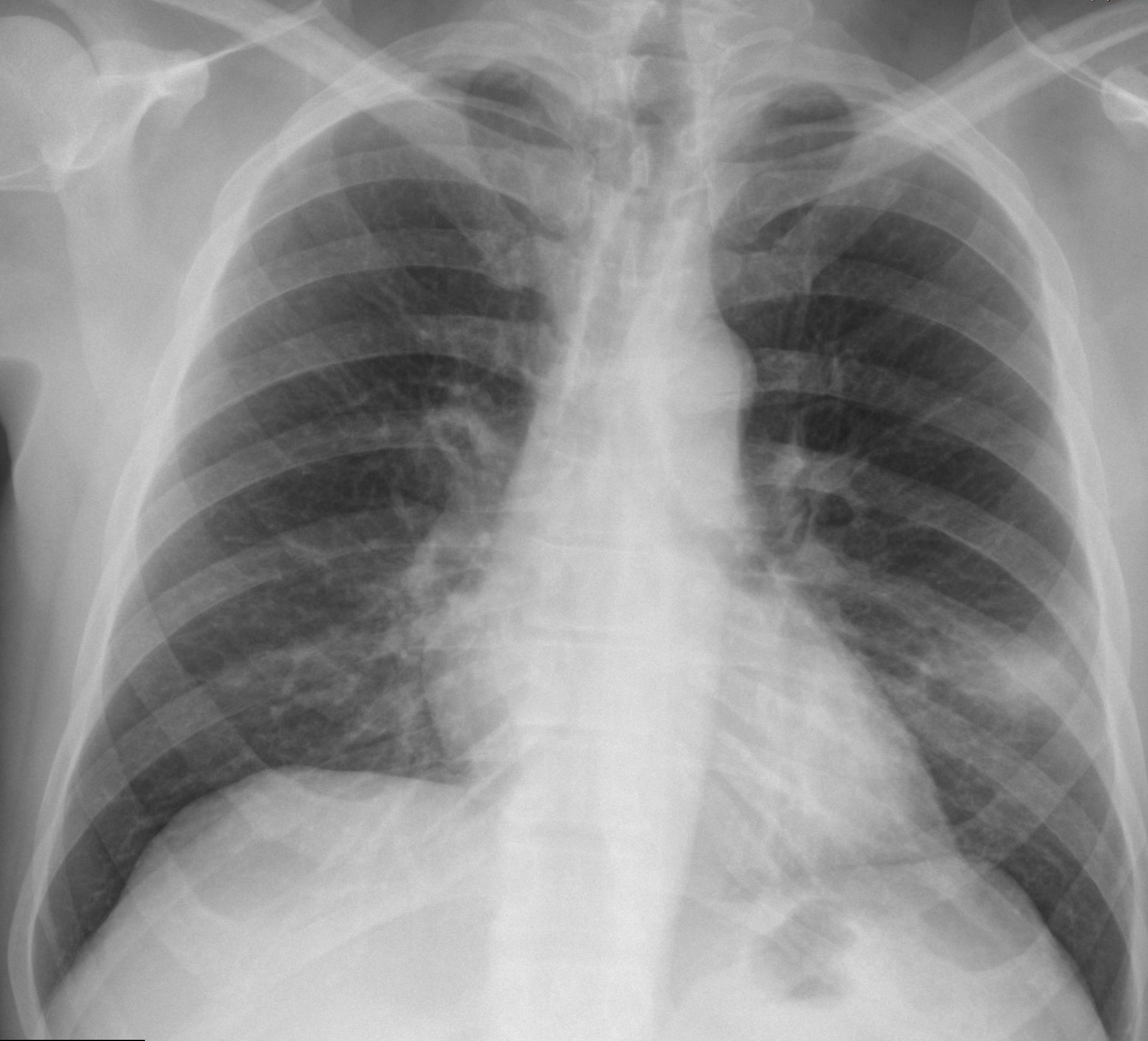
Muppet is very excited because case 100 is only two weeks away. In the meantime, he wants to present a simple case that we saw one month ago. The radiographs below belong to a 53-year-old man with cough and fever. What do you see?
Leave your thoughts in the comments and come back on Friday for the answer.
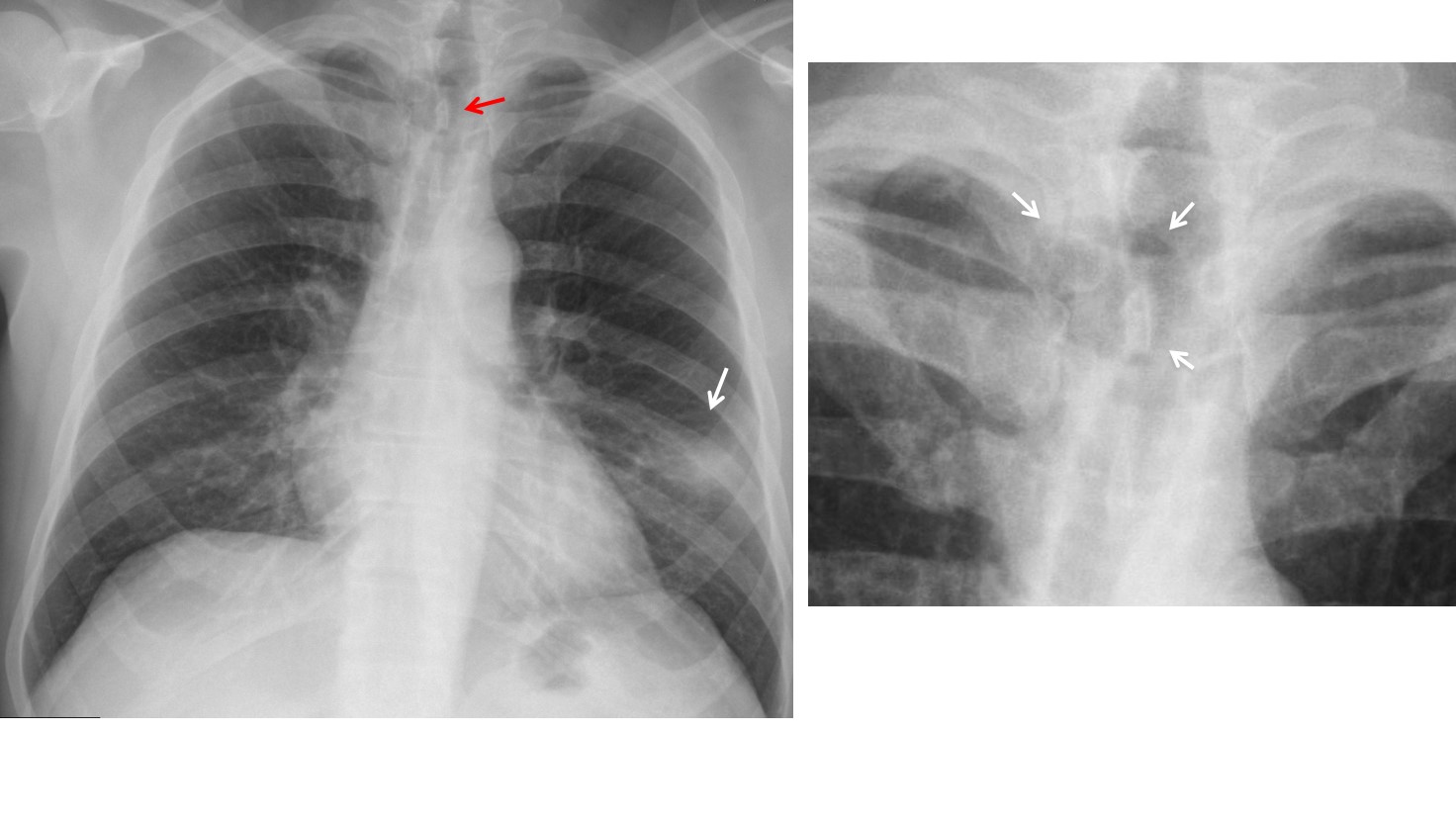
Findings: PA radiograph show a segmental air-space opacity (A, arrow) which, given the clinical information, represents most likely a pneumonia. In addition there is buckling of the upper trachea (A, red arrow). The cone down view shows the tracheal angulation and a rounded air-filled structure at this level (B, arrows).
Answer – A & B
Axial and coronal CT confirm the presence of a diverticulum impinging on the trachea (C, D arrows).

Answer – C & D
Tracheal diverticula are uncommon and incidental findings, found in less than 1% of patients at autopsy. Usually asymptomatic, occasionally they accumulate secretions that may became infected.
Final diagnosis: Segmental LLL pneumonia and tracheal diverticulum
Congratulations to Genchi Bari, who made a good diagnosis
Teaching point: always look at the trachea in the PA and lateral films. You may discover interesting pathology.



Patchy opacity is seen in left lower lung zone with distal oligemia and right hilum shows filling defect in pulmonary artery giving like appearance of “Tram track ” sign.
Overall findings suggest Pulmonary Thrombo-embolism with Westermark sign
Pseudotumour- small amont of fluid in left interlobular fissure, maybe with some adjacent discrete consolidations (infectious?)
LLL opacity of subcostal intensity limiteed to the oblic fissure, relativly homogenous with difuze borders.
DD: round pneumonia, pneumonia in the early stages.
Good diagnosis. Is there anything else?
….la non invasione della scissura esclude una formazione maligna….in LL essa sembra alimentata da strutture vascolari ipertrofiche…..penso allora, contro l’opinione dei colleghi, possa trattarsi di una MAV( malformazione artero-venosa)….comunque , prima della TAC, opportuno un ciclo di terapia antibiotica e controllo RX…
I agree with your comment about the lack of invasion of fissure. Is there any other finding in the chest?
Have you all forgotten the satisfaction of search?
….mi sembra che a dx, ci sia un “rimaneggiamento” dell’arco anteriore della 3 costa .nonché una immagine pseudo-tubulare a livello ilare…
I think there is dilatation of the right main bronchus and bronchial wall thickness.
I see the opacity of the LLL with downward displacement of the left hilum and a small elevation of the left hemidiaphragm.
sorry not the right main bronchus…the left
Look higher
…a livello ilare sx, due immagini aeree, prospicienti due immagini vascolari…..possono essere bronchiectasie…
…la trachea in alto a dx ,appare deviata ed improntata…..bronco tracheale?
Good answer!
Amputation of the left pulmonary artery with left perybronchial nodular opacities, subcostal intensity, homogenous ( enlarged left peribronchial lymphnodes ) +/_ left arterial venous malformation.
Apart from the upper deviation of the trachea to the left, there seems to be a round well defined radiolucent area of about 3 cm diameter at the place of th angling of the trachea, right in front of the T2.
Thank you )
Closer to the apex of the right lung I mean
Good diagnosis. See the posted answer, above.