Today, we’re showing you radiographs of a 29-year-old non-European male with moderate dysphagia. Questions:
1. Where is the lesion?
2. What would be your diagnosis?
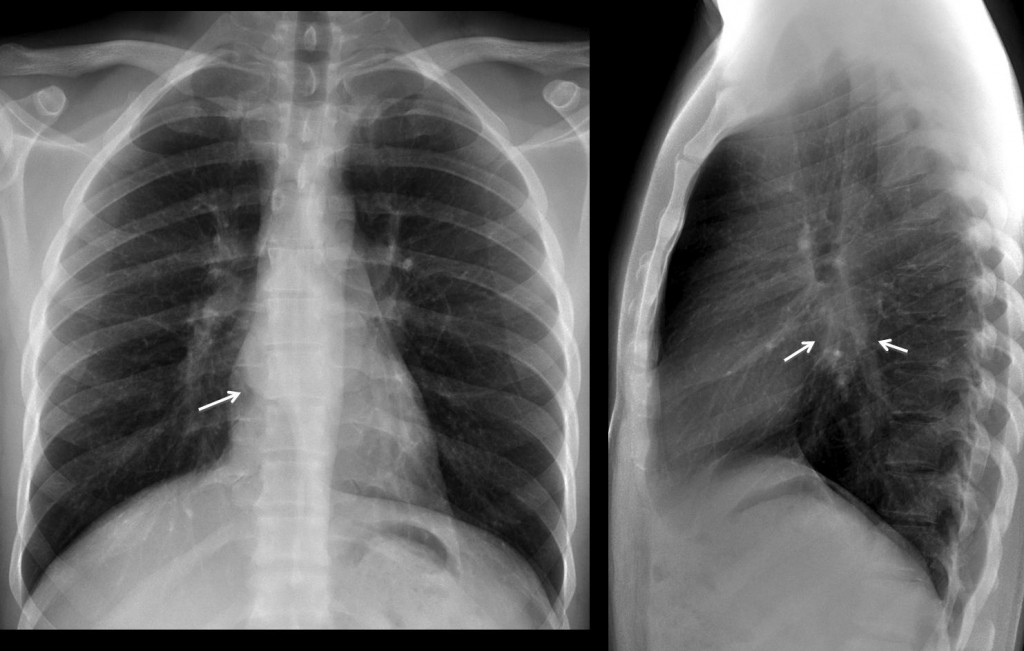
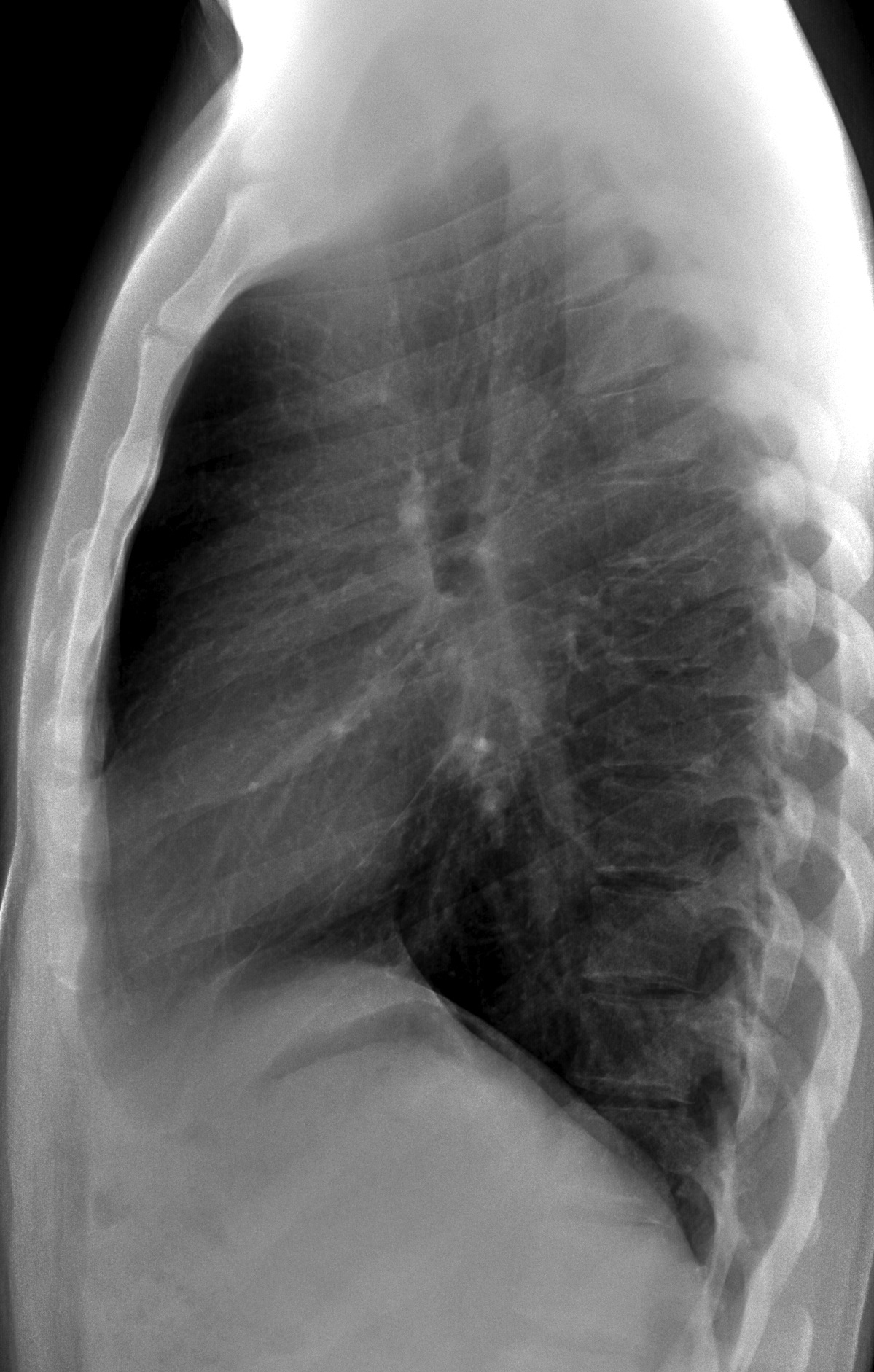
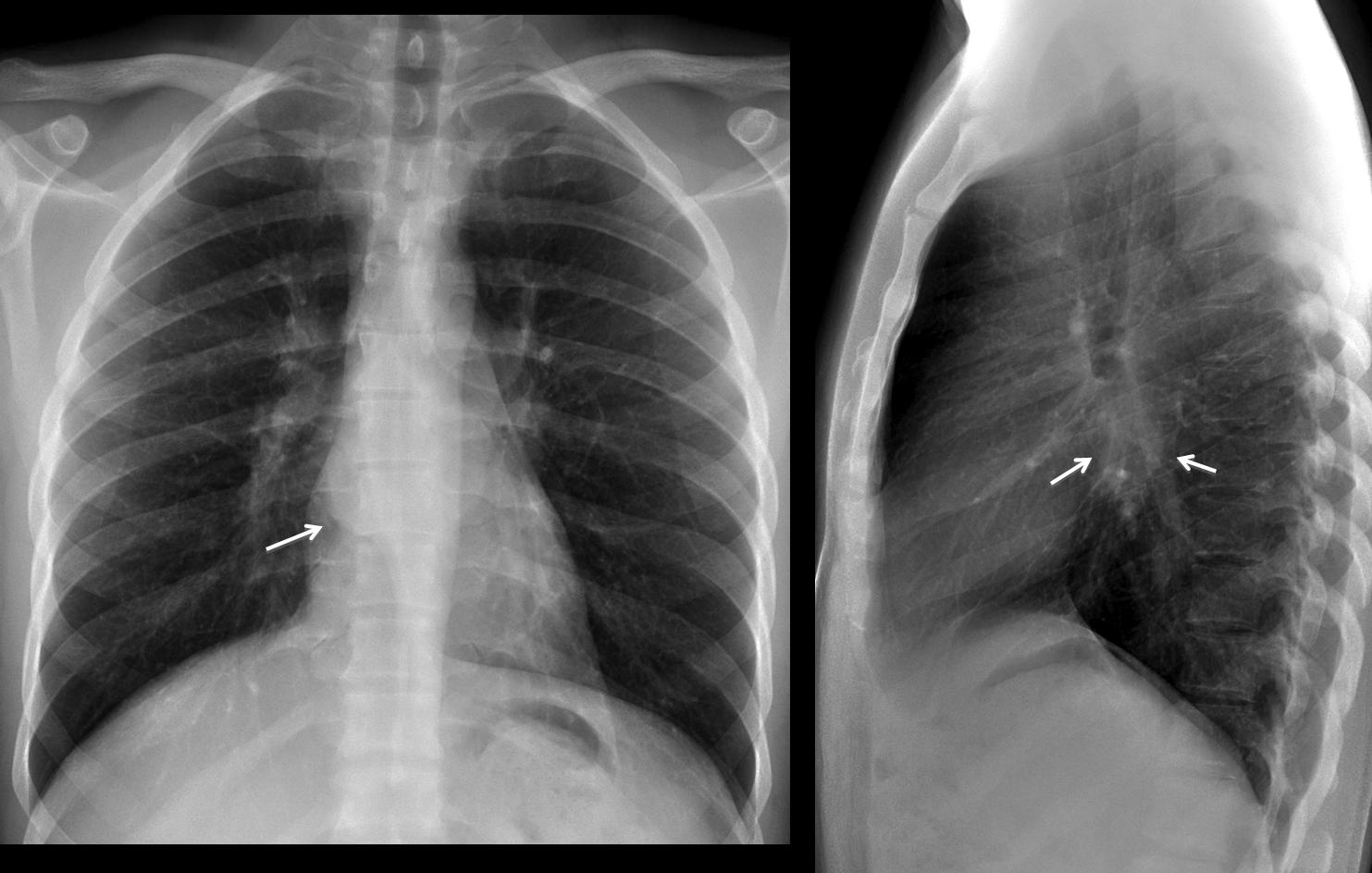
Findings: chest radiographs show bulging of the azygo-oesophageal line in the PA view (arrow) and occupation of the subcarinal space in the lateral view (arrows).
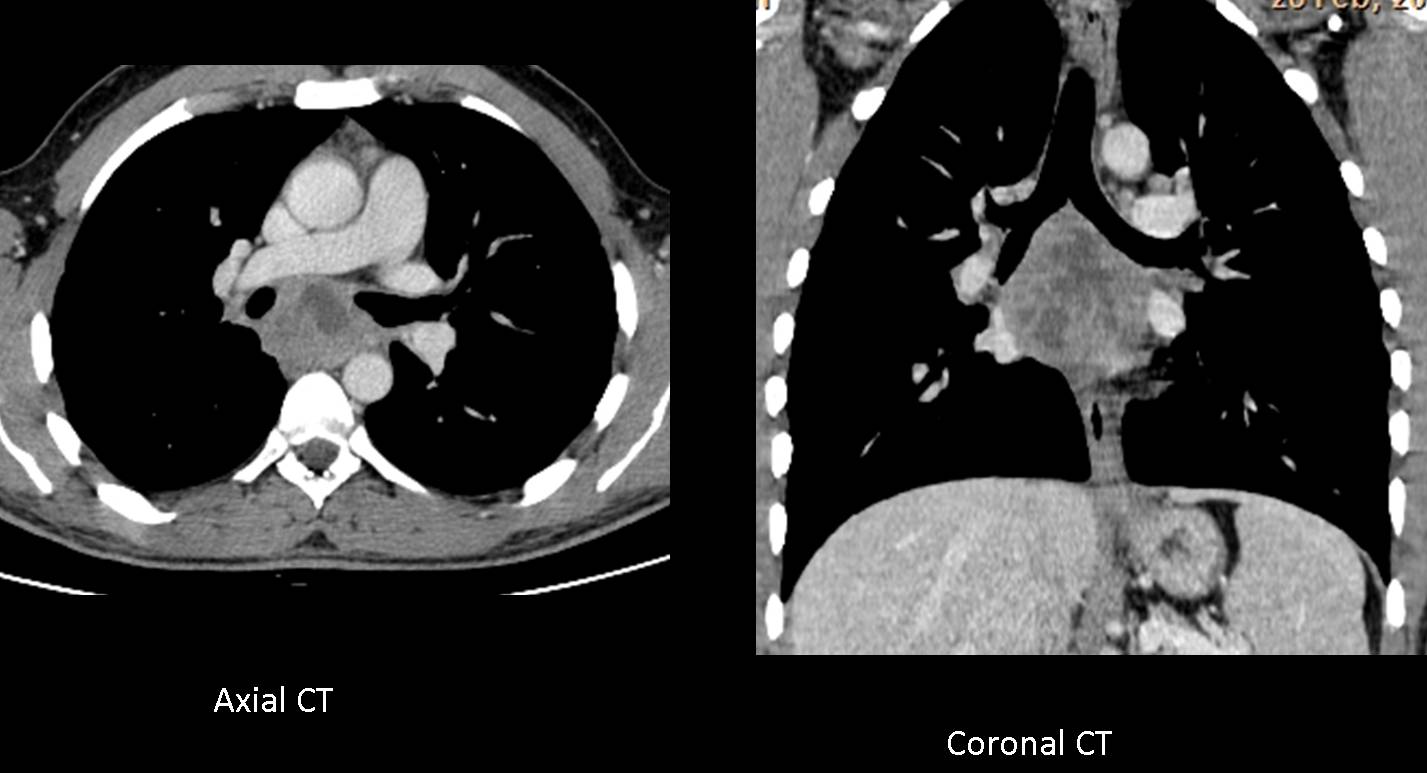
These findings point to a mediastinal process in the middle portion of the middle mediastinum. The most common pathologies in this location are duplication cysts or those related to enlarged lymph nodes. Axial and coronal enhanced CT show an irregular necrotic mass in the subcarinal area, compatible with necrotic lymph nodes.
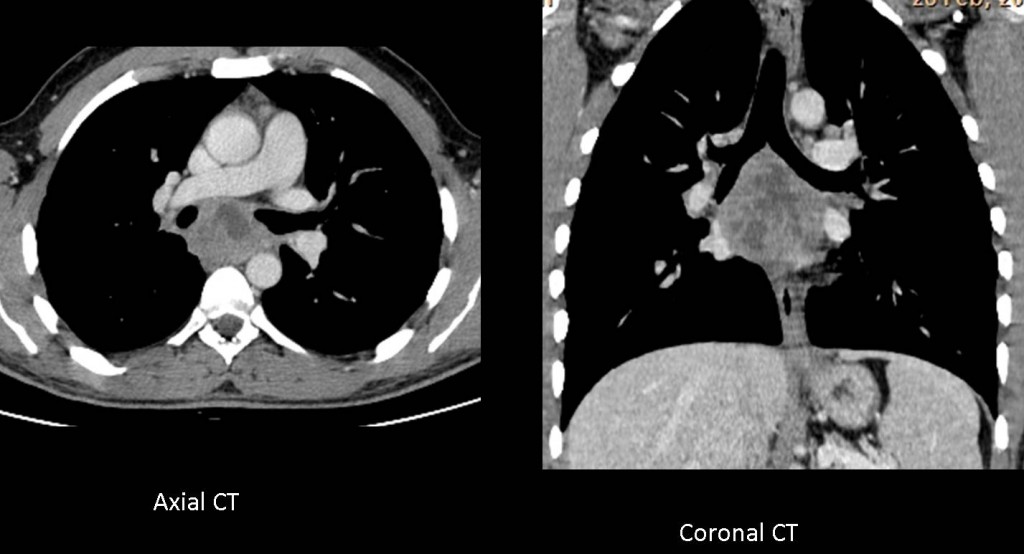
Considering that the patient is non-European, tuberculosis is a strong possibility. PPD was negative, but BK was found in needle biopsy.
Final diagnosis: TB lymph nodes
Congratulations to all of you who made a correct reading of the films and suggested the diagnosis, headed by Dr. Ashraf Abohadeed. Keep up the good work!
Teaching point: Management of mediastinal masses entails three steps. The first two are discovery and placement, both of which are made in the chest radiograph. The third step is characterisation of the mass, which is done with enhanced CT. These three steps allow the correct diagnosis of the majority of mediastinal masses.



Medium mediastinum mass. No lymph node enlargement or other finding pointing at traction diverticulum.
The dysphagia suggests primary a esophageal disease. May be a GIST ?
chest x ray frontal and lateral views.
A large well defined lobulated mass is seen subcarinal in location and extend into azygoesophageal recess with normal carinal angle .
normal lungs and cardiac shadow.
no pleural effusion.
normal underlying ribs and vertebrae .
conclusion
subcarinal mass extending into azygoesophageal recess .
DD: enlarged lymphnode either inflmmatory or neoplastic .
bronchogenic cyst .
esophageal mass , for ct scan with oral and IV contrast
there is a subcarinal mass.there is not normal carinal angle.
the mass desplace esophagus in lateral view and produse depression and dilatation of esophagus.i think that is external pressure.
bronchogenic cyst this time
middle mediastinum lesion with discrete borders . If not a congenital mass, i would think of infectious disease( non european male).
Thymom
Leomyoma of the esophagus , aberent lt pulmonary artey is another possibility
Location: Medium Mediastinal space
Diagnostic: Broncogenic vs pericardial cist
Opacità ovoidale nel mediastino medio, al di sotto della carena tracheale che non sembra improntata.Nessuno ha pensato alla M. di Castleman nella DD ? Io lancio questa opzione.
bronchogenic cyst
1/ Middle mediastinum.
2/Foregut duplication cyst (esofaphageal, bronchogenic) or lymphadenopathy.
there is an oval slightly lobulated mass in the lower middle mediastinum with close contact to the posterior mediastinum.
no other abnormalties.
1 duplication cyst
2 lymphadenopathy (anamnesis could be misleading though)
3 oesphageal mass (protruding in the middle med. from posterior) – diverticulum?
contrast could be given during repetition of the lateral view to gain more information of the position of the oesophagus, although ct is necessary.
Correct discussion. Just a little correction: the mass is in the middle part of the middle mediastinum. Masses in the lower part are lower(of course!) and have a different origin.
Thanks for pointing this out!
Good. Many of you are following the correct approach to mediastinal masses: first, place it in the correct compartment and second, mention the most common etiologies in this location. The following step is an enhanced CT, which will be shown next Tuesday.
Have a nice vacation!
1. middle mediastinum subcarinal
2. bronchogenic cyst
Pretracheal mass could be lymphadenopathy with minimal cp angle blunting
anteriorly side?.