Muppet wants to start the new season with a warm-up case, provided by my good friend and former resident Carles Vilá. Images belong to a 62-year-old woman who has had a dry cough for the last six months. Chest radiograph was normal and a CT was taken.
1. Coin
2. Chicken bone
3. Pencil lead
4. None of the above
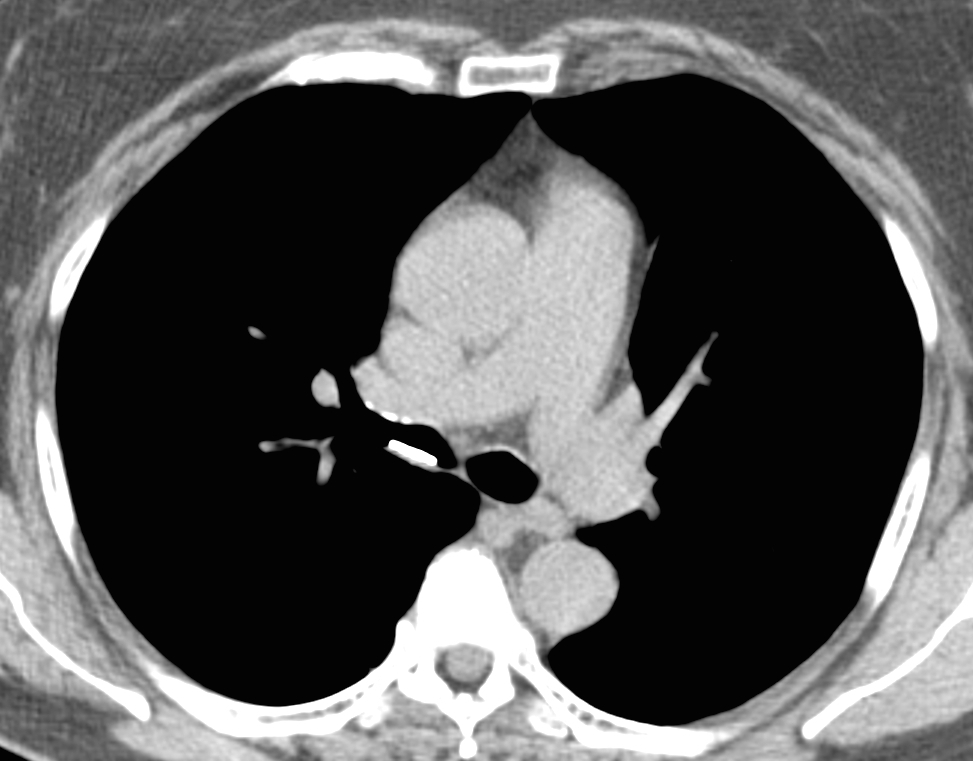
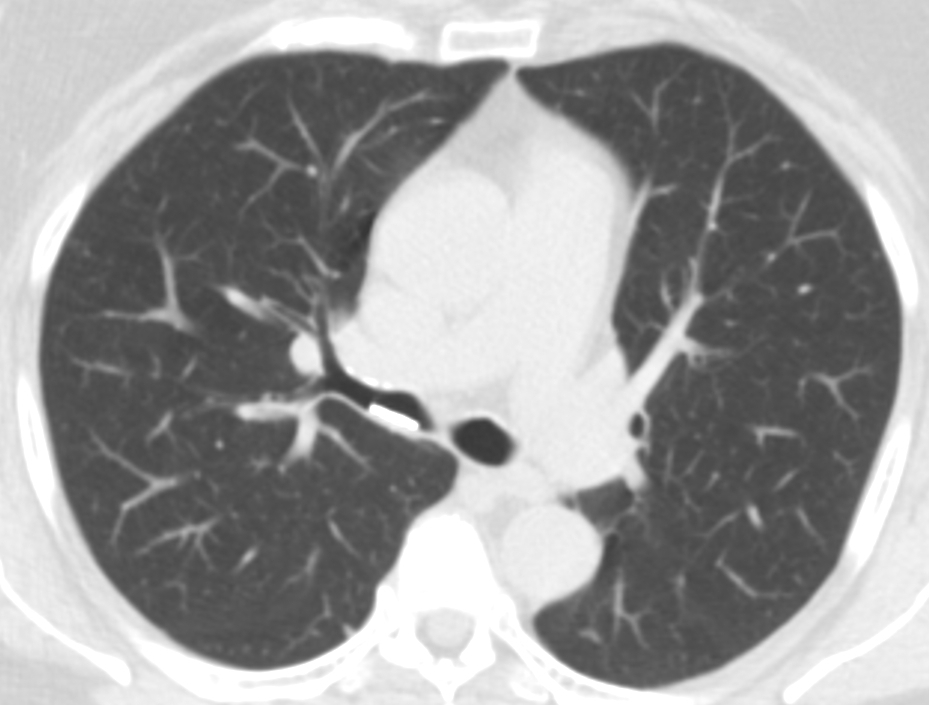
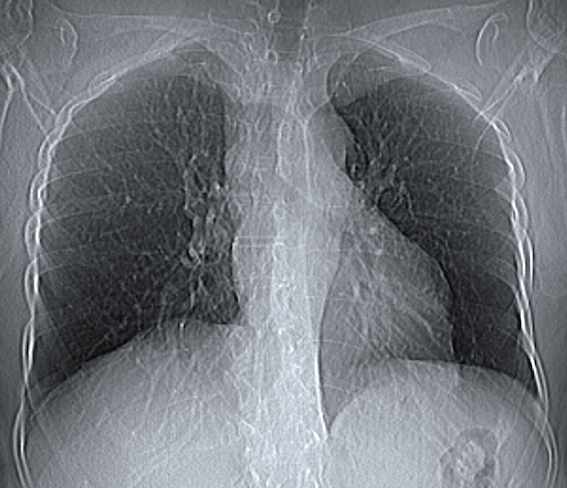
Findings: axial CT shows a linear metallic opacity within the intermediate bronchus (A, B arrows). Coronal CT reconstruction shows that the metallic opacity is rounded (C, arrow) and, in retrospect, can be seen in the scout film (D, arrows). At bronchoscopy a coin was found (insert).
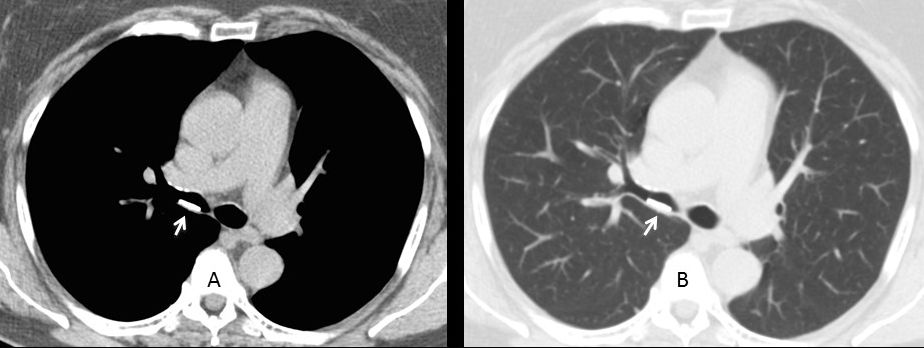
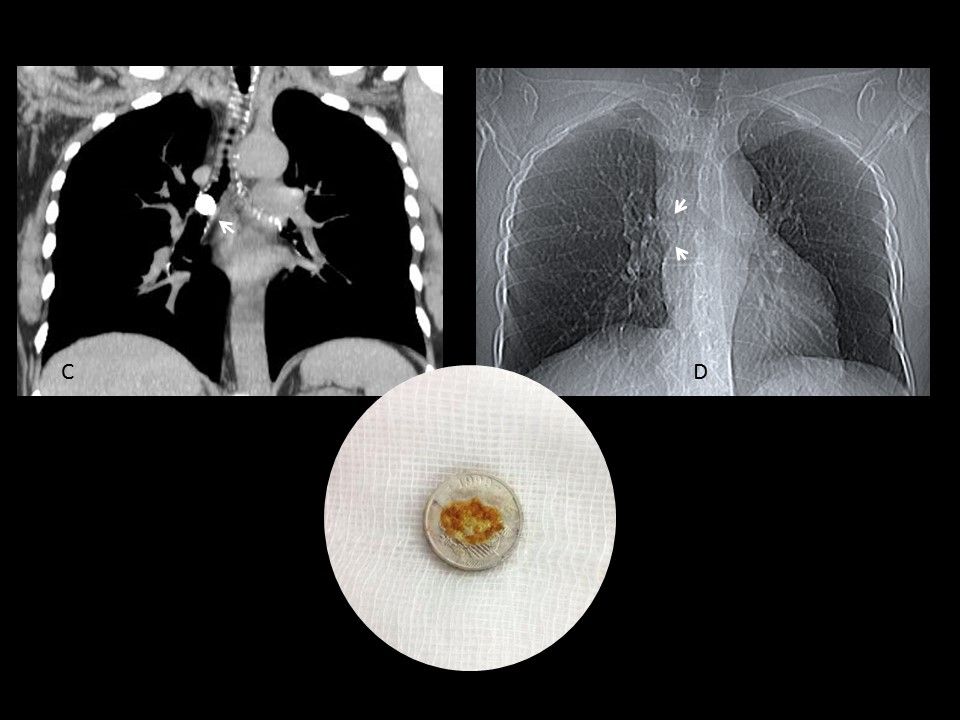
Final diagnosis: foreign body (coin) in intermediate bronchus.
Congratulations to Gus, who made an early and accurate diagnosis.
An interesting aspect of this case is the lack of detection of the coin in the chest radiograph and scout film. The coin is a Spanish peseta, made of aluminum with a weight of 0,55 grams and 14 mm of diameter. Its small size and aluminum’s low density makes the coin undetectable when imagined en face.
Another interesting point is that this coin was minted in 1999 and ceased circulating in 2001, after the arrival of the euro. Was it in the bronchus since 2001 until 2014 when it was discovered? To increase the mystery, the patient’s husband is a coin collector, casting doubts about the date of the aspiration.
Teaching point: remember that foreign bodies in adults are uncommon, but may happen, as proven by this case.



4.
welcome back professor
my answer ia :a coin
Welcome back, Gus. Why do you think it’s a coin?
because the shape and the density.
i can see the coin on the right main bronchus on the chest radiograph too .
This is not a coin or pencil lead, as it would be seen in the chaest radiogram. It doesn`t look like chicken bone as well, so answer is 4- none of above. I suggest performing a bronchoscopy:)
Your suggestion was carried out and bronchoscopy performed. Afraid you have to wait for the answer till Friday!
welcome back sir
i think its bronchial wall lesion
It does not produce beam hardening artifact nor does appear clearly in the chest radiograph, so I asume that is calcium density, and not too much of it.
With that morphology I could be a broncolith. The positions looks good to me too.
So my answer is 4. Broncolith maybe.
Welcome back professor!!!
I think it’s a calcified plaque in the bronchial wall,as there are calcified foci on the opposite (ventral) bronchial wall.
The calcium in the ventral wall has no significance. Probably secondary to advanced age.
On the topogram I can’t see any metal intensity projections in that area. So it might be a pencil lead aspirated and stuck into the wall of the right bronchai, so option 2 for me.
Inwards calcifications of the bronchial wall is rather seldom.
1. History of foreign body aspiration is absent!
2. Bronchial wall calcification is seen i.e it seems to be a chronic process.Since bronchial wall calcification is seen in both bronchi, a local foreign body reaction may be ruled out since they will be unilateral.
3. Answer seems to be option 4.
4. Bronchoscopy will help.
Although foreign bodies in adults are not frequent, a history of previous aspiration is not always elicited.
It has the same density as patient’s bones (ribs and vertebres). So why not chicken bone? It’s interesting to know bronchoscopy results=)
4. It’s location and its regular shape with sharp borders all suggest an aspirated foreign object. It’s shape is too regular for a bone; too thick for a conventional coin, which would also show up on X-ray; I also assume pencil lead would show up on X-ray.
It would obviously help to see the object’s profile on other CT axes, but with the combination of its size, radiodensity on CT, and lack of visibility on plain film, it seems most consistent with a chewable tab of calcium carbonate (if profile was round on coronal view), or potassium chloride (if coronal profile was identical to axial profile). It’s too big to be any other med. Only problem, it seems highly improbable that either would have survived 6 months without being dissolved – unless the symptom duration is a red herring.
Excellent discussion. Duration of symptoms is correct (according to patient), although I am sure that you have seen a patient with a large breast mass, that states that the mass appeared two weeks earlier.
#4. No metal in axial or scout. No collapse or other effects of obstruction
I think it’s a coin: even if it has not clear hardening artifact in the ct-scan (copper? zinc?), it is leaning down into the bronchus and in the scout-view it has a clear round shape!
Good. Congratulations
High-densitiy aspirated foreing body in the right main bronchus without beam hardening and not clearly visible in the CT topogram. I think it could be a medical tablet.
A MPR would be of help for selecting the right answer 😉
….scusa MITICO…..sono arrivato in ritardo dalle vacanze!!!!Non ti dimentico e sarò in “campo” dalla prossima partita!!!!
Welcome back. Looking forward to your collaborations.