Dear Friends,
Showing radiographs of a 42-year-old woman with high fever.
Diagnosis:
1. Carcinoma of the lung
2. Pulmonary abscess
3. Loculated empyema
4. None of the above

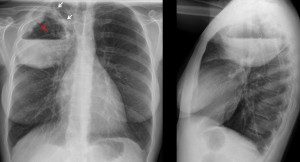
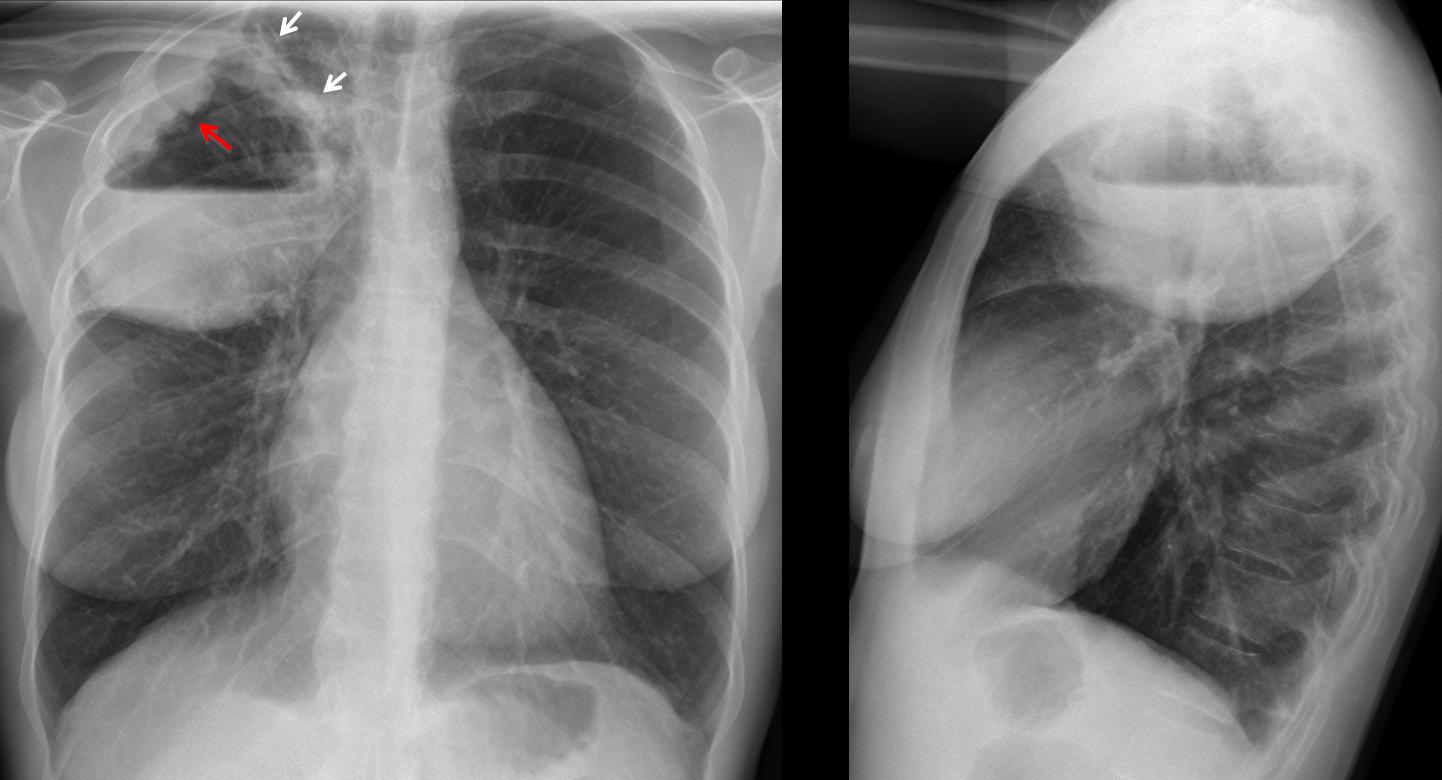
42-year-old woman, PA chest
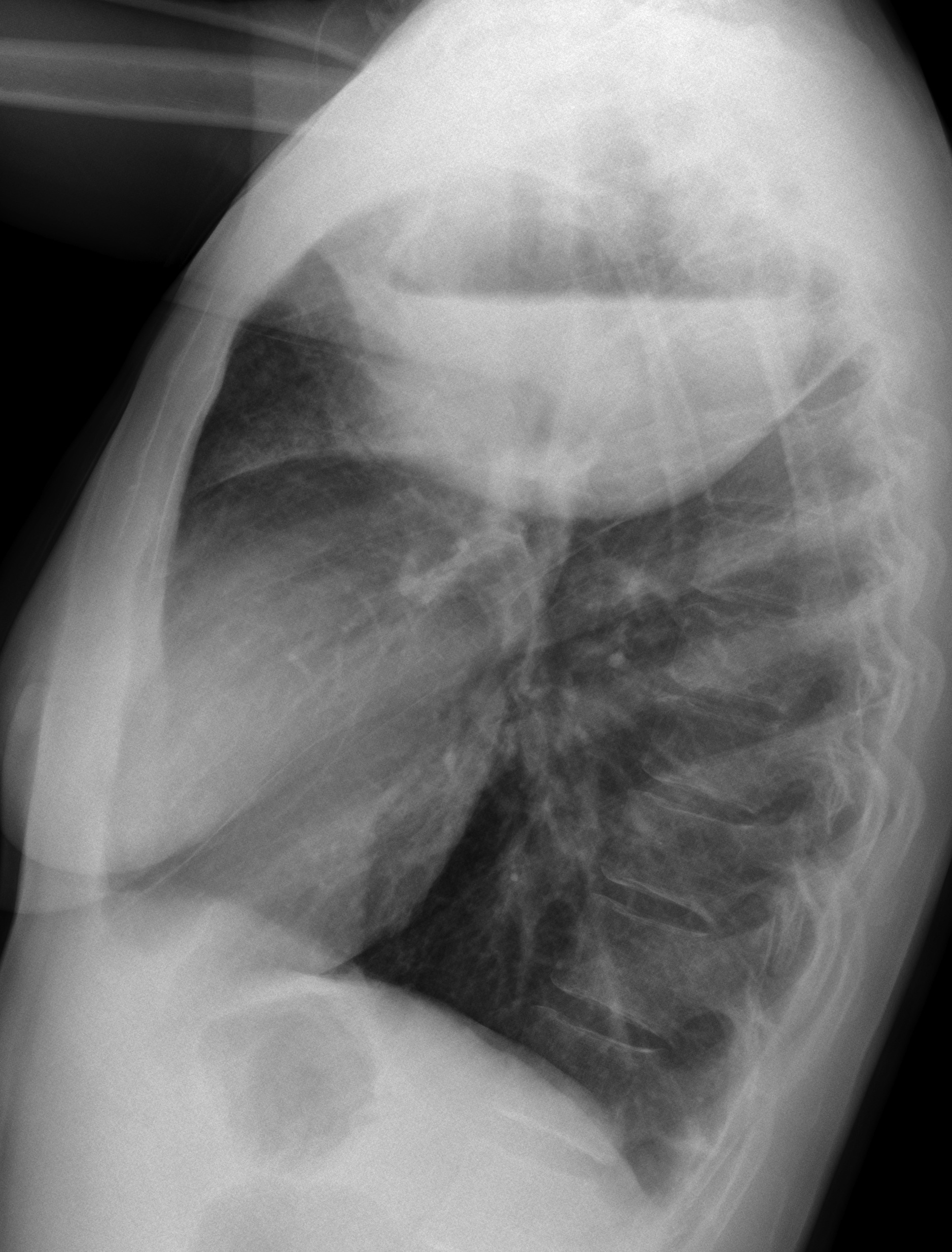
42-year-old woman, lateral chest
Click here for the answer to case #52
Findings: chest radiographs show an RUL lesion with an air-fluid level. The lesion is clearly intrapulmonary because it has an upper wall (arrows) and the air-fluid level is about the same size in both projections. The main finding is an irregular mass protruding from the lateral wall of the cavity (
red arrow). This finding strongly suggests a malignant process.
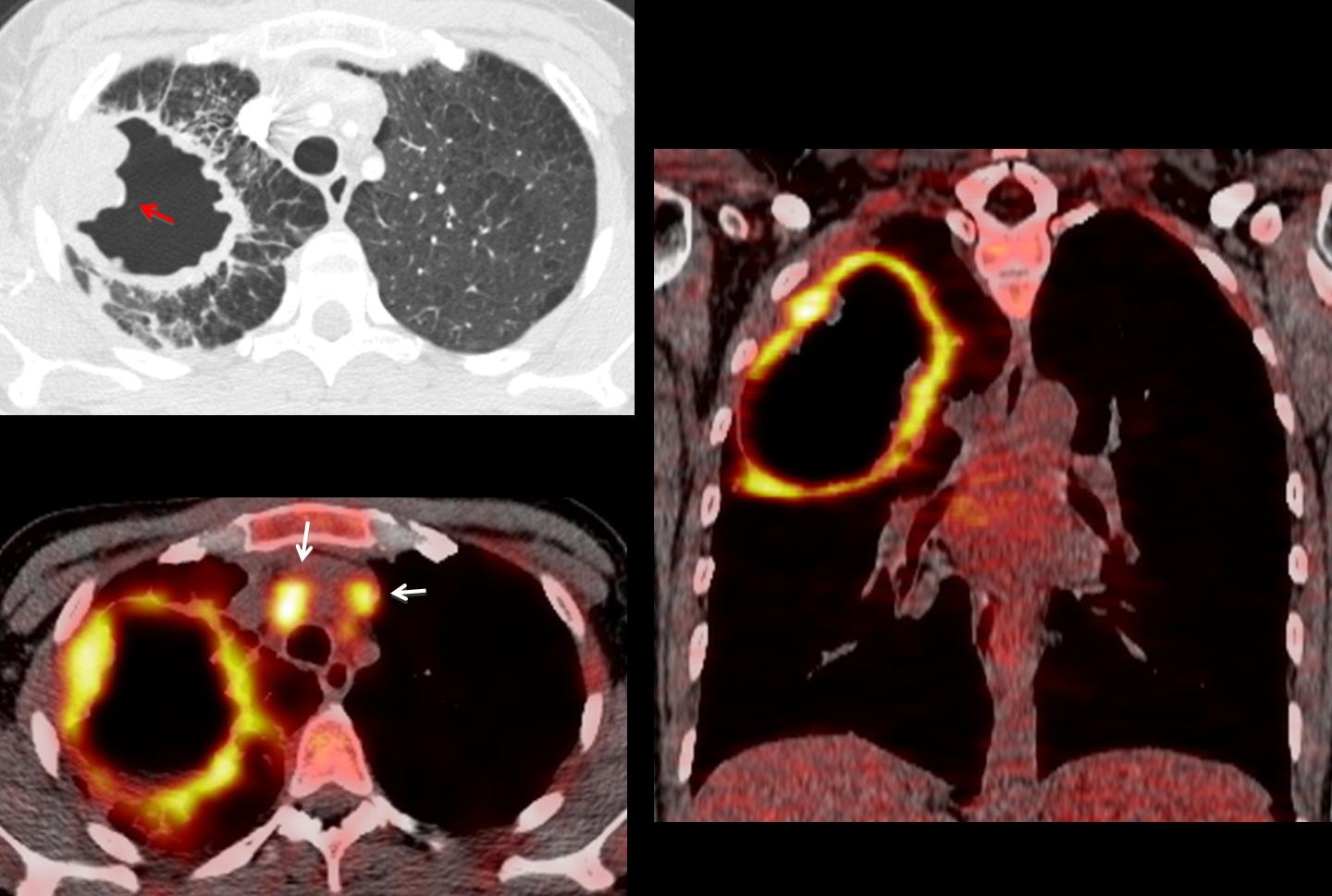
CT confirms the wall mass (red arrow). Additional criteria of malignancy are the numerous Kerley lines around the lesion. PET-CT images show enhancement of the wall and mediastinal lymph nodes (arrows).
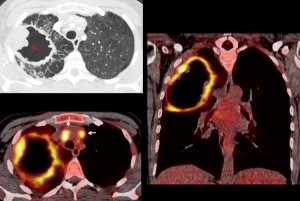
Final diagnosis: infected squamous-cell carcinoma.
Congratulations to Dr. Amutha, who was the first to suggest the right diagnosis.
Teaching point: cavitated inflammatory masses may have irregular walls, but a localised wall mass is highly suspicious of malignancy.


pulmonary absces
Probably a loculated pleural empyema due to the wall abnormalities and dislocation of the parenchyma seen on the lateral projection
pulmonary ab
I think about a loculated empyema; I see the pleural sheets around it.
lobulated empyema
There is a cyst with a thick wall and a fluid level.
The Rx findings with the high fever are elements for pulmonary abscess.
pulmonary abscess
pulmonary abscess
loculated empyema
Loculated Empyema
1
Laconic. I like that.
Empyema
Pulmonary abscess
Loculated empyema
Pulmonary abscess
Carcinoma of the lung, cause asymmetric thicking wall.
Dear Minnie I am sure you will perform very well in this rat´s race.
Polmonite necrotizzante.
Lesioni intrapolomonare con parete spessa, irregolare e bernoccoluta , superiormente. Non visibili adenopatie ilari. Un poò stirato verso l’alto l’ilo dx e la piccola scissura interlobare.Polomonite necrotizzante. Illustre professore ma non erano finiti con il caso 49, i livelli idro-aerei?
Sorry, Muppet made me do it!
Seeing the answers, I believe the air-fluid chapter is not over yet…
Teaching is hard…
Yes, it is. But very satisfactory.
Pulmonary abscess
Welcome! Muppet delighted to have somebody from Argentina (other than Messi)
I think it Is a pulmonary lesion, either simply an abscess or (more likely as mentioned by Minnie above) a carcinoma due to the nodular upper lateral wall.
Different sizes of the lesion in PA and lateral views, but it seems a pulmonary one. The wall is rough where we can see.
It must be a superinfected carcinoma.
Correct answer 1.
Loculated empyema
3. Loculated empyema
Hydropneumothorax can be a good option. The upper liquid level has a horizontal (in empyema usually concave), extending from side to side of the thoracic cavity as both lateral projection PA.
What nonsense are said not to look carefully at the picture.
I take it back
I think it is an abscess in a lung cancer and a air-liquid level. It has an irregular thicked wall in the upper side.
Pulmonary abscess.
Do you want to try again?
In addition to the asymmetric wall thickening pointed out by Minnie M, two more signs:
– there is some volume loss of the RUL.
– the minor fissure makes a Golden S sign (lateral view).
Io penso , alla luce delle osservazione di alcuni miei colleghi e dello slittamento verso l’alto della piccola scissura interlolobare e dell’ilo che un cancro-ascesso non può essere escluso. Tuttavia la giovane età della paziente mi ha fatto propendere x una polomonite necrotizzante.Risulta evidente che la non responsività al trattamento antibiotico nei radiogrammi successivi, deve propendere x un cancro-ascesso.
we are dealing with cavitary lung lesion in the posterior segment of the Rt upper lobe with irregular thick wall and irregular inner margin, no hilar or mediatinal lymph nodes enlargement. so,it is less likely to be carcinoma, with clinical history, and location, most likely post primary TB.
Chest radiographs revealed a well defined right UL cavitary lesion. , thick walled , irregular inner margin , with air fluid level that is nearly of equal diameters in both views . Also homogenous opacity is seen Laterala to the cavity in frontal view , the right transverse fissure is bulging downwards, the there is no hilar lymph adenopathy .
No pleural effusion seen.
Normal rest of both lungs .
differential diagnoss .
Lung abscess on top of necrotising pneumonia in view of fever .
Lung carcinoma, the Golden “S” sign is visible not only in the lateral view, but also in PA, and the thicknesss of the wall, I think it’s an infected lung carcinoma
More interesting signs:
– posterior wall of intermediate bronchus is thickened.
– there is an opacity at inferior hilar window (doughnut sign) (lateral view)
Hi. I’m a medical student. I had an exam last week and there was one question with a chest x-ray image showing a cavity with an air-fluid level. I had no doubt that it was “lung abscess” but I was wrong. Here I see your post, and now I understand it could be also lung cancer. It was very informative. Thank you.