.
DISH in thoracic spine.
Given the anamnesis ( torn ligaments of the right shoulder)and characteristics of the lesion combined I wouldn’t put fibrous tumour as a first and most possible diagnosis. Fibrous tumour of pleura is quite rare. My suggestion: after a strong thorax contusion a fibrin clot in the pleural cavity can be formed in the resolution process of hemothorax. Therefore ,I would go for pleural mouse(tumor-like serofibrinous collection), as a first diagnosis in my differential. In most instances, it is located near the base of the lung and contacts the pleural surface. As this lesion often shifts after a change of patient’s position, sometimes repeat imaging can be quite useful in making the diagnosis. Regards 🙂
What about some foreing body inside the chest wall? Did he suffer from some intervention? The image reminds me something like a complicated breast prosthesis. Doesn´t it? Other thought is right breast fat necrosis.
Welcome back, Lola. No breast prosthesis in a male. How would you describe the lesion?
Pocket complication on infected cardiac pacemaker?
(prior reimplantation period?) crazy??:)
Don’t get too fancy. It is simpler than that. Look at the lesion closely.
Hola Doctores!
Frontal chest X ray reveals a rounded mass apparently placed in lower pulmonary field, with relatively well defined margins.
However, the lateral view shows a lentiform lession, with an inferior well delineated margin and an ill-defined superior margin, which suggest extrapulmonary mass placed oblique to the horizontal fissure.
The ribs seem to be intact to think in tumors like chondrosarcoma…
It could be a pseudotumor or “vanishing tumor of the pleura” due to loculated pleural effusion if the patient had heart disease or pneumonia, which is not this situation.
Maybe it is a localized fibrous tumor of the pleura…
Is there also chronic obstructive pulmonary disease?
I’m sorry about my english…!
Regards!
OK last try. cratilage tumor – rib tumor (Chondrosarcoma – Fibrous dysplasia)
Bingo!
…..grazie Mitico…..in ritardo, perchè sono in ritiro con la squadra di calcio (sono anche medico-sportivo)della Puglia per il titolo nazionale del torneo delle Regioni…..FORZA PUGLIA!!!!!!
It is a fairly rounded soft tissue opacity mass at the right lower lung zone differentials includes
1. fibroma
2. Loculated Pleural Effusion
3. Round Atelectasis
4. Bronchogenic Ca