Showing images of a 30-year-old male, asymptomatic. What would be your diagnosis?
1. Pericardial cyst
2. Lung tumour
3. TB lymph nodes
4. None of the above
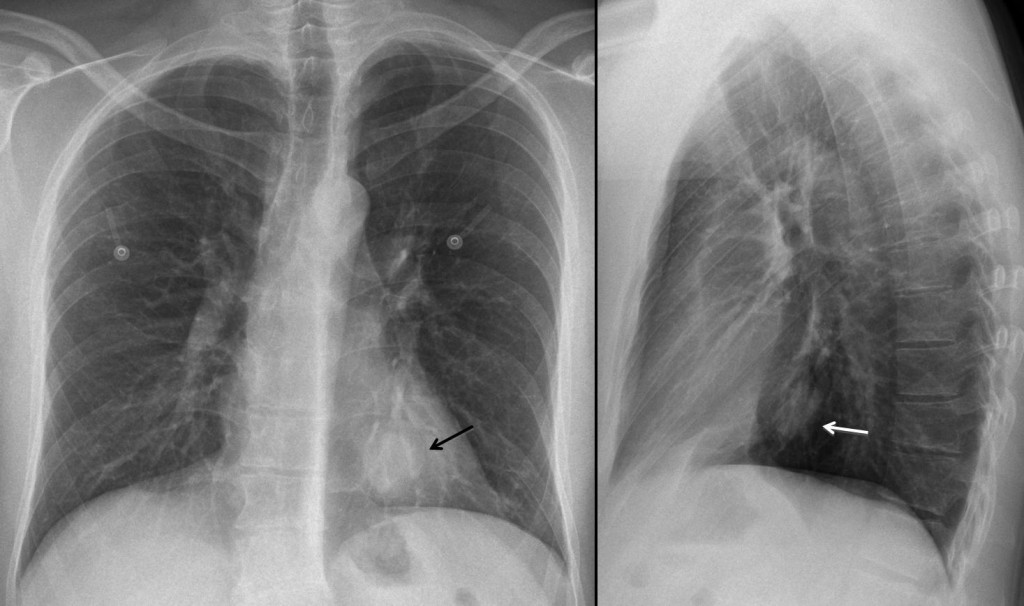
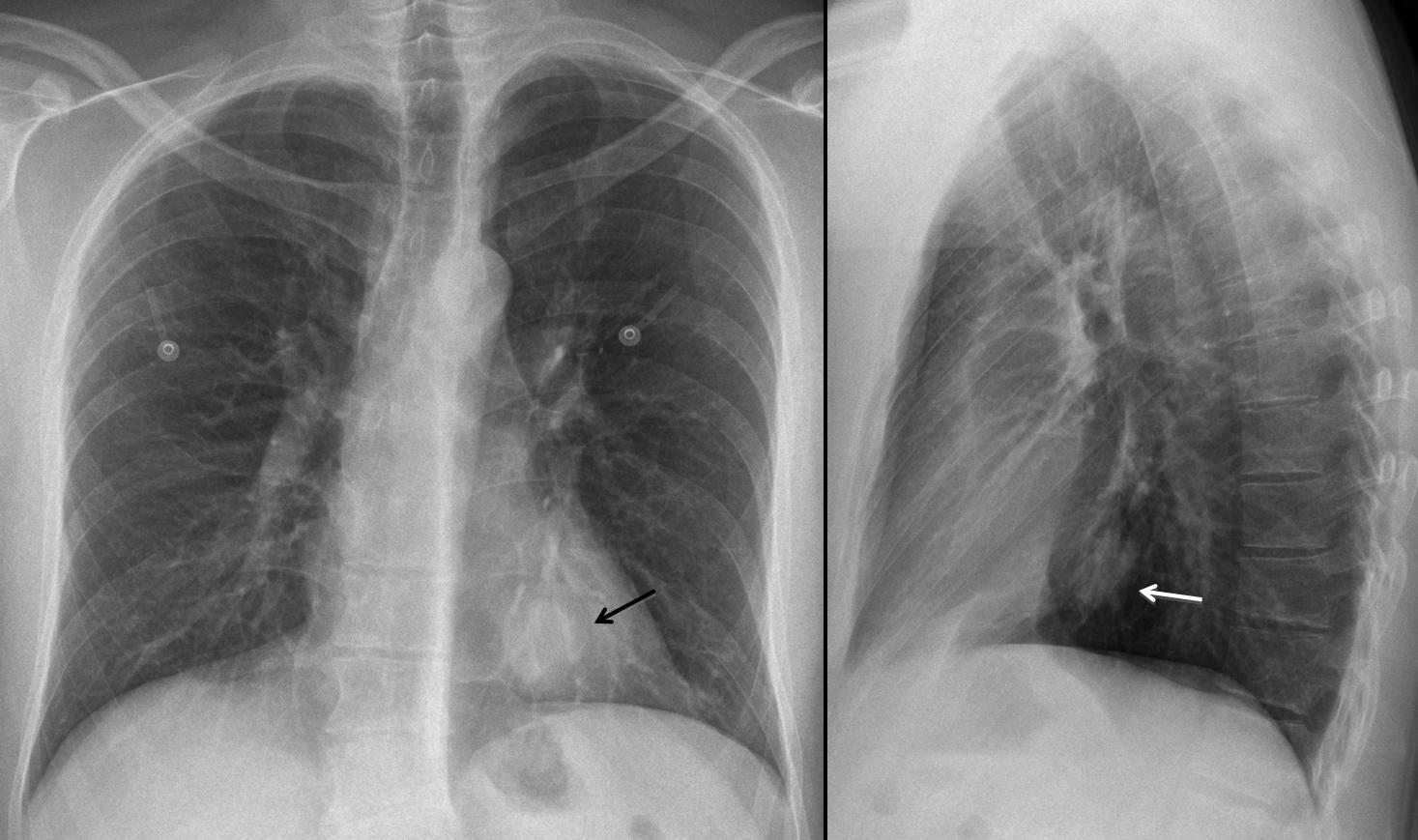
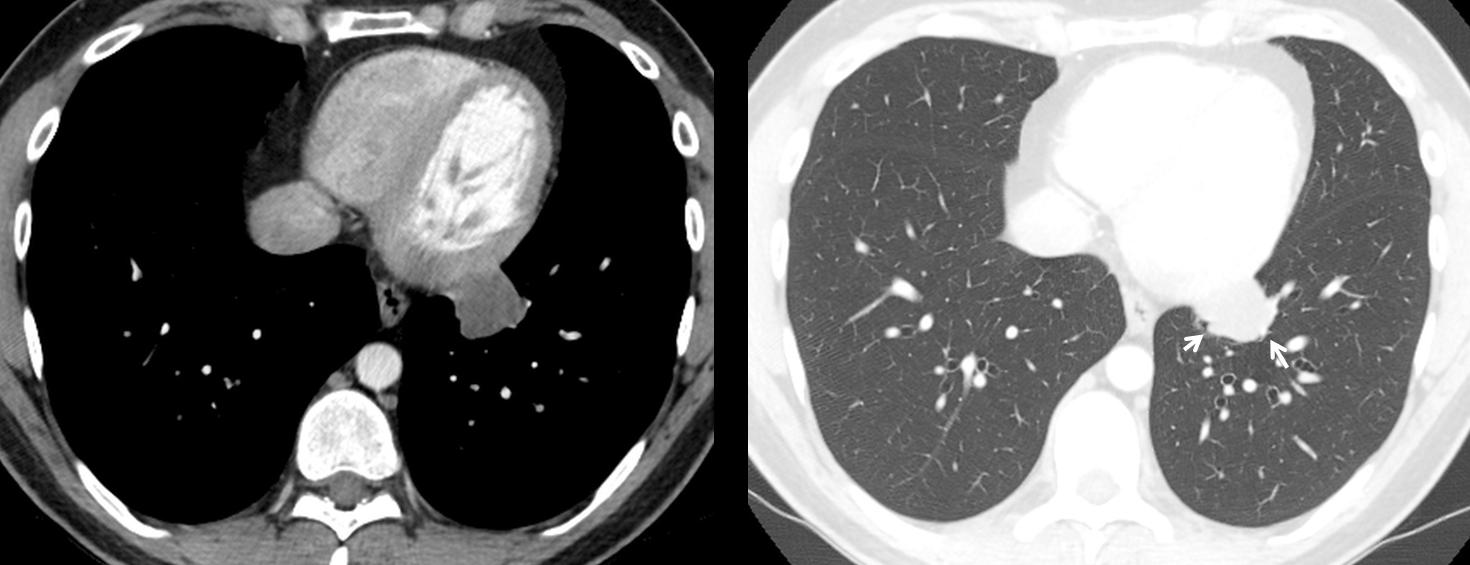
Findings: PA and lateral chest show a rounded lesion behind the cardiac silhouette (arrows).
CT shows a slightly irregular hypodense mass, which does not enhance with IV contrast.
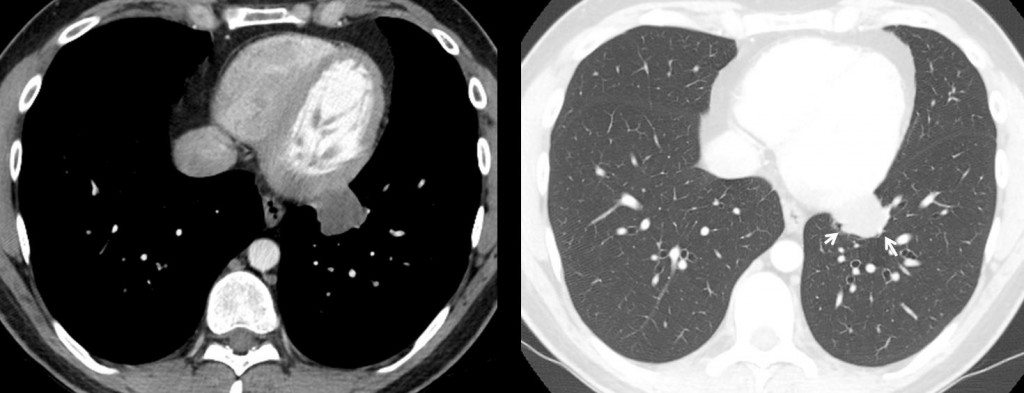
In the pulmonary window the mass is poorly defined, with irregular borders (arrows). This combination of signs speaks against a mediastinal mass and makes the lesion intrapulmonary, excluding pericardial cyst and mediastinal lymph nodes.
Final diagnosis: mucinous adenocarcinoma of the lung (explaining the hypodensity of the mass).
Congratulations to Dr. Prasanna Kulkarni who made an accurate description of the findings and arrived at the correct conclusion.
Teaching point: recognising the signs that differentiate intra from extrapulmonary lesions will lead you to the right diagnosis, as Dr. P. K. did.






Pericardial cyst
Nothing of the above!
Could you be more specific?
In the PA-Chest there is a retrocardiac nodular image, with well defined borders, which leads me to think it’s an extrapulmonary lesion.
At the CT, the nodular lesion has a soft tissue density, with well defined borders, and doesn’t appear to be disrupting the surrounding lung parenchyma.
With all this, I’m inclined to think this is a mediastinal lesion, in contact with the heart, an so a Pericardial Cyst would be my choice.
I disagree with your comment about the mass having well defined borders
CR shows a round well-defined mass in the left side, over the heart. In CT there is a extrapulmonary mass in contact with the heart, with soft tissue atenuation, although in enhanced CT pericardium shows an atenuation higher than mass does. I think it is a percardial cyst
I think it is a vascular lesion ?? aneurysm of the ?? coronary artery
Considering that IV contrast has been injected, I would expect a vascular lesion to enhance.
vascular lesion
pericardial cyst
An important point in the evaluation of this lesion is the absence of pericardial effusion.
It could be a fibroma?
I cant see the x ray images. I think we are in front of a pericardial lesion. It doesnt look like a simple cyst, so I would exclude the pericardial cyst. The most frequent pericardial solid lesion would be metastasic disease, the age of the patient goes against this diagnosis. The same happens with the lack of pericardial effusion, does not favour the malignant ethiology. With this I would think of a benign mesenchymal primary pericardial tumor (hemangioma, lymphangioma, lipoma, neural tumor, leiomioma). No fat density and no significant enhancement goes against lipoma and hemangioma respectively. I would hope a slightly dense and homogeneous soft tissue mass for a leiomioma. It has no calcium and the enhancement if exists seems to be minimum.
I have never seen one, but my orientation would be a PERICARDIAL LYMPHANGIOMA.
Anyway, comparision with prior Xray and further strict follow up is necesseary.
Soft tissue mass in left lower lobe adjacent to or invading the pericardium, possibly of mediastinal origin.
It is somewhat ill-defined, while the surrounding lung parenchyma seems normal.
The mass is rather homogeneous without calcifications or cystic
Even though the lung looks normal and there are arguments for mediastinal origin it could very well be an early stage lung tumour. I am not convinced we can reliably differentiate between the above mentioned options with imaging alone.
Biopsy or surgery is mandatory (unless there are older images to prove it is a stable lesion).
Vi sono due tubicini (?) rxopachi a livello della sesta costa, bilateralmente.Vi è una immagine ipodensa, che non prende CE ed appare indissolubile dalla parete cardiaca. Se il soggetto ha subito un intervento chirurgico, questo puo’ essere la risposta infiammatoria localizzata,come nela Sindrome post-pericardiotomia.La risposta alla terapia cortisonica ne è la controprova.
My answer is D.
On the frontal view, there is evidence of a well circumscribed ovoid mass projecting over the retrocardiac region in the left lower zone. on lateral view, the mass appears to be in the region of middle mediastinum.
On CT scan, the mass appears to be intrapulmonary. bronchioles and pumonary vessels are seen at the periphery of the mass. the contact between the mass and the pericardium is ill defined, without any visible fat planes.the internal attenuation of the mass is slightly less than of the interventricular septum, indicating enhancement. no evidence of calcification or macroscopic fat.
Correlating with the age and absence of symptoms, my differentials would include peripheral carcinoid, intrapulmonary sequesteration and round atelectasis.
Good! At last someone has seen the light!
I disagree with round atlectasis as there is no volume loss, also no associated pleural disease.
I like your diagnosis of peripheral carcinoid (there is a distorted bronchus at the periphery of the mass). A dense bronchogenic cyst is less likely. Definitely it is NOT an extrapulmonary mass.
CCAM , Tipo 3 sec. Stolker.La malformazione cistica adenomatoide, di tipo III sec. Stolker si può presentare come una massa solida, ipodensa alla TC.Essa inoltre ha sede frequentemente paramediastinica. PS. il Bari malissimo in campionato: stiamo retrocedendo in serie C ! Ho recuperato “qualche punto” per la salvezza? Ma quei tubicini rx-opachi a cosa corrispondono?
I don’t know what the tubicini represents. It may be lepidic growth of the carcinoma; but I cannot be sure.