Today we are wearing typical Basque txapelas; a gift from my good friend Dr. Estibalitz Montejo from Bilbao.
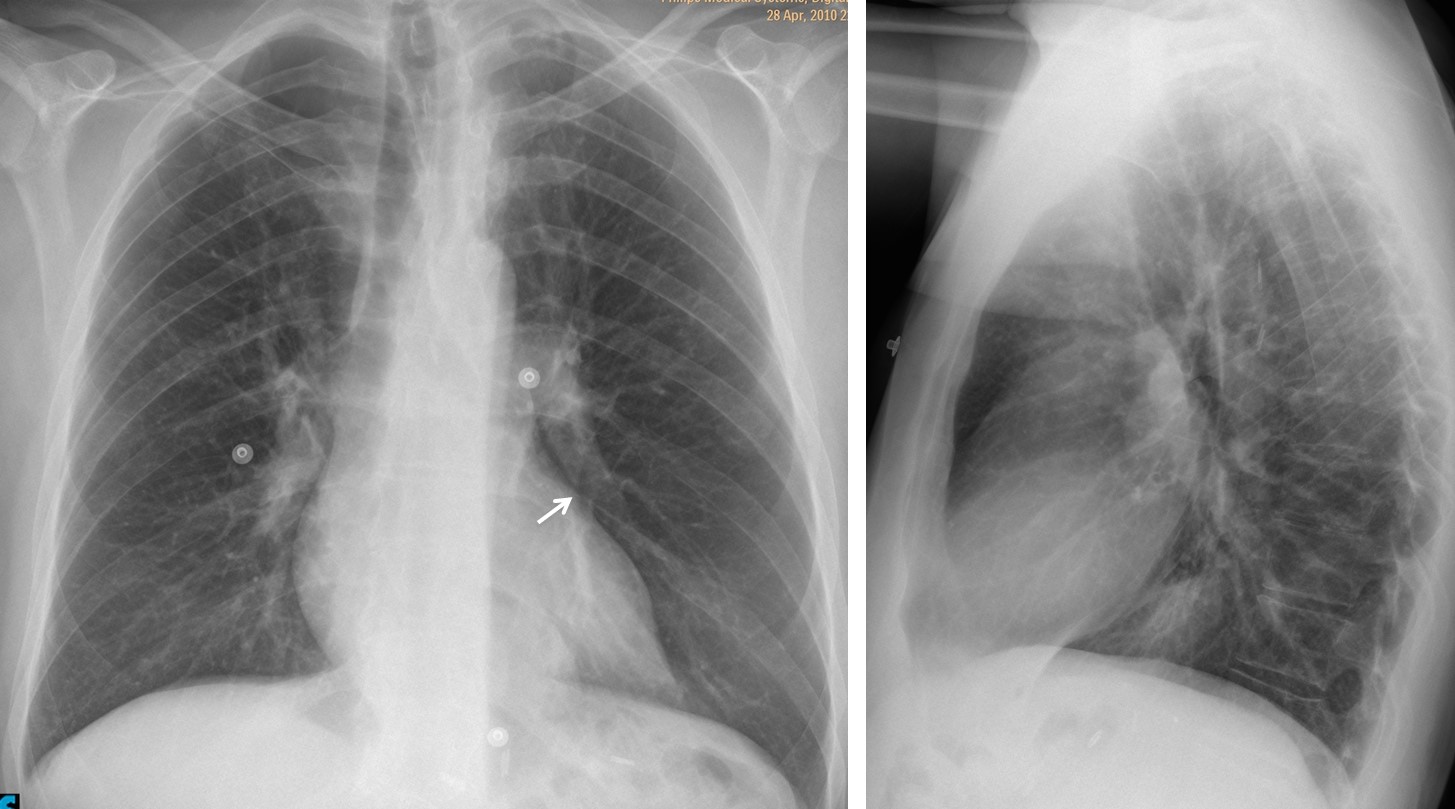
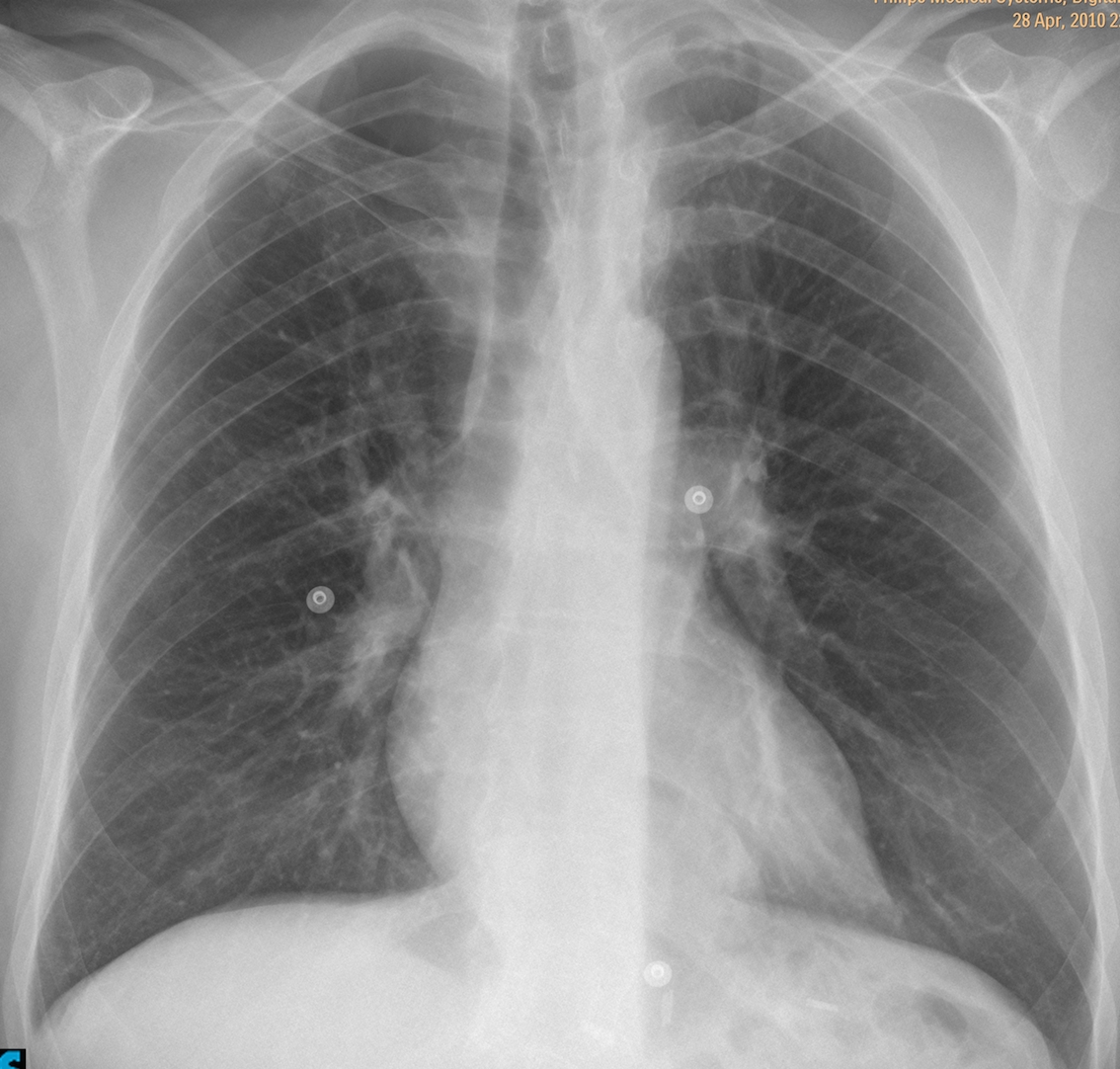
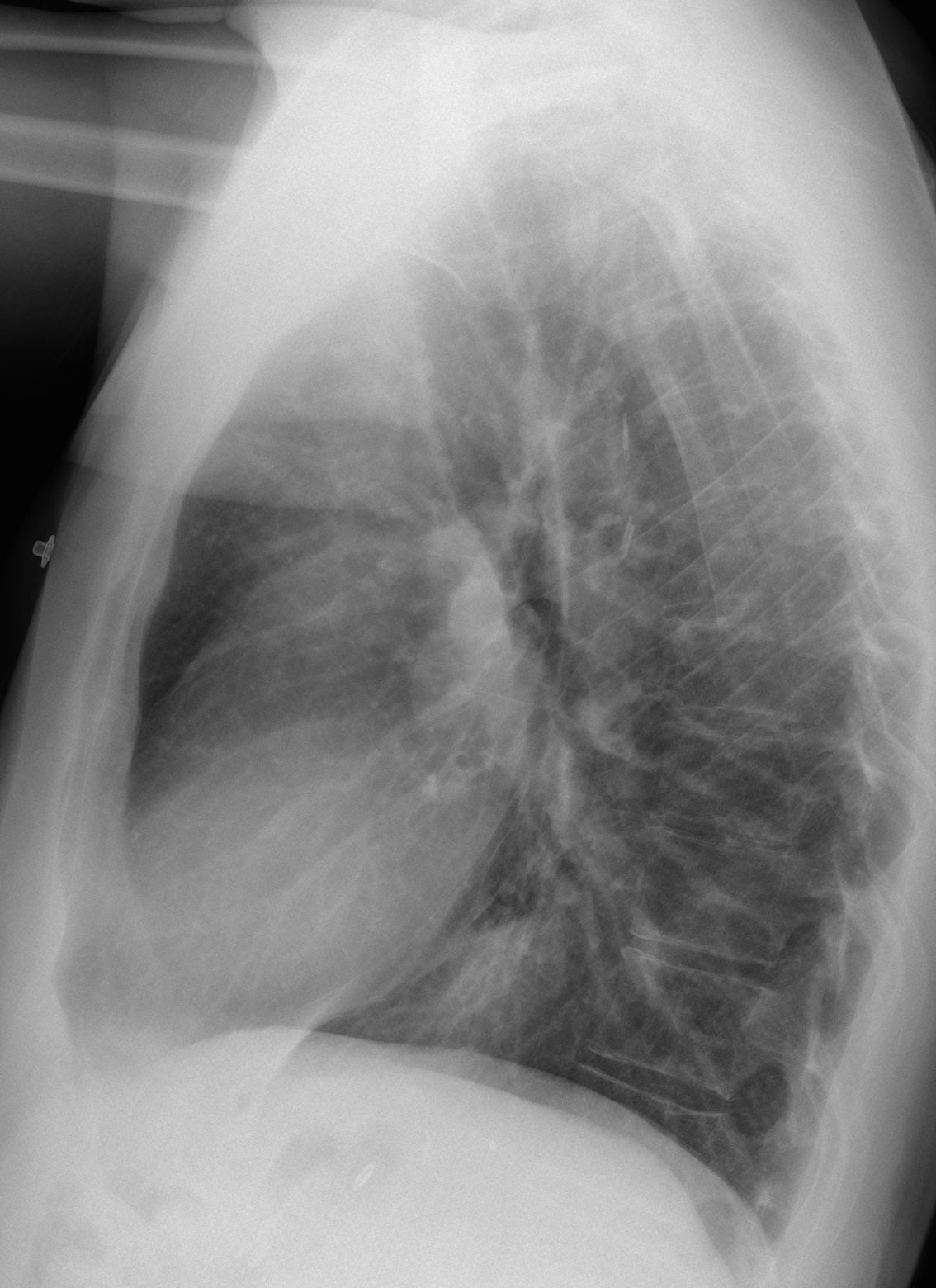
Below are two radiographs of a 45-year-old male with acute chest pain. What do you see? What would be your diagnosis?
Leave us yout thoughts in the comments section and come back on Friday for the answer.
Findings: the most obvious finding is redistribution of the pulmonary vasculature, with increased size of the upper lobe vessels compared to the lower ones. This appearance has been described in mitral disease, left heart failure and emphysema of lower lobes, among others. In this particular case, the appearance of the chest does not support these diagnoses. Redistribution may also occur in lower lobe embolism, suspected in this case for the clinical symptoms and the presence of a Westermark sign in the left lower lobe artery (arrow).
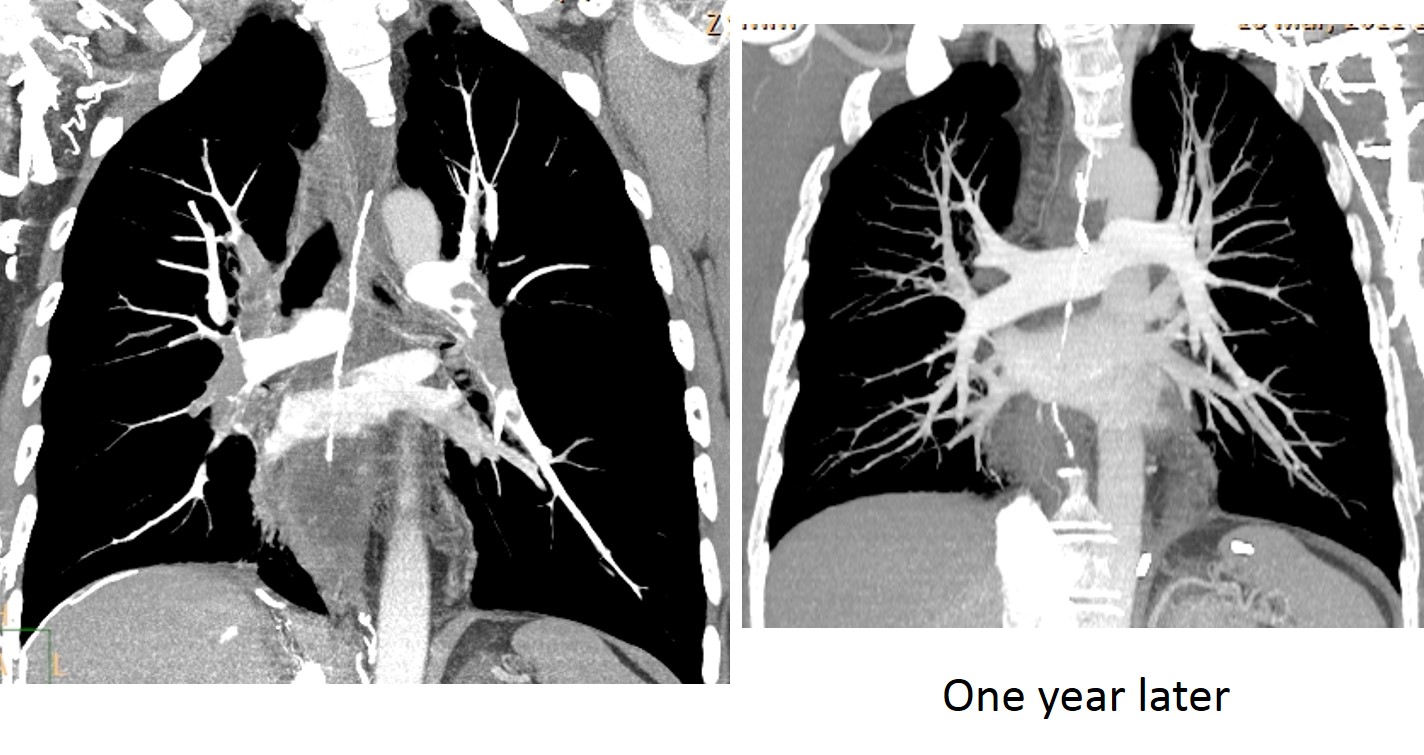
CT angiogram confirms extensive pulmonary embolism. Follow-up one year later shows a normal arterial tree.
The patient had SVC thrombosis secondary to previous port-a-cath and, at the time of this episode, had right femoral vein thrombus.
Final diagnosis: acute pulmonary embolism with Westermark sign.
Congratulations to Luis Cueto, Laurens and Genchi Bari, who suggested the correct diagnosis.
Teaching point: It is important to identify vascular redistribution, because it narrows the diagnostic possibilities. After saying that, I must confess that this is my first Westermark sign!


three are two finds, right paratracheal opacity and retrocardiac opacity as hiatal hernia
In the first x-ray I see a retrocardiac opacity that is confirmed in the lateral view and surgical clips in the LUQ.
In the second one, there are more surgical clips, this time they are project in the posterior mediastinum, in the aortic or esophageal wall??
There are also clips in the upper abdomen. Patient was operated on for carcinoma of the lower esoghagus in 2005. No problems since then.
Sorry, German: Vd.a. Neurinoma im unteren BWS-Bereich bei angedeutet weitem Neuroforamen in seitlicher Projektion oberhalb des Zwerchfells.
Don’t worry. Google translator works for me.
Falsche Diagnose 😉
There is also absence of vessels at the right apex which can be
1.a secondary esophageal diverticulum
2.rupture of a pulmonary bulla
3.any other idea?
Good observation. I would expect a ruptured bulla to have an air-fluid level at the botton.
There’s an azygos fissure, with a position more caudad than normal. There are no vascular markings cranial to the azygos fissure. To me these findings suggest a pneumothorax confined in an azygos lobe.
Smart diagnosis, but not the right one.
Left apex seems abnormal -is it only my imagination?
Dear Professor why are You using jpg intstead of DICOM?
Sorry, you are imagining things 😉
I am using jpg because most of the cases are from my private collection and all of them are on jpg format.
pulled up stomach
Yes, the patient had been operated on. But it is not the intended diagnosis.
I believe you all are failing to see the obvious.
Take a step back and look at the PA chest.
Old costal fractures on the both sides – most probably due to the operation.
Giant bulla in RUL (it would be good to compare to the previous CXR). But bulla is not painful, and here is no pneumothorax. Why patient has chest pain? Is the answer on this CXR?
Left apical pleural thickening is seen. Possibility of a left pancoast tumour needs to be considered.
In a patient operated for esophageal cancer, the upper thoracic levoscoliosis is worrisome for me. Possibility of vertebral metastases needs to be considered.
The hyperlucency in the right apex, devoid of vascularity is most likely due to a bulla. There is no tracheal deviation to suggest localized pneumothorax.
We can see a triangular opacity both rigth paratracheal and left cardiophrenic angle, Can be two focus of pulmonary tromboembolism?.
Best regards to Prof Cáceres.
oesophageal-pleural fistula ?
…gentilissimo professore….in AP immagine rx-trasparente in sede apicale dx, da probabile cisti aerea infetta…..alla base toracica posteriore sx, “opacità” retrocardiaca a sx, con sospetto di area libera sovrastante….clinica di dolore acuto toracico, senza febbre e-o dispnea, in soggetto con pregressa operazione chirurgica dell’esofago distale….penso ad una complicanza “tardiva” di tale intervento a carico del segmento intestinale utilizzato per anastomizzare l’esofago residuo allo stomaco….complicanza di natura “ischemica” il che potrebbe spiegare il dolore “acuto” a febbrile…ischemia con perforazione del segmento intestinale….
i suggest esophageal rupture causing pneumomediastinum
the heart is outlined by a thin lucent lint and there is a suspicious lucency seen overlying the left cardiac shadow could represent naclerio v sign.
also on the lateral view there are lucent lines outlining the mediastnal structures
these findings likely represents pneumomediastinum and from the surgical clips seen and the history of the patient likely the cause is reputed oesophagus
How come that nobody is looking at the pulmonary vessels?
Putting it in a different way: what do think (and look for) in a paient with acute chest pain?
….se dobbiamo guardare i vasi polmonari….essi sembrano collegarsi con la opacità basale sx…..allora una MAV?
You are a clinical radiologist. Use your clinical common sense.
…..infarto polmonare….
Right apical oligemia suggesting pulmonary embolism?
Right Apical Bulla
Left Pulmnory Artery Embolism /Infartion Lower lobe
Pulmonary Embolism
…..grazie mitico!!!!NB il Bari è ai play-off per salire in serie A…Aspettaci BARCA!!!!!