Muppet has insisted in presenting the following case: radiographs of a 48-year-old male with cognitive problems and episodes of amnesia. What do you see? What would be your diagnosis? Leave us your thoughts in the comments section and come back for the answer on Friday.
Findings: PA radiograph shows an obvious increase in size of the LUL vessels (Fig 1A, arrows). The lower lobes are oligemic and the calibre of vessels is decreased (Fig 1A, red arrows).
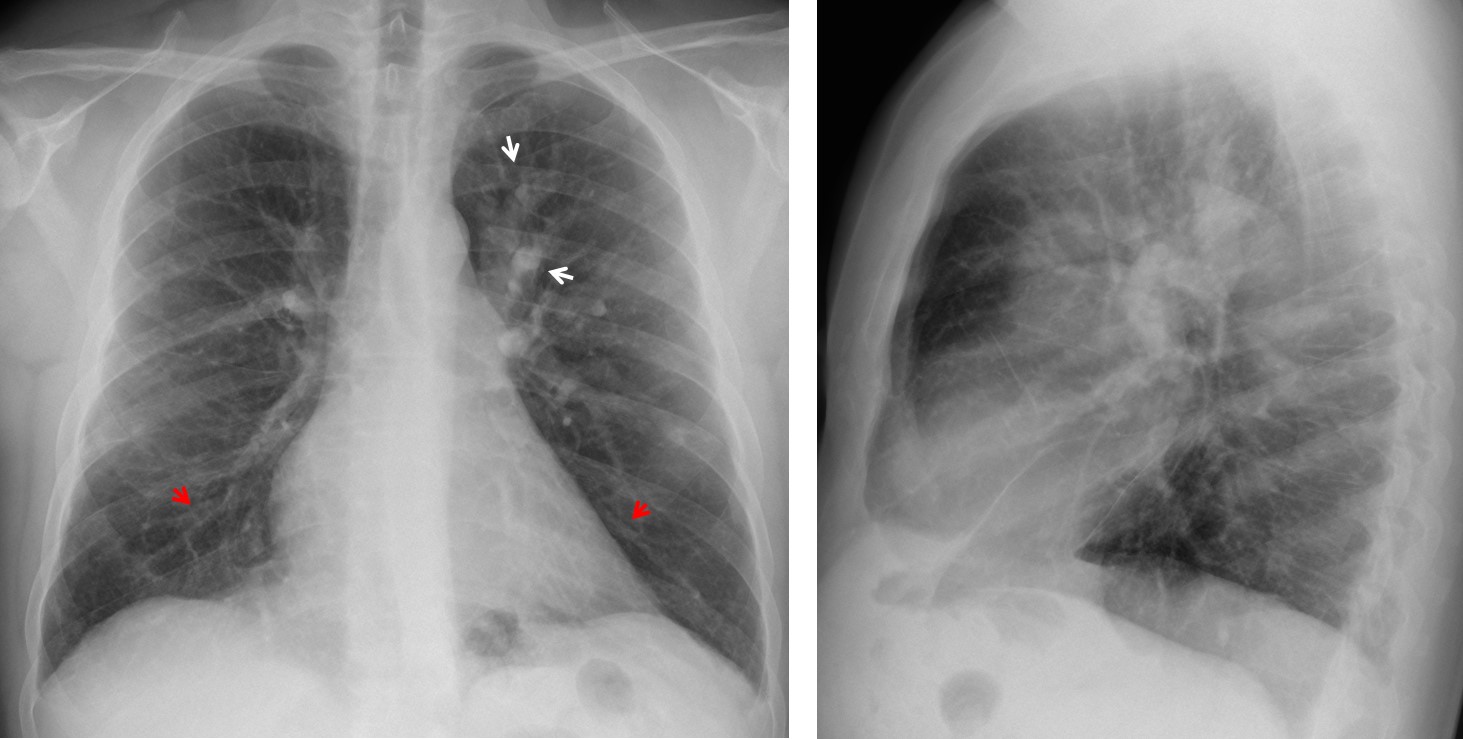
Fig. 1
These findings suggest a widespread vascular abnormality. The first possibility that comes to mind is chronic pulmonary embolism, but the hila are not enlarged and the heart looks normal. There are no signs of pulmonary emphysema, either. An uncommon possibility is pulmonary arteritis, supported by the clinical fact that the patient had neurologic symptoms. Further investigation discovered that the patient had been diagnosed with Takayasu’s disease eleven years earlier. At that time, CT (not available) discovered obliteration of lower lobe arteries and dilatation of LUL arteries. MRI was done and confirmed the findings (Fig 2).
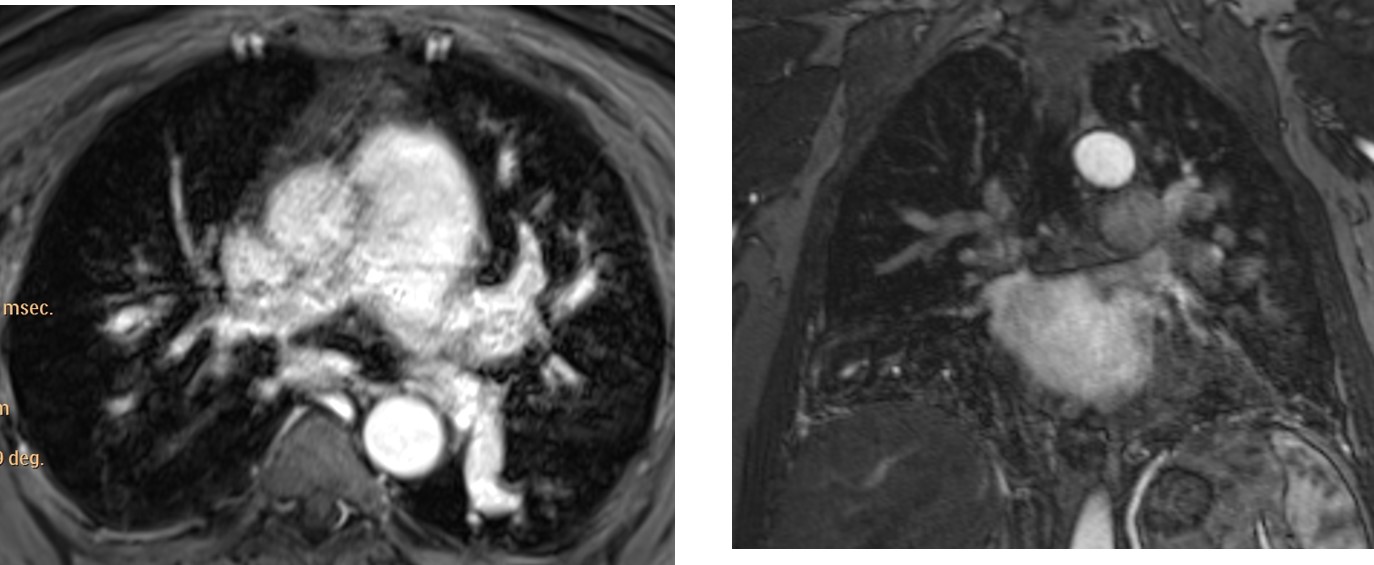
Fig. 2
Neck MRI showed occlusion of the left carotid artery (Fig 3, arrow).
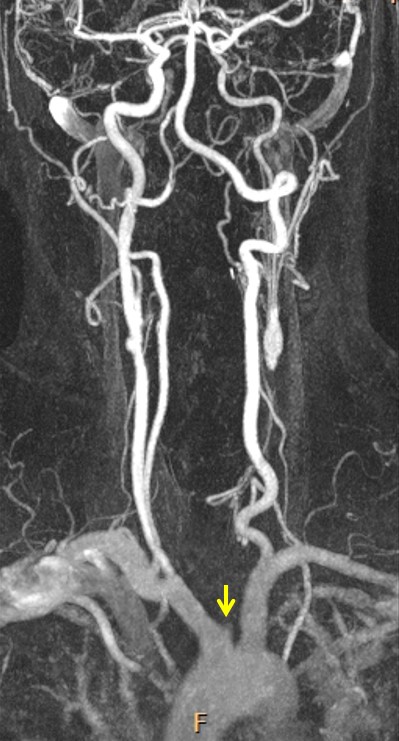
Fig. 3
Final diagnosis: Takayasu’s disease affecting pulmonary vessels.
Congratulations to Genchi Bari and Laurens who got close enough and deserve recognition.
I realise this is a difficult case, but Muppet made me do it! We have been waiting to show it ever since we saw the plain films in January. MRI was done two weeks ago and confirmed the findings.
Teaching point: vasculitis has variable manifestations. Think of vasculitis when several organs are affected and you don’t find a clear link.
This is the last case of the semester. I am leaving on vacation and Dr. Pepe will remain one more week to present the last Diploma case next Monday. I wish you all a happy summer vacation!



Venous pulmonary hypertension and lingular atelectasis.
There seems to be a bulge in the left side of the heart, left atrial appendage maybe? It could be left atrial embolism causing ischemic strokes.
See reply to Lauren.
Increased pulmonary flow with upper zone vascular prominence.
Vessels visible to the periphery of the film. Heart size normal. Left atrial appendage prominent. This could indicate left to right shunt, possible ASD.
Review Dr. Pepe’s Diploma nº 52. It tells you whether or not there is bulging of the atrial appendage.
Thank you Professor, atrial appendage is ok. Is pulmonary flow more prominent on the left side?
What do you think?
I think that the left side has more prominent pulmonary flow.
More prominent blood flow on the left could mean pulmonary stenosis. I am thinking of other differentials.
I am adding a possibility of left basal bronchiectases causing plethora of the upper lobe vessels on the left.
And Blalock-Taussig shunt.
pulmonic valvular stenosis with post sténotic dilatation
Prominence of the pulmonary arch especially dilatation of the left pulmonary artery and increased of the pulmonary vasculature. PAH
(left-to right-shunt)?
No the heart size is normal.
chronic pulmonary emboli?
And hiatus hernia
Main question I am asking why is there more prominent pulmonary flow on the left than on the right. I will stay with my first suggestion of left to right shunt and say there is a possibility of patent ductus arteriosus ( in ASD we would have bilateral increase of blood flow, not unilateral). Other differential will stay pulmonary stenosis (possible jet effect).
Does the clinical history help you?
Cognitive problems and episodes of amnesia – I am thinking of a Down syndrome.
AVSDs are often. Tetralogy of Fallot and PDA can also occur.
No Down. Keep thinking.
….stimatissimo Professore….il punto è spiegarsi l’iperafflusso “distrettuale” in campo polmonare superiore sx e la patologia cerebrale(primitiva o secondaria?)….Escluse le cause “classiche” di ridistribuzione del circolo(Scompenso cardiaco-enfisema polmonare) resterebbe l’embolismo…ma il territorio ipoperfuso, in questo caso il lobo inferiore, è normale( assenza segno di W.)….resta pertanto una causa locale…è chiaro che la diagnosi è fatta con angio-TC, ma possiamo ipotizzare un processo produttivo neoplastico(angiosarcoma) con successive metastasi cerebrali? Fantasia??? Tutti i grandi calciatori infatti sono ottimi fantasisti!!!Un abbraccio.
Your theory is interesting, but is not the right diagnosis. Consider a pathologic process that may affect different organs.
….tromboembolia polmonare da Lupus Eritematoso Sistemico: da auto-anticorpi anti-fosfolipidi.Encefalite e tromboembolismo polmonare….ancora fantasia?
Close enough. Will give you credit.
Tuberous sclerosis?
As far as I know, tuberous sclerosis gives disseminated interstitial changes.
See the answer to Genchi Bari and go back to square one.
….grande Barca….grande Bari( anche se restiamo in serie B!)….
My shunt propositions ended in total failure.
I was thinking of a new idea: it could be vasculitis,
like Behçet’s disease.
Hi,
As to the rule KISS – the most often seen cause of unilateral vascular lung anomaly is pulmonary embolism. This could go with the mental deterioration syptoms caused by multiple embolic infarcts.
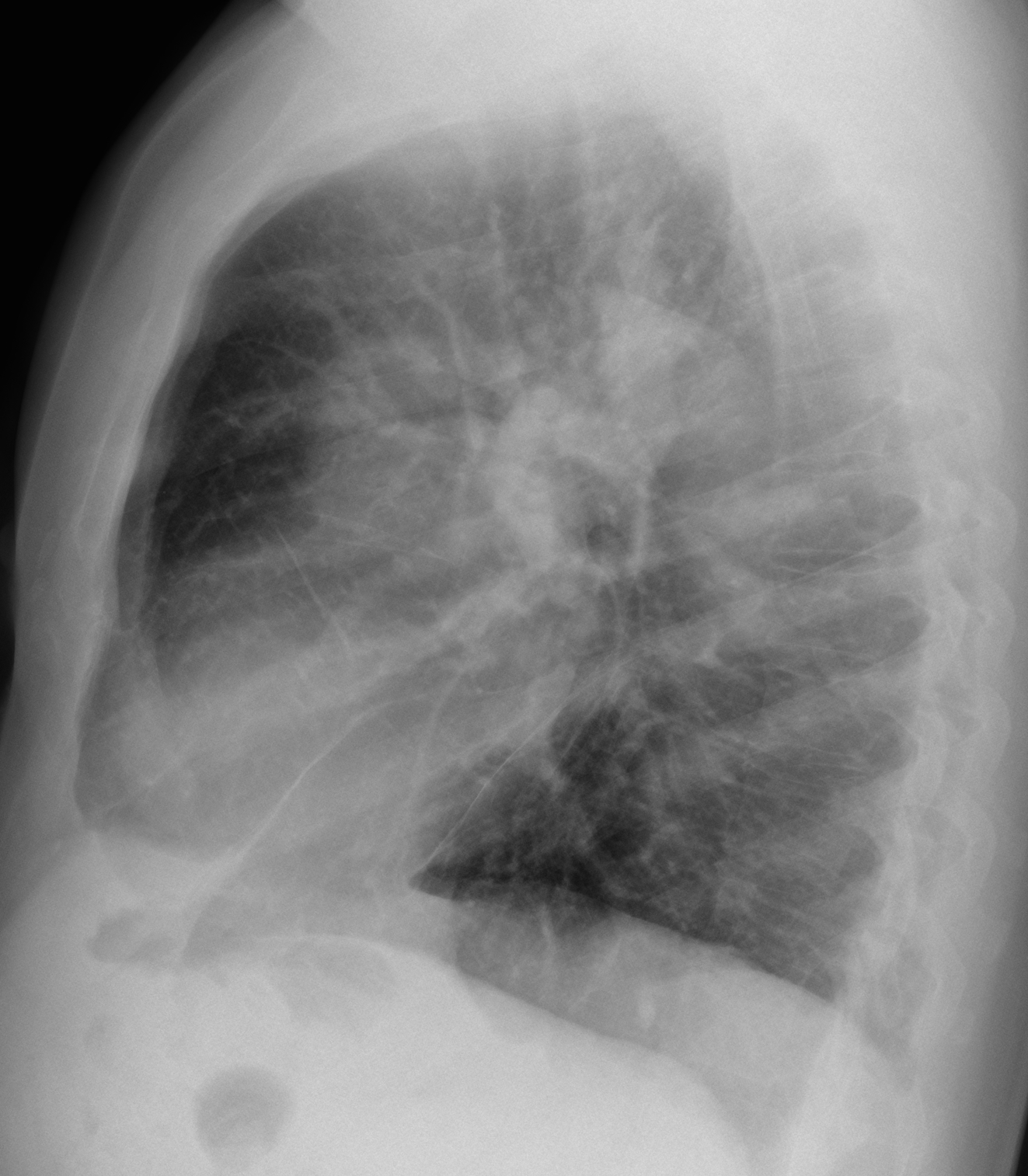
I am worrying about shape of the aorta on lateral view.. why it is so opaque at the arch/descending part? it is not contiguos but has “step”.. Could it be dissection pressing the left hilar structures – including the left pulm artery? and then – possible disscention and thrombosis in carotic artery – giving neurological symptoms?
You are right about pulmonary embolism. But it is not the correct diagnosis in this case. Heart is normal and hila are not enlarged.
This is an unusual disease. Answer tomorrow.
Langerhans cell histiocytosis ?
SLEEP APNEA SYNDROME WITH PULMONARY HYPERTENSION
For me is a lung and characteristics of enmphisema, athelectasias, loos of the pulmonar arc, because I think in a poor concentratión by oxigen. Too exist central hiperdensity and great posterior hiperdensity in the place of left appendege that is posterior, is posssible tha atrial chronic fibrilation and samall multiples infarcts in the brain
I´m according to Lauren. Could it be any vasculitis? Probably Behçet’s disease.