
Dear Friends,
With your welfare in mind, Muppet has selected this week’s case. Radiographs belong to a 76-year-old woman, admitted to the hospital with moderate fever and vomiting.
Diagnosis:
1. Aspiration pneumonia
2. Tracheomegaly and pneumonia
3. Pneumonia and pericarditis
4. None of the above

Click here for the answer to case #98
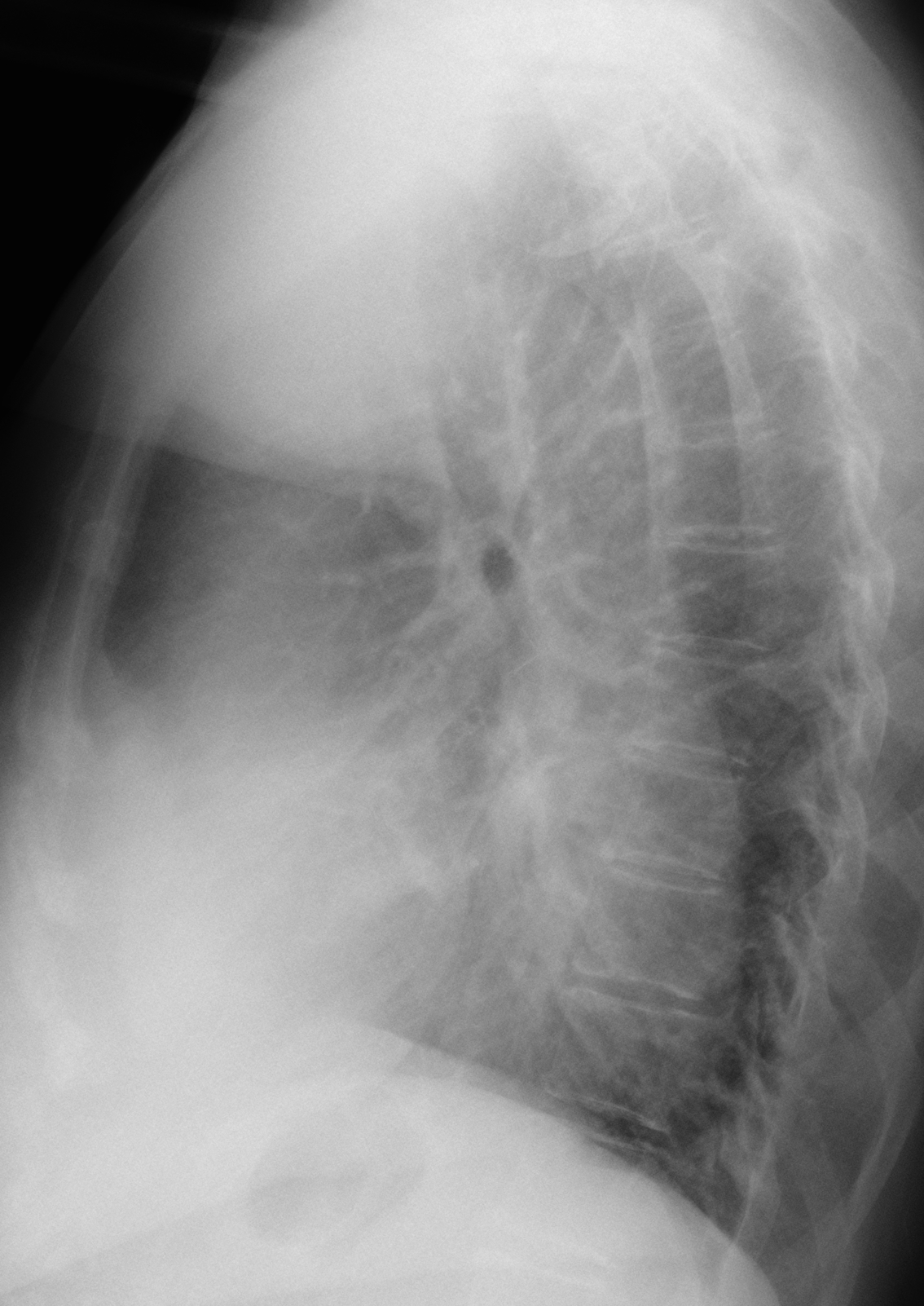
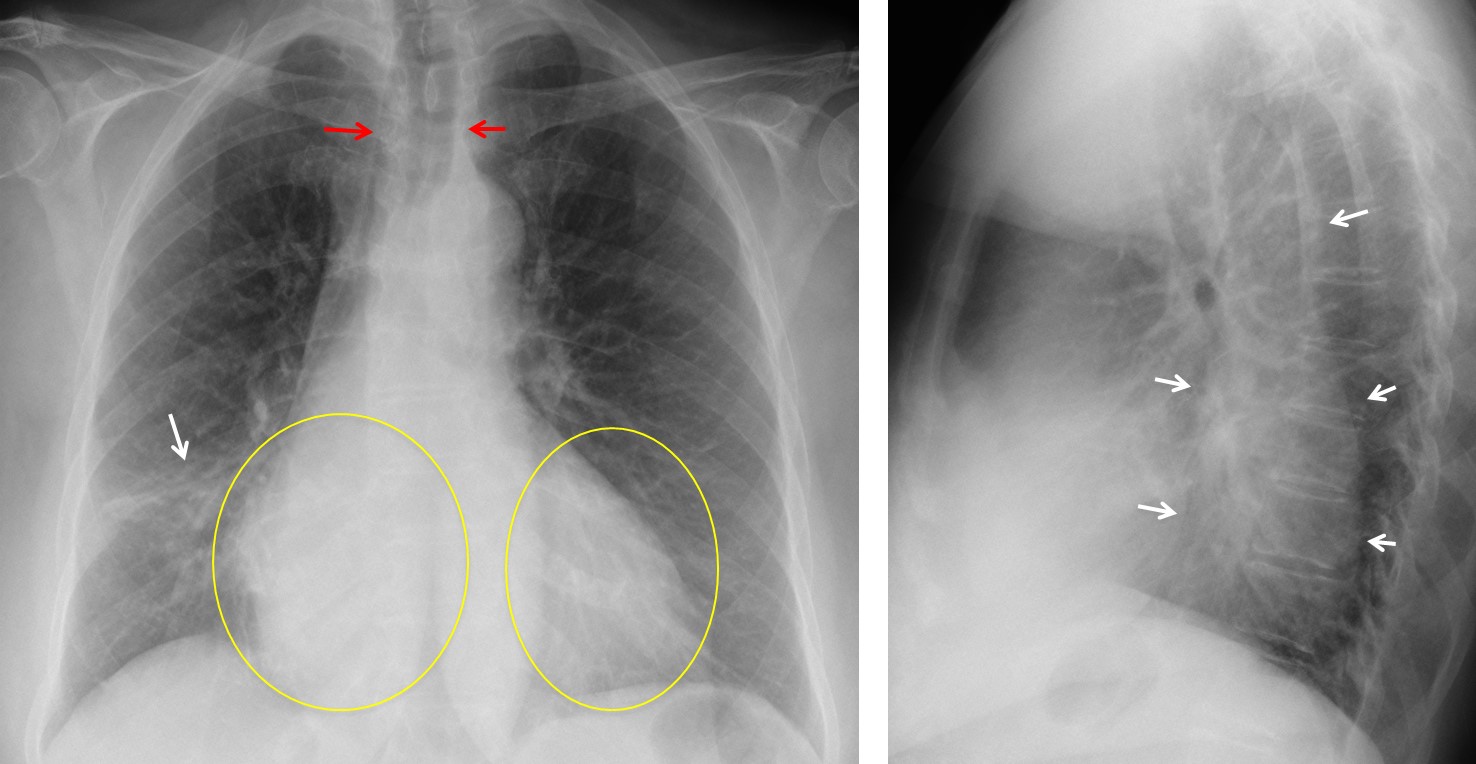
Findings: PA chest shows an RML infiltrate (arrow). There is also increased density of the right side of the heart compared to the left (circled areas), due to superposition of an elongated sausage-shaped density behind the heart in the lateral view (arrows). These findings are indicative of a dilated oesophagus, which is seen as an air-filled structure in the upper mediastinum (red arrows).
Coronal and sagittal CT confirms the dilated oesophagus (arrows), full of undigested food. Note the dilated air-filled upper oesophagus (red arrows) Oesophagoscopy demonstrated achalasia. No distal tumour was found.
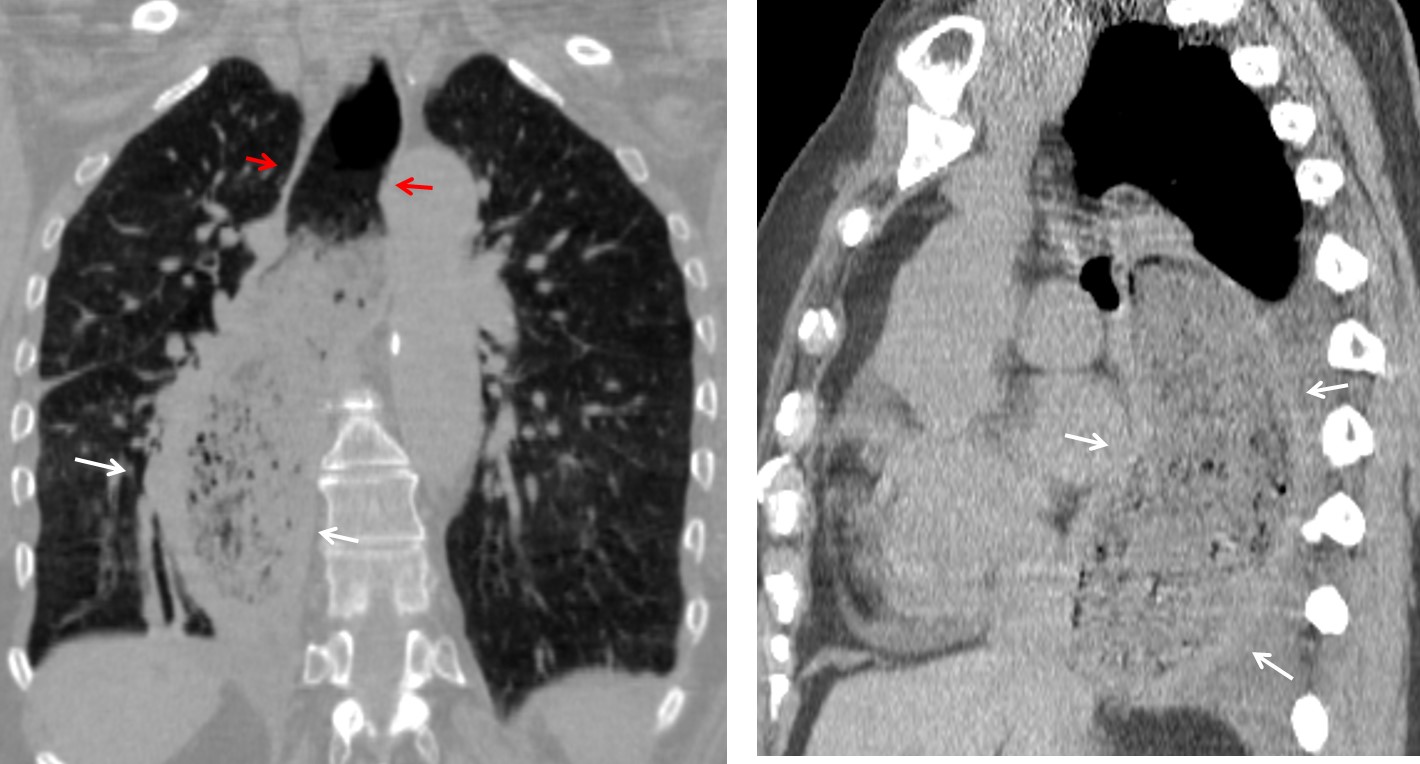
Final diagnosis: achalasia with aspiration pneumonia.
Congratulations to Adam and Jonathan who were the first to suggest the correct diagnosis.
Teaching point: when seeing a structure that traverses the middle mediastinum from top to bottom, always consider the oesophagus, with the descending aorta as the second possibility.


Me parece que neumonía y pericarditis es la correcta. Saludos desde Chile
Bienvenido. Pronto tendremos un blog en español.
Aspiration pneumonia
Any previous surgery? Does the patient have a pull-up stomach?
No previous surgery.
Achalasia and aspiration pneumonia
Dilated esophagus for sure with probable aspiration pneumonia. Given age, I would guess pseudoachalasia from gastroesophageal adenocarcinoma. I would move onto CT first to look for possible fistulous connection between esophagus and airway/lung.
JC
mediastinitis?
Greetings sir…
Looks like Aspiration pneumonia …
RLL pneumonia
Neumonía lóbulo medio
Condenstation of the RML, clinicaly it might be an aspiration pneumonia of the middle lobe. Decending toracic aorta on the lateral view is shifted post. idicating a mass located retrocardiac, it can be an enlarged distal oesofagus or an atipical pericarditis as you can observe almoust entire cardiac siluete on the lateral view. I vote for option no 3. An Iopamiro enema with would help in case of a oesofagus bronchai fistula.
Did you notice the right side of the heart is more opaque then the left on the PA? This would be unusual in pericarditis
There is clearly something retrocardiac that is pushing the decending toracic aorta posterior. I agree with genchi, it might be a leiomioma of the oesofagus. Fever can be explained by the pneumonia, but the vomitig must be from a longer time if there is a leiomioma, as they tend to grow slow.
…”pseudo-cancellazione” del disegno vascolare polmonare, in PA,a livello della silhouette cardiaca di dx, da parte di una opacità, fusiforme, densa ed omogenea che sembra connettersi con l’esofago superiormente leggermente ectasico…potrebbe trattarsi di un leiomioma esofageo…
I think Jonathan may be right. The esophagus appears dilated, suggestive of achalasia, but it’s only the prox esophagus. The patient appears to have either a middle mediastinum mass with posterior extension, or posterior mediastinal mass with anterior extension. Overall, I’d say a mediastinal mass with mass effect on the distal esophagus – may be an esophageal cancer, but also could be an mass extrinsic to the GI Tract.
The whole esophagus is dilated. Look at the air-filled upper esophagus in the PA film.
i see the opacity on the right cardiac side (silhouette sign )ok
On the lateral view i think there is posterior dispacement and widening of right main bronchus. maybe a fistula?
….e se fosse un aneurisma fusiforme dell’aorta discendente ?
Aneurisms go to the left, esophagus to the right. And the opacity in on the right side on the PA film
Aspiration pneumonia
Enlarged esophagus due to Esophageal cancer and fistulas made with the right lung,which causes pneumonia with fever and vomiting.
Ah ok it’s not 🙂