Muppet wants to leave air-fluid levels behind and put your collective minds to work!
The first case of 2013 presents the radiographs of a 56-year-old female who came to the emergency room with syncope. There is an abnormal opacity in the aortic knob. What do you think it is?
1. Vein
2. Aneurysm
3. Lymph node
4. Tumour
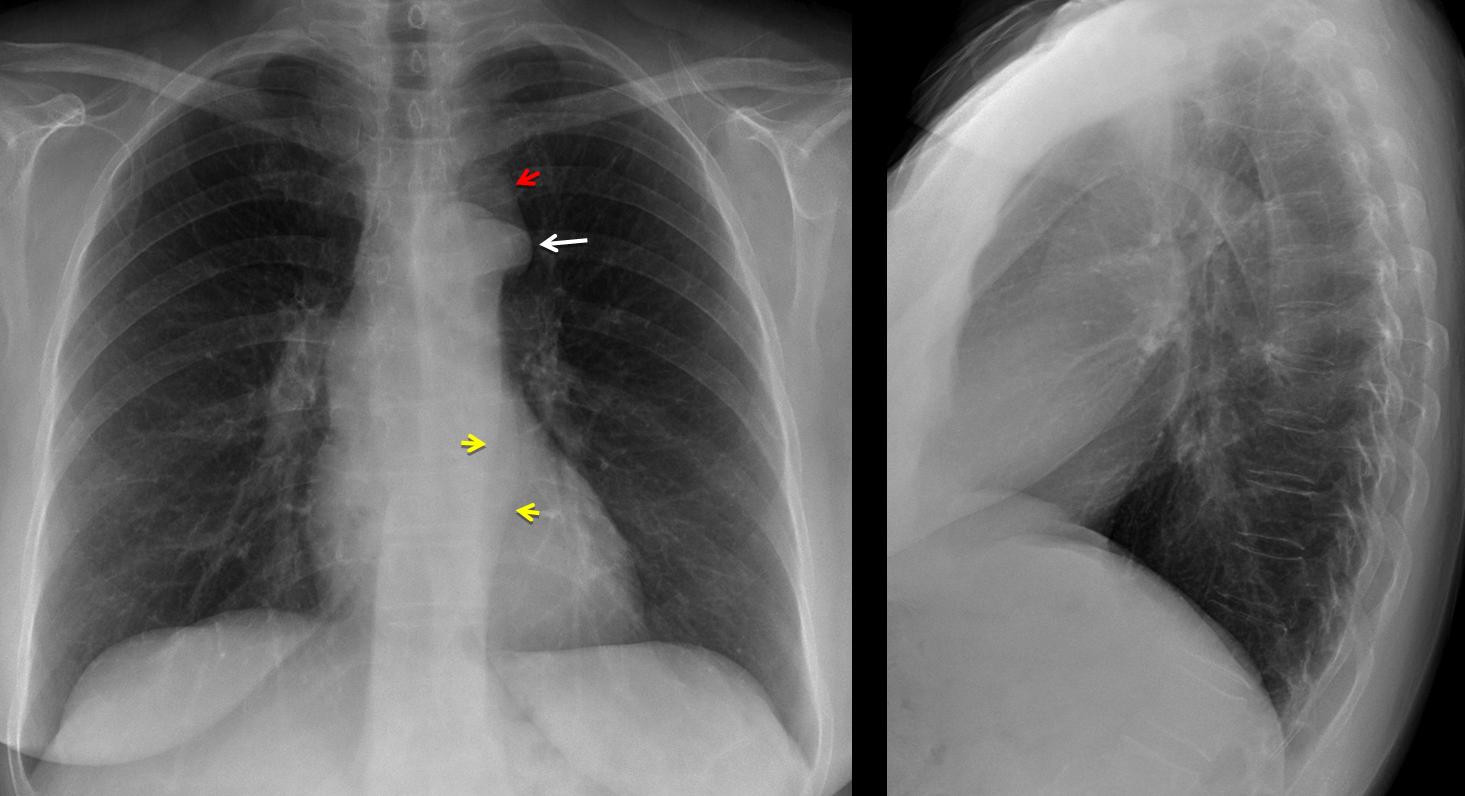
Findings: PA chest shows a rounded opacity over the aortic knob (arrow), with a faint line above it (
red arrow). There is a double contour of the left mediastinal line (
yellow arrows). SVC and azygos vein are not visible.
The rounded shadow at the aortic knob is a typical aortic nipple, secondary to an enlarged left superior intercostal vein (LSIV) which joins superiorly (
red arrow) the brachiocephalic vein and inferiorly the hemiazygos vein (
yellow arrow). Absent SVC is associated to syncope, secondary to arrhythmias. In this patient, a good possibility is absent SVC with drainage of the blood trough the hemiazygos system.
Axial CT confirms the absent SVC (neither right nor left) and the enlarged LSIV. CT reconstructions show the hemiazygos vein (arrows) parallel to aorta (A), draining blood from the brachiocephalic veins.
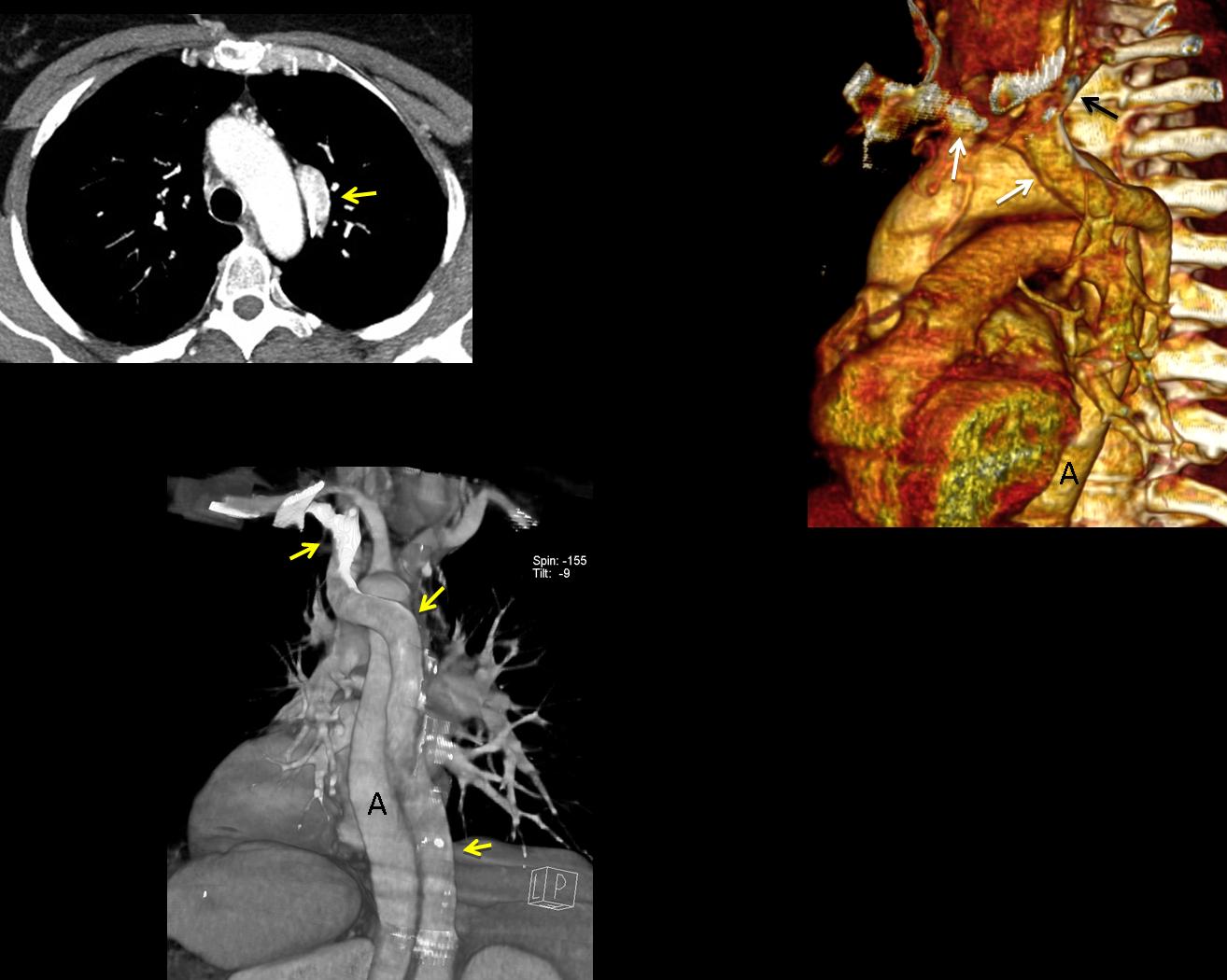
Teaching point: a small aortic nipple is a normal finding. When enlarged, suggests obstruction of SVC/IVC, with drainage through the azygos/hemiazygos system.



Anomalia vascolare come da diverticolo di Kommerel.
la diagnosi finale dovrebbe essere di malformazione venosa del ritorno venoso sistemico:assenza della VCS dx e persistenza della VCS sx. Questo dal punta di vista emodinamico, comporta una dilatazione del seno coronarico, con stiramento delle strutture del nodo atrio-ventricolare e conseguenti episodi di sincope.
2. Aneurysm. Saccular Type.
think 2. Aneurysm. Saccular Type.
A vein
A vein is a vein is a vein
This is aneurysm
Aneurysm
The azygos teardrop-like shadow is missing. Also, SVC border is not well seen. There are “two descending aortas”. One of them must be a dilated hemiazygos vein. And the opacity in the aortic knob must be the left superior intercostal vein. The left paratracheal widening could be a left SVC.
But this aortic nipple is very dilated. May be there is a hemiazygos continuation of IVC . What a mess !
By the way, link for solution case 48 is not working.
I CANT SEE THA AZYGOUS VEIN.
IT SEEMS TO BE A SECOND SILOUETTE PARALEL TO DE DESCENDING AORTA.
PROMINENT ESTRUCTURE SUPERPOSED TO THE AORTIC ARCH.
I HAVE NEVER SEEN, BUT IT SUGGEST TO ME:
ABSENCE OF THE AZYGOUS VEIN WITH SECONDARY DILATED HEMYAZIGOUS SYSTEM AND A DILATED INTERCOSTAL (NIPPLE) VEIN DRAINING TO IT.
left side SVC with azygous or Hemiazygous draining in the azygous and last option acessory hemiazygous draining in the azygous
1. vein
Collective question to Dr. Strangelove, Albert and Bruno:
Why does the patient has syncope?
il link per la soluzione del caso 48 non funziona!
la diagnosi finale dovrebbe essere di malformazione venosa del ritorno venoso sistemico:assenza della VCS dx e persistenza della VCS sx. Questo dal punta di vista emodinamico, comporta una dilatazione del seno coronarico, con stiramento delle strutture del nodo atrio-ventricolare e conseguenti episodi di sincope.
Google is awful:
Absence of the right superior caval vein has been shown by postmortem studies of infants and children to be associated with histological abnormalities of the sinus node. We report the case of a 32-yr-old man who presented with syncope due to disease of the sinus node and was found to have absence of the right superior caval vein.
International Journal of Cardiology
Volume 36, Issue 1, July 1992, Pages 115–117
Does this patient have a lef superior vena cava?
it could be a left SVC
or even a Left Superior Intercostal vein
Yes, absent right SVC and persistent left SVC, with hemiazygos system draining to it via left superior intercostal vein.
If left SVC is present why does it need a draining hemiazygos system?
I think because right SVC may be absent or hipoplasic. So the venous return with azygous would be done by hemiazigous draining in the left ( what enlarges a left superior intercostal vein).
I think Bruno is right. The question is: why is left superior intercostal vein so dilated ? Where does all that blood come from ? I suggested hemiazygos continuation of IVC. That would make this an extraordinary case, very rare.
However, there are alternative explanations. An obstruction of distal left SVC would produce a reversal flow from head and arms to hemiazygos and to IVC. Or may be it is a simple varix.
Let´s start over again and apply the KISS method.
Facts:
1. Patient has syncope, which is associated to absent SVC
2. There is an obvious hemiazygos vein
3. Would it obvious if left SVC were present?
Answering your question 3, Dr. Caceres, I think Hemiazygos continuation of IVC as Dr. Strangelove said could join all this features described before. It can be associated to cardiac malformations, left SVC and enlarged hemiazygous (heterotaxy syndromes).
Another possibility I think, but very rare is congenital absence of the azygos vein associated with left superior vena cava.
OK. The absence of the right SVC is usually associated with persistent left SVC. Excepcionally, there is no SVC at all, and blood from head and arms goes via azygos-hemiazygos to the IVC. I´ve never seen such a case but I suposse findings at chest X-ray could be similar to this case.
OK, Bruno, I think I owe you an explanation. When the azygos/hemiazygos system is enlarged it is usually due to absence/obstruction of superior/ inferior vena cava.
What I wanted you to say is that this patient cannot have a superior SVC (either right or left) because, if it were present and unobstructed, the hemiazygos vein would not be enlarged.
Isn’t magnificent? With a plain chest film we can make the diagnosis of a complex venous malformation. Plus, a pacemaker should not be inserted because the axillary veins do not connect with the right atrium. Muppet drooling!
Thank you, professor, good questions. But couldn`t this patient have a normal SVC and problems in the IVC? This image wouldn`t be the same?
If the patient had any obstruction of the IVC (congenital or adquired), the azygos vein has to be enlarged as well. Imagine IVC obstruction could be associated with azygos arch atresia, but I am not aware of this association.
After such an exciting arguments, a very few issue would remain.
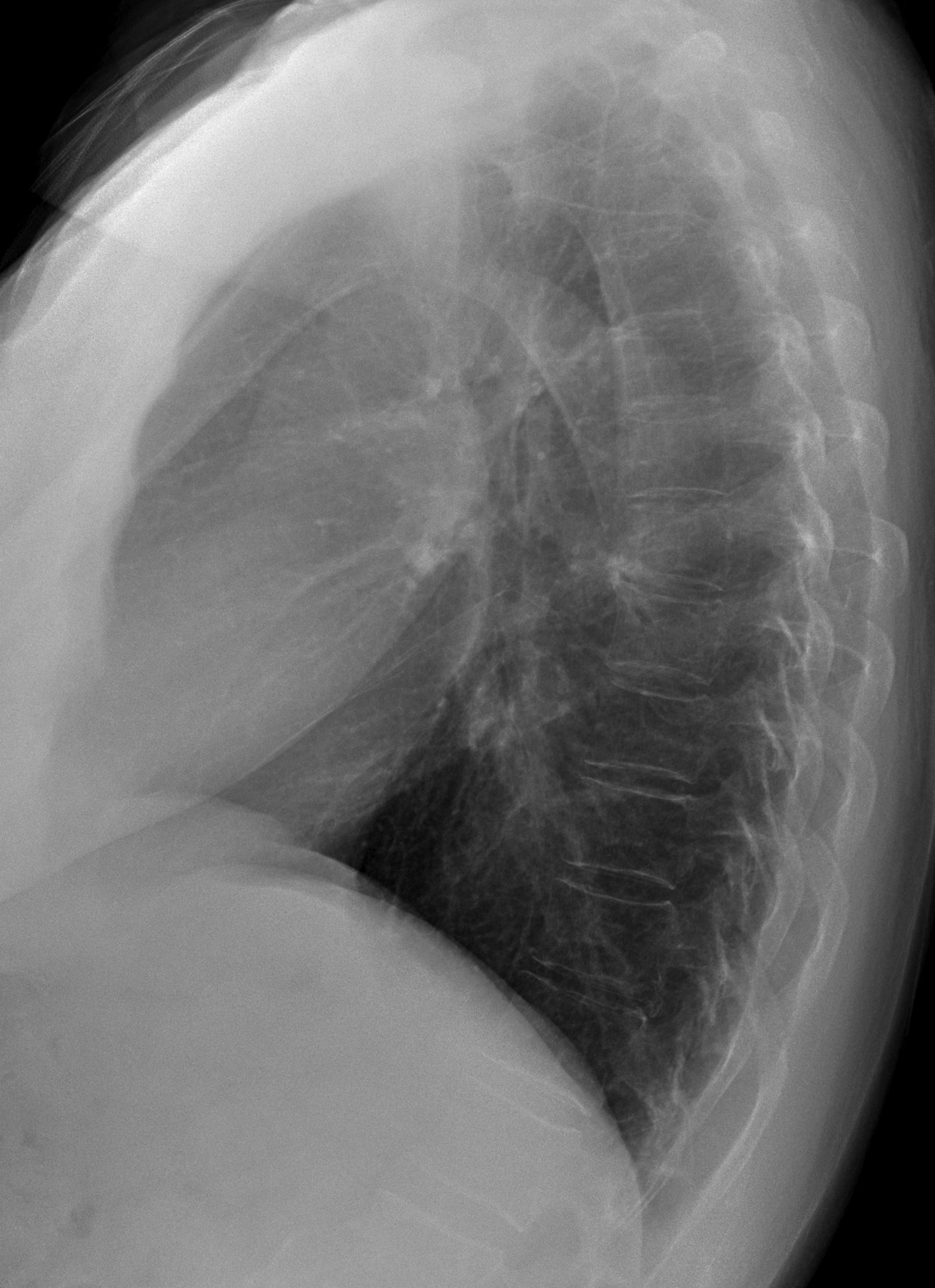
However, i’d like to point out the absence of the shadow of the inferior vena cava on the lateral X-ray. That goes with azygos or hemiazygos continuation of the IVC, hemiazygos in this case.
In the complex venous malformation, with also absence of the SVC, the dilated left superior intercostal vein makes a giant “aortic nipple”, entering the hemyazygos instead of the innominate vein.
True or Sci-Fi ?
Happy new year!
The giant aortic nipple (left superior interconstal vein) connects the innominate vein to the hemiazygos. Is the only drainage available to head and upper extremities, since there is no SVC (neither right nor left)
la diagnosi finale dovrebbe essere di malformazione venosa del ritorno venoso sistemico:assenza della VCS dx e persistenza della VCS sx. Questo dal punta di vista emodinamico, comporta una dilatazione del seno coronarico, con stiramento delle strutture del nodo atrio-ventricolare e conseguenti episodi di sincope.
Is normal the appearance of the aortic arch on lateral view?
Is not its posterior aspect like a 3? Why is it?
I believe it’s due to superposition of the dilated hemiazygos arch