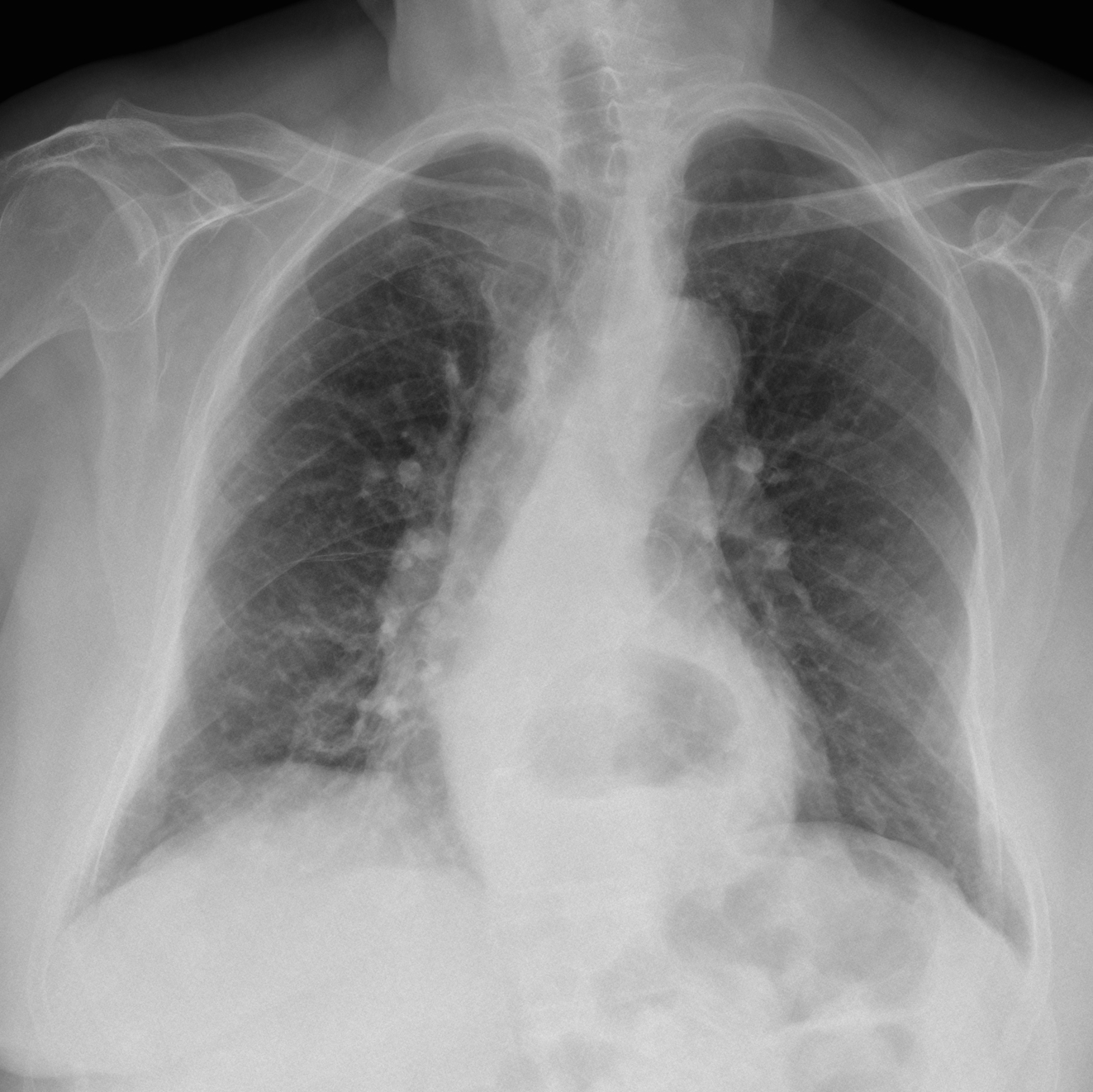
Presenting the case of a 85-year-old woman admitted with a severe urinary infection secondary to renal stones. Chest radiographs were taken one week after admission. Do you see any abnormalities in the chest?
Check the images below, leave your thoughts and diagnosis in the comments section and come back on Friday for the answer.
Findings: PA radiograph shows a pigtail catheter projected over the pulmonary artery silhouette (Fig 1A, arrow). The lateral view confirms that the catheter ends at the level of the main pulmonary artery (Fig 1B, red arrow) with its distal portion going into the abdomen (Fig 1B, arrows).
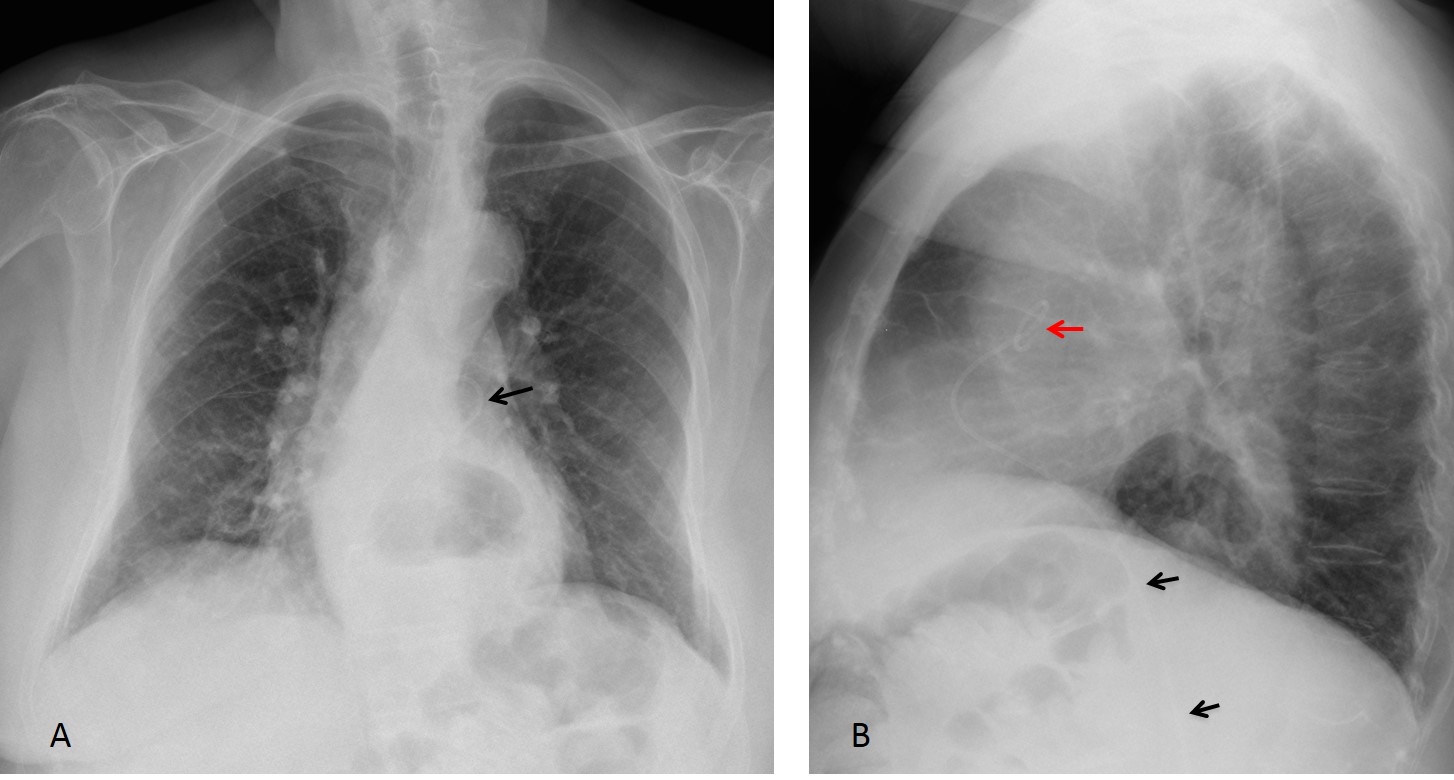
Fig. 1
Plain film of the abdomen shows the catheter in the midline (Fig 2, arrows).
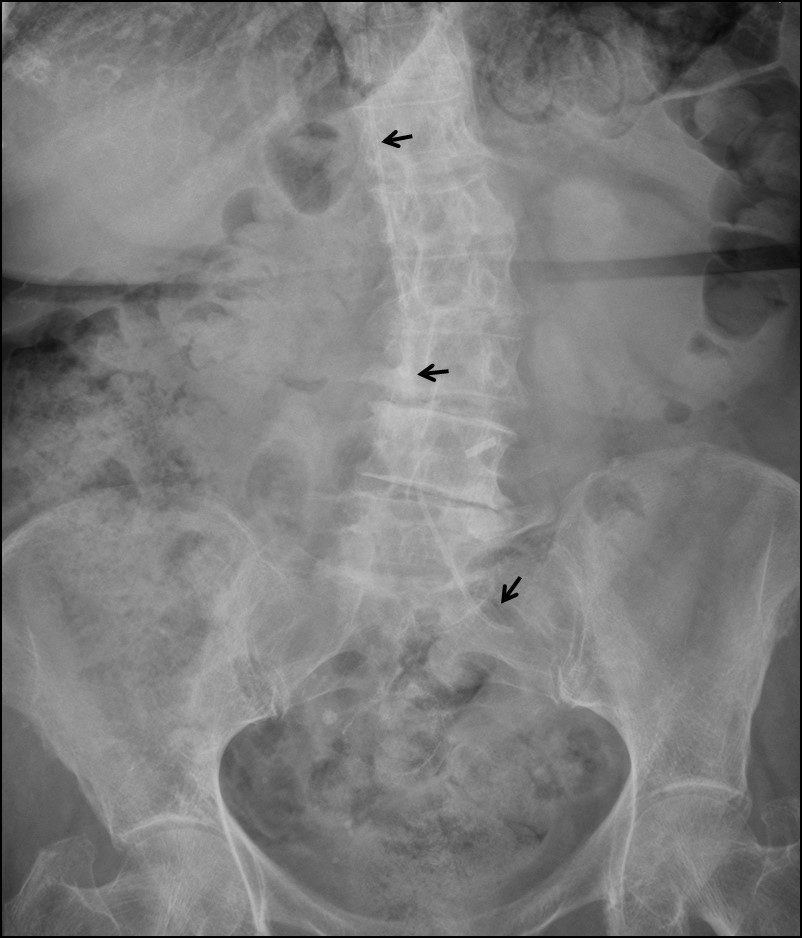
Fig. 2
Coronal and sagittal CT show the catheter entering the left iliac vein (Fig 3A, arrow), traversing the inferior vena cava (Fig 3A,B, arrows) and ending in the main pulmonary artery (Fig 3C, arrow).
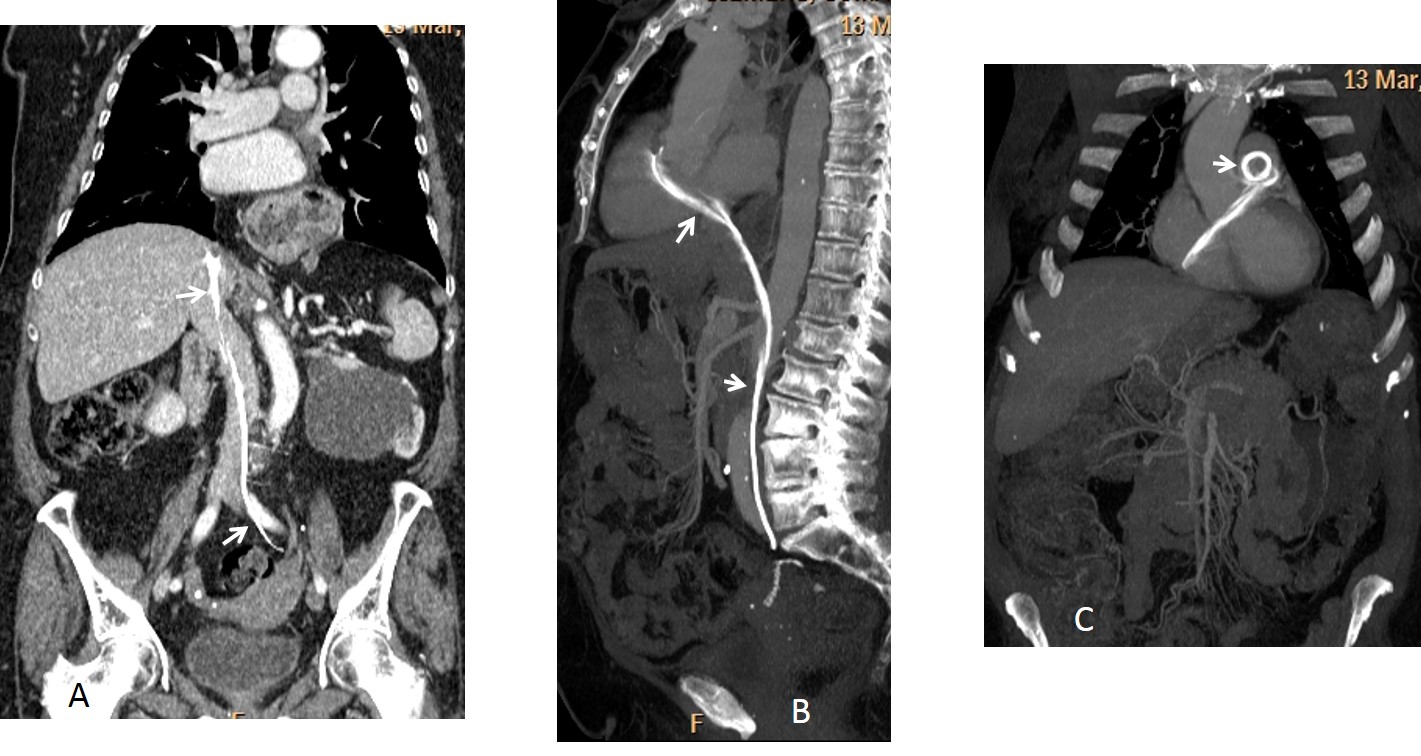
Fig. 3
In this patient, the pigtail was supposed to drain the left kidney. It was misplaced and perforated the left iliac vein, ending in the main pulmonary artery. Once discovered, it was removed percutaneously without complications.
Final diagnosis: inadvertent misplacement of urinary catheter into the inferior vena cava.
Congratulations to Jordi Velasquez, Genchi Bari and Francesco for their diagnostic acumen.
Teaching point: this is another case of catheter malposition. It is difficult to formulate a teaching point of this case, except for this: if anybody comes at you with a pigtail, cross your legs!



Hiatal hernia.
Hidropericardium.
Pigtail in pulmonary trunk, Pulmonary embolism?
Scoliosis and air fluid level retrocardi
1 Intrathoracic kidney
2 iatrogenic diaphragmatic rupture
IVP can help us
Bochdalek hernia with intrathoracic kidney
Hiatal hernia,…but it’ s obvious.I don’t believe that here is nothing else pathological:)
Hiatal hernia.
What’s with the right bronchus?
Right bronchus is OK
…”galactico”…ragioniamo con la clinica…..calcoli renali e grave infezione…..il calcolo ostruente può aver determinato idronefrosi, “complicata” con pionefrosi….necessità di drenaggio esterno del pus tramite nefrostomia percutanea…..ma il catetere , mal posizionato, “migra” nel torace(si proietta contro l’ombra cardiaca!)….vi è inoltre un livello idroaereo che può corrispondere ad una ernia iatale da scivolamento gastrico….NB il Bari è nei play-off x la serie A….ai “blaugrana” gli auguri di tornare i grandi di sempre!
….gentilissimo professore non pensi che la mia prima diagnosi fosse esatta? …parlavo di un cattivo posizionamento del catetere di drenaGGIO per la idro-pionefrosi, pensando solamente che il catetere fosse stato posizionato PER VIA trascutanea, pielostomica e non ascendente….la mia intuizione diagnostica era esatta….anche se il Bari domenica ha perso il Bari come il Barca sono grandi!!!!!
I gave you credit, of course. Hope you don’t mind sharing it with two colleagues.
It seems like hiatal hernia….
? sliding hiatus hernia with gastric fundus fluid level
iatrogenic diaphragmatic rupture vs diaphragmatic hernia with intrathoracic kidney
Interesting diagnosis. But is not the correct one. Sorry
Where is the other end of catheter?
Where, indeed?
trans-diafragmatic erniation of hollow viscus (hiatal hernia?); pig-tail catether in inferior vena cava, right atrium, right ventriculum, pulmonary trunk (for pneumoangiography).
Mediastinitis?
…la chiave di lettura è il catetere( che non deve più essere in relazione alla pielostomia percutanea, come suggerito dalla clinica: calcolosi renale ed IVU)….allora il catetere è “vascolare” e si localizza in una sede “aneurismatica” cardio-vascolare, come si vede in LL…..a parte l’ernia iatale da scivolamento gastrico….qualche notizia anamnestica in più avrebbe agevolato la diagnosi….va meglio ora?
I think there is a posterior cardiac displacement, maybe the catheter is not incidental there. the other job is to drainage collections but a pericardial fluid collection with cardioparacentisis is subxiphoid approach or percardiocentesis via pleural space. that’s why i want to know the other end of the catheter 🙂
OK, you stated your case. The catheter ends in the abdomen (look at the lateral view)
soft tissue located anterior to cardiac shadow likely intra thoracic kidney congenitally located with renal stone treated by DJ stent to release obstruction ,, hiatus hernia / inflammatory process located posterior to kidney shadow
Very interesting case. There are many propositions for explaining the catheter – normal position of pulmonary catheter, percutaneous drainage catheter,inrathoracic kidney etc.
I will add a possibility of a double J ureteral stent displacement through vena cava inferior and into the heart.
Hiatal hernia is also seen.
Correct diagnosis, but late. Sorry
Ok, next time I will try to answer earlier 🙂
good case!!! I didn’t know that. It’s an urgent condition.
To be honest , I also didn’t know that until this week. 🙂
That makes three