Dear Friends,
Dr. Pepe has urgent business (suspect he is visiting Miss Piggy) and asked me to cover for him this week and the next. He will be back with a new Diploma case on Monday, June 9.
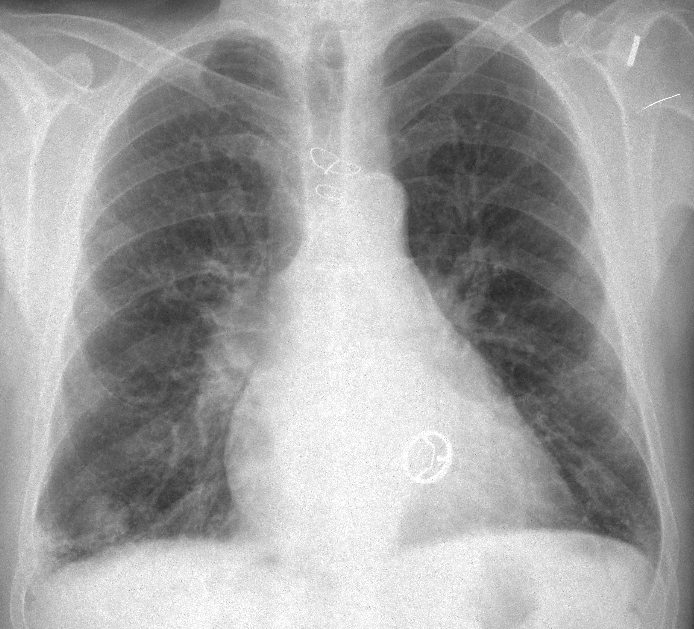
My good friend and former resident Dr. Eva Castañer has contributed with this week`s case. Images are of a 74-year-old male admitted with hemoptysis. Leave your diagnosis in the comments section and come back for the answer on Friday.
Diagnosis:
1. Pulmonary infarction
2. Carcinoma
3. Tuberculoma
4. None of the above
Click here for the answer to case #94
Findings: PA radiograph shows an ill-defined infiltrate at the right costophrenic angle and a nodular shadow at the right base (arrow). A prosthetic mitral valve is seen.
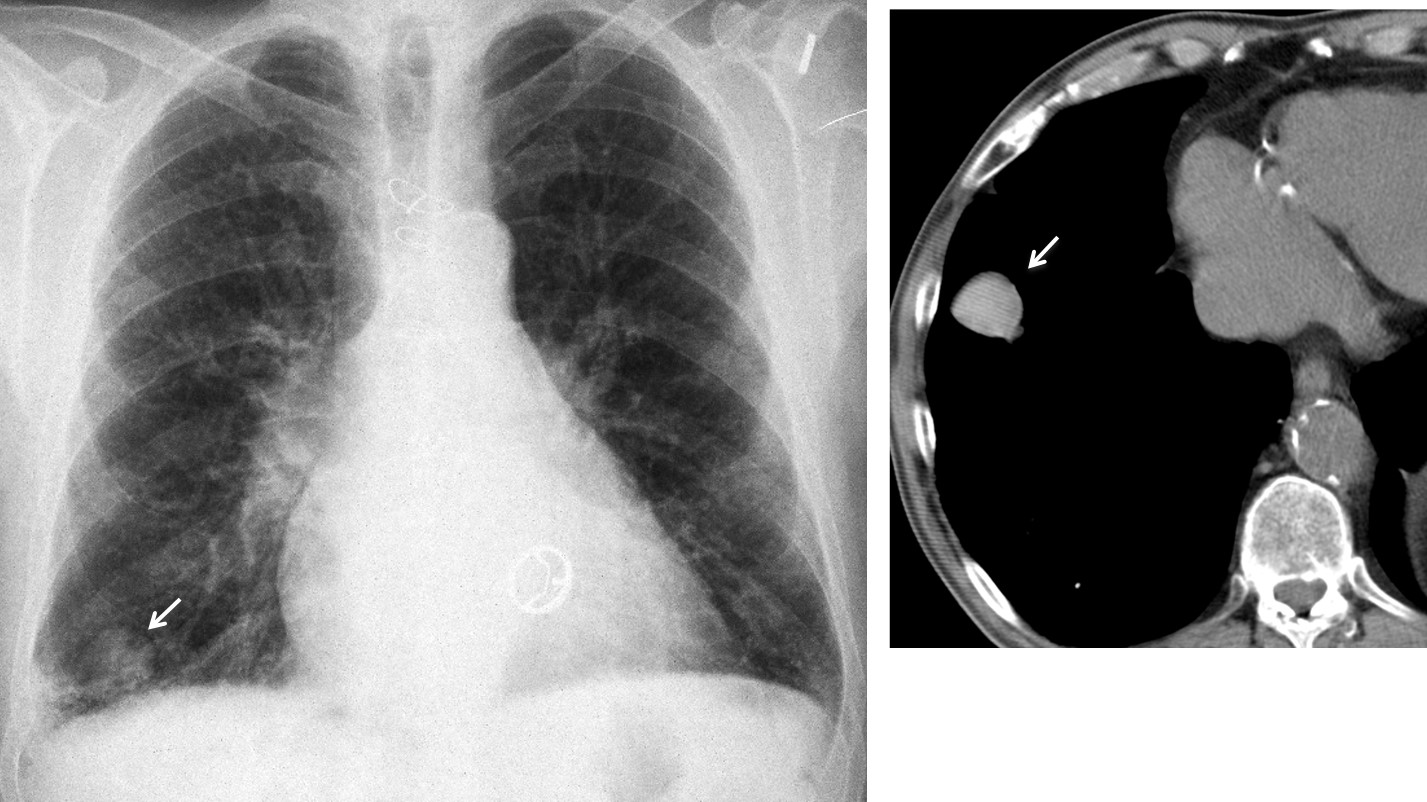
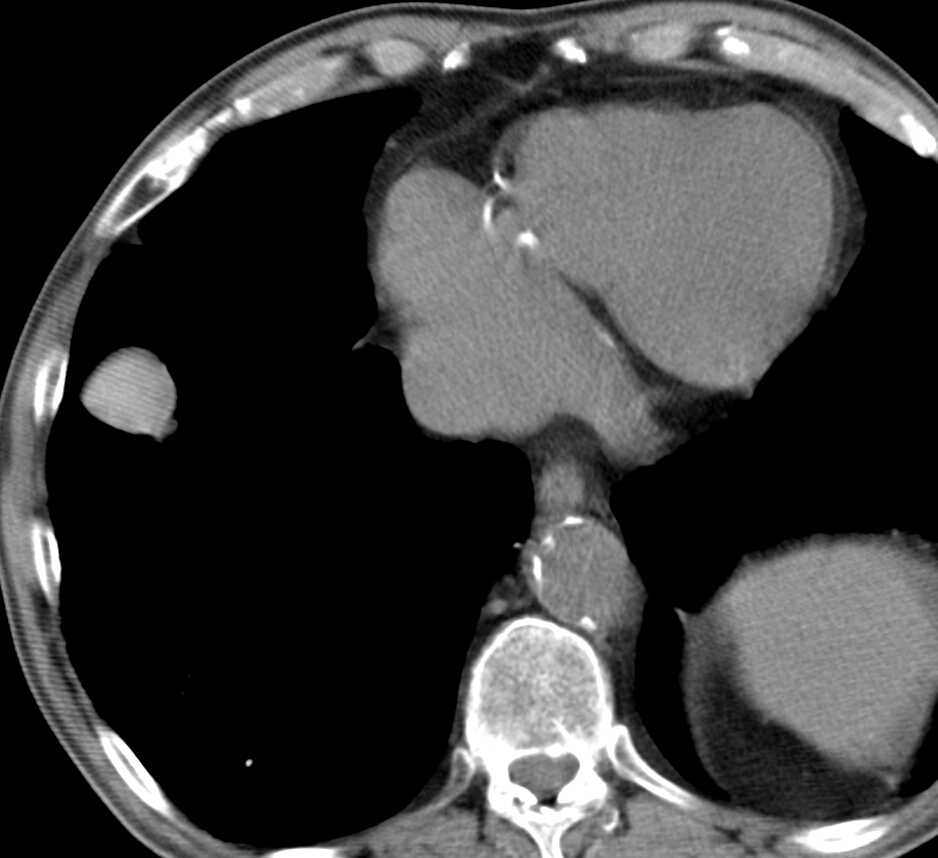
Unenhanced axial CT confirms a well-defined nodule (arrow), denser (84 HU) than the surrounding soft tissues. This finding raises the possibility of a haematoma, although a needle biopsy was done to exclude malignancy (negative result). Follow-up CT at one and four months shows a marked decrease in the size of the nodule.
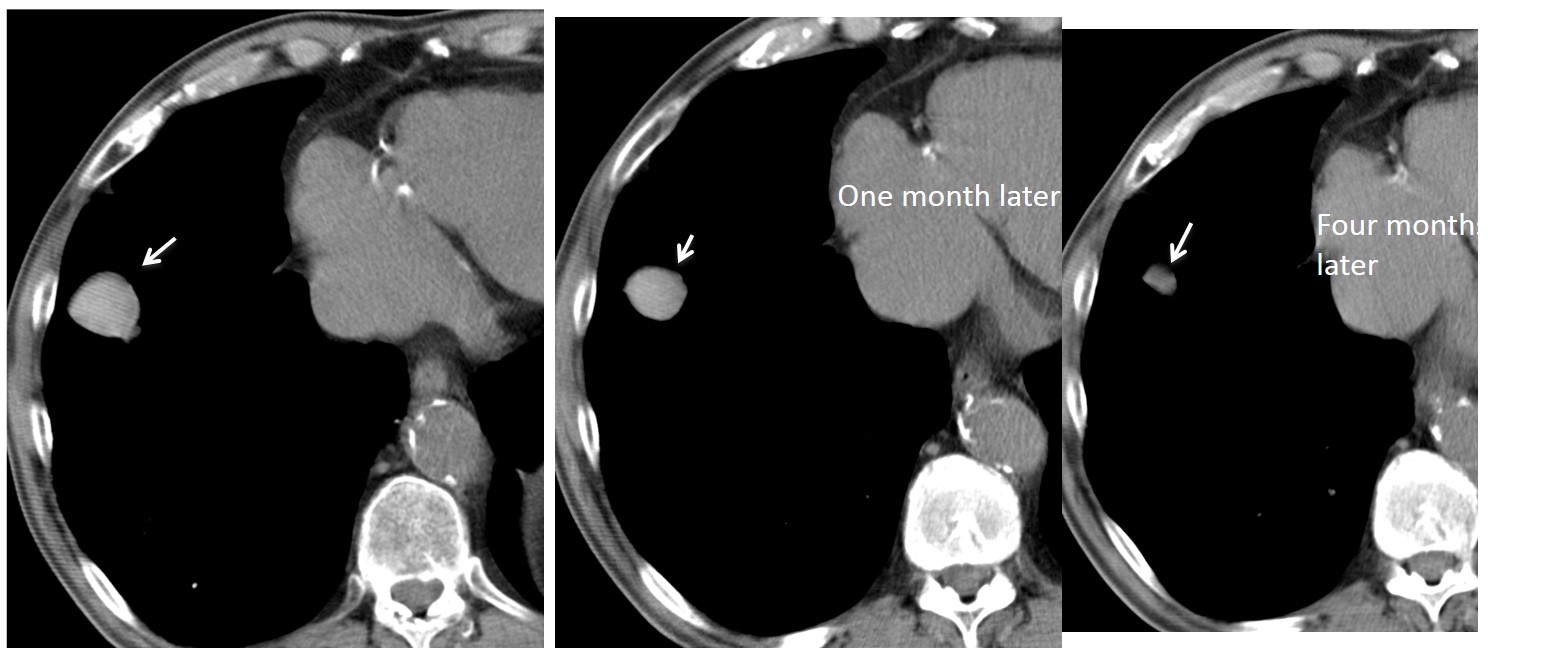
Final diagnosis: spontaneous lung haematoma in an anticoagulated patient.
Congratulations to Gaborini who was the very first to answer and gave the right diagnosis.
Teaching point: spontaneous haematomas are unusual but can be suspected by their high density at unenhanced CT. Follow-up films confirm the diagnosis by showing a steady decrease in size.


the lesion seems a little bit hyperdense relative to the muscles or the intravascular blood on the non-enhanced scan. Together with the history of the patient this suggests a pulmonary hematoma / hematocele.
He may be on anticoagulation therapy due to valvular prosthesis.
due to its hyper density in a non contrast scan, i’m thinking of haemorrhage, with a linear opacity seen medial to it on the X-ray, seams like something vascular, i’m thinking of AVM, also the patient had a previous heart surgery so likely he is on anticoagulant medication, so my final diagnosis is AVM haemorrhage
another differential i would say pulmonary pseudo aneurysm
Carcinoma
….”galactico”…..clinica….protesi valvolare meccanica esiti di sternotomia mediana e capsulo-plastica scapolo-omerale sx….non può essere un cr per le caratteristiche ,non infiltranti, dei margini regolari…non tubercoloma per la sede atipica e mancanza di reliquati calcifici…può essere invece, non tanto una complicanza della terapia anticoagulante, quanto una complicanza della protesi meccanica, con trombo-embolismo ed infarcimento vascolare emorragico(nodulo disomegeamente iperdenso)…regola KISS….
My dear friend I have to disagree with you, because you exclude carcinoma due to the regular borders (partially correct) and you suggest an infarction (usually irregular borders) for the same reason. One or both should be wrong.
….gentilissimo Professore, grazie per le osservazioni….il caso è interessante in quanto determina un grosso problema,relativamente alla “gestione”del nodulo di ndd nei casi di soggetti con terapia anticoagulante x protesi valvolare:è un nodulo emorragico(=terapia anticoagulante con eparina) oppure è un nodulo trombo-embolico da complicanza valvolare(= terapia coagulante con fibrinogeno)…il radiologo è chiamato a risolvere , con “urgenza” il problema…..se invece il nodulo è di altra natura la diagnosi può essere posta in tempi più lunghi….tu cosa suggerisce fare?
4. None of those 🙂
To be honest: no idea…
I think, he’s got cardiac valves…
Ähm artificial heart valves…
Don´t worry. Answer on Friday. Hope you learn something new.
for a patient with heart problems i’m thinking also of amiodarone toxicity
I dare to say that there is crescent air sign on the xray around the nodule. So i would add aspergiloma or tuberculoma on à preexisting cavity.
I believe the possible crescent sign is a Mach band and not real. You don´t see it in the CT.
Because the patient has previous heart surgery and the location of the lesion in the peripheral base i think it looks more like
infarction.
i think we have to wait for a while before the biopsy.
Do you really believe that I would show an infarction?
No! 🙂 but Dr. Eva Castañer has contributed with this week`s case 🙂
Solitary pulmonary lesion of the RLL in a patient with anticoagulation for previous cardiac valve implant: we need to includein the DD bronchogenic carcinoma, bronchogenic cyst, granuloma and, of course, a iatrogenic origin from the anticoagulative therapy. I tink that a needle aspiration biopsy will be really useful ( if no previous rx/tc were avaliable!). Waiting for your illuminating comments.
This case was reported by Dr. Eva Castañer. Look her up in internet
Thanks, professor, I’ve just found an article of Eva Castaneda in the Radiographics site named “CT Diagnosis of Chronic Pulmonary Thromboembolism”. It seems intresting. I’ll follow you on the blog. Thanks again
Ciao
This case was reported in the European Journal of Radiology Extra 01/2007: Pulmonary hematoma secondary to anticoagulant therapy: imaging findings.
Glad to have you with us.
benign looking nodule smooth margin no calcification cystic ares fat or feeding vessels peripheral but not pleural based i suggest hamartoma rather than tuberculoma inspite of no fat or calcification yet lower lobe location and age may prefer this suggestions ,follow up for growth rate is only needed as no difference in management between both of them??
In the x-ray we see a nodular image in the right lower lobe, we confirm this finding in the axial CT image, the nodule has smooth borders and is a little hyperdense compared with the cardiac cavities and aorta. Between the choices for the differential diagnosis for me the better one is a TUBERCULOMA, complicated with a Rasmussen Aneurysm.
Hello Everyone – as I am new here 🙂
I agree with the concept that this lesion probably have sth in common with anticoagulation therapy in the setting of prosthetic heart valve and therefore hematoma would be my 1st choice – but – I am curious why nobody add to the list round atelectasis? I thought about that mostly looking at the plain film- there is some pleural thickening and connection with the lesion ( I am imagining that ths could be comet`s tail sing)- unfortunately – CT scan is not showing these features ( maybe it is taken from the level of upper half of the lesion?.. Location in basal portion of the lungs, where alveoli are less ventilated, is more frequent..But I cannot connect hemopthysis with that..What do you think?
Rounded atelectasis are not dense on CT and they are ill-defined and with air bronchogram. I would not considered them in the differential diagnosis.
Glad to have you with us. Hope you diagnose the next case.
Is so clear, a mechanical valve in mitral positión and add the ICT. The right hyperdensity is the lever Is very possible a descoagulation by iatrogenia