Today we’re presenting a routine chest control of a 53-year-old woman who had a lumpectomy for carcinoma of the breast three years ago. Radiographs were read as normal. Do you agree? Any ideas?
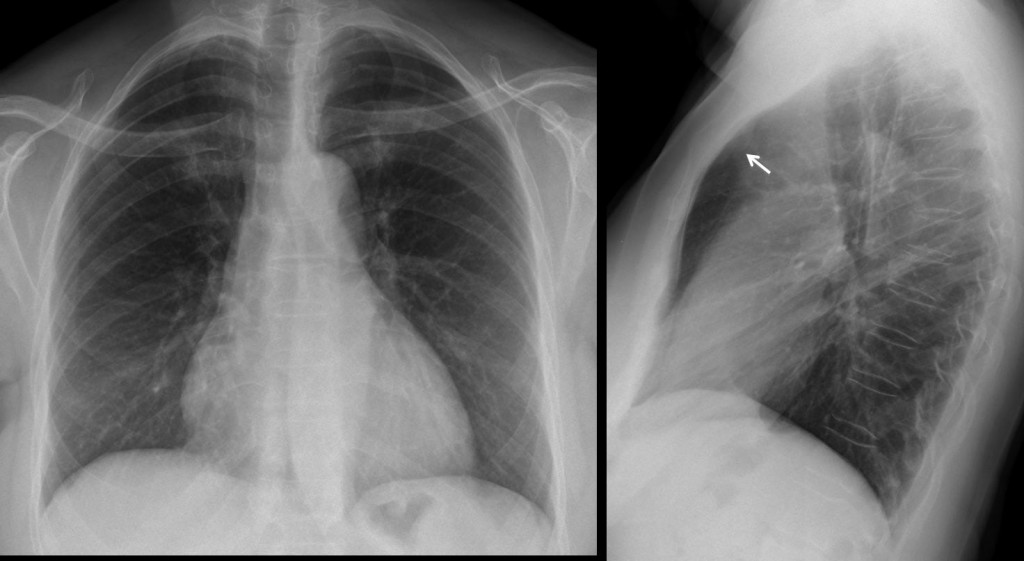
Fig. 1
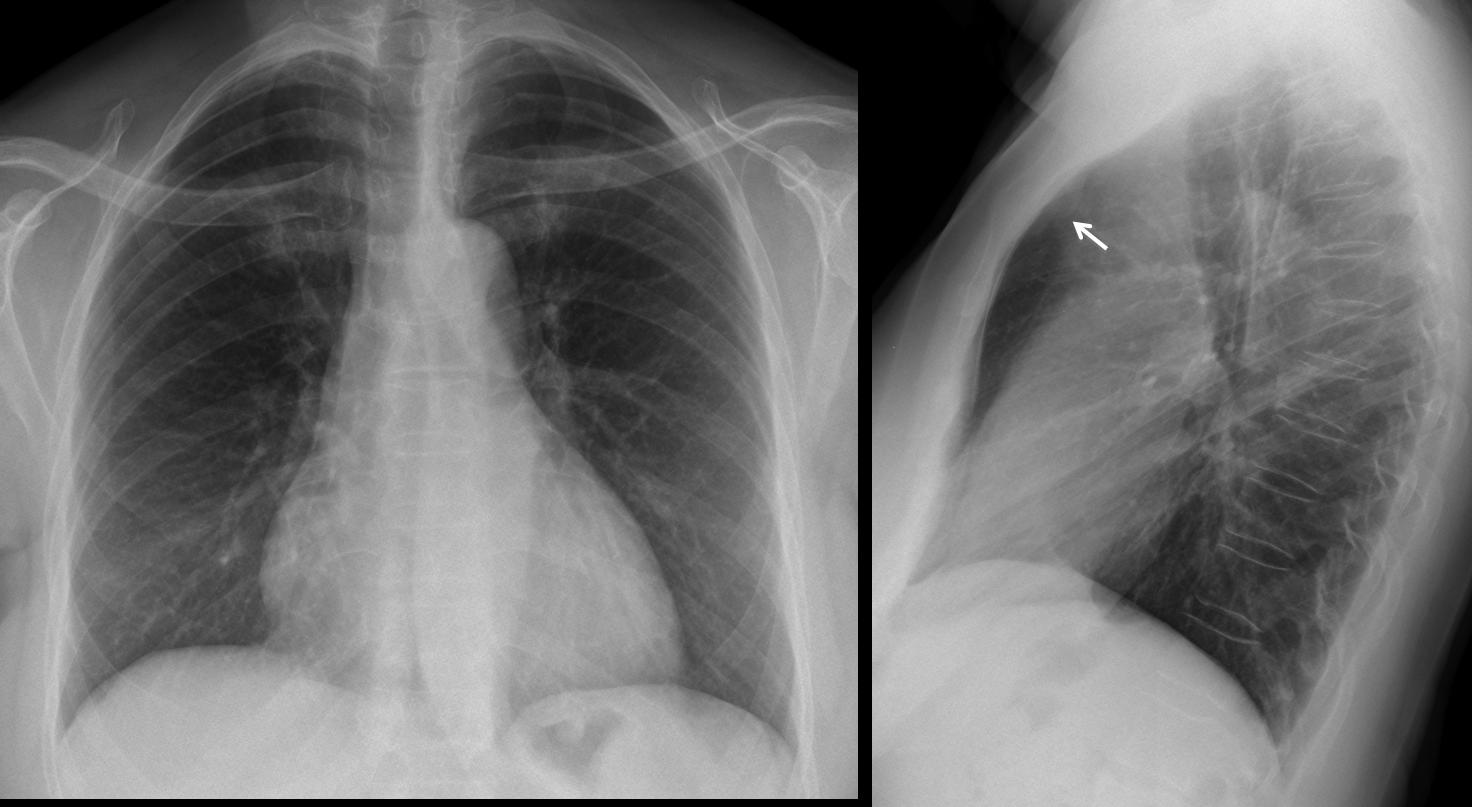
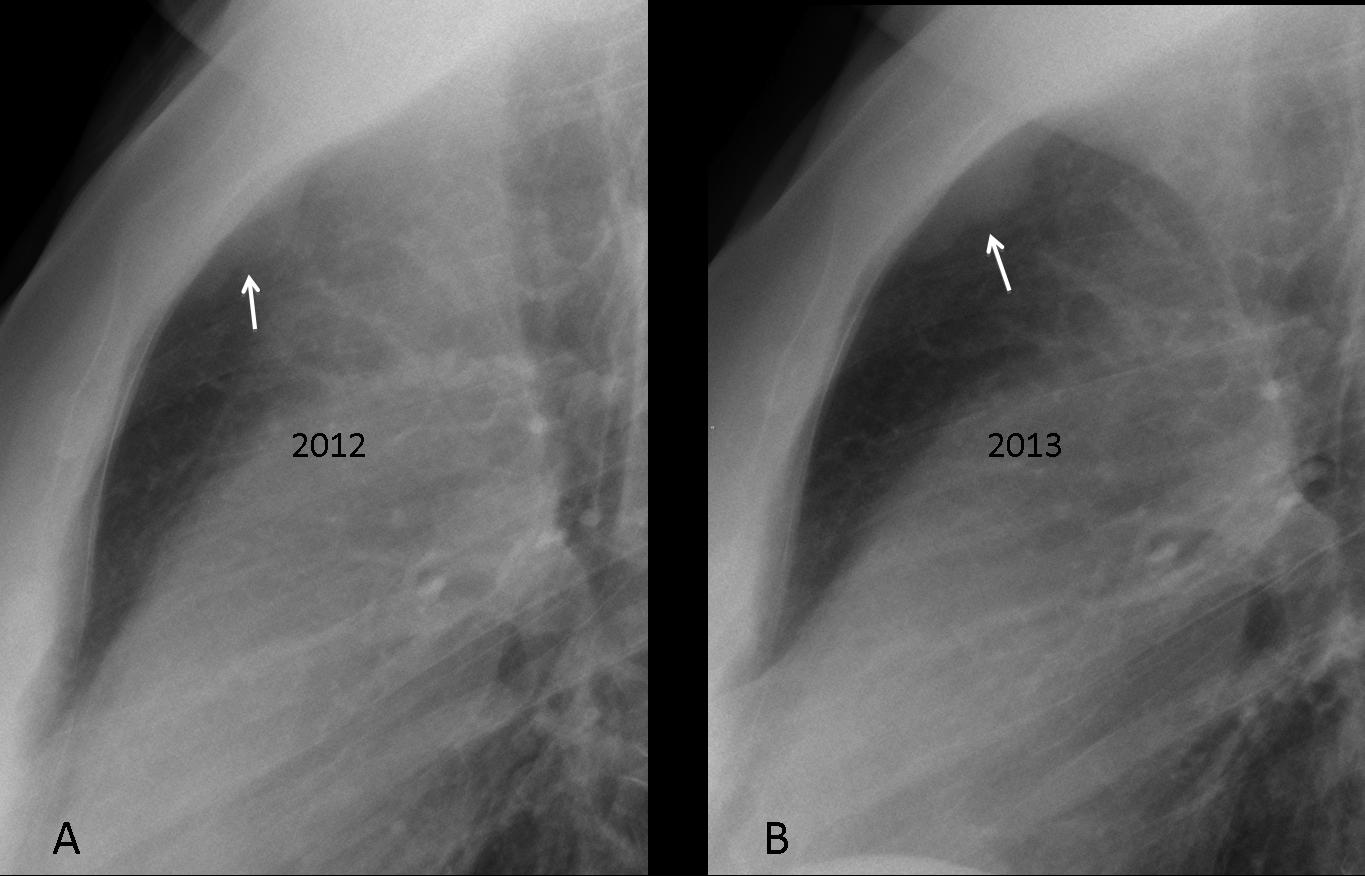
Findings: the lateral chest radiograph shows a lobulated, well-defined retro-sternal opacity (arrow), better seen in the cone down view (fig. 2a, arrow). The opacity has increased in size one year later (fig. 2b, arrow).
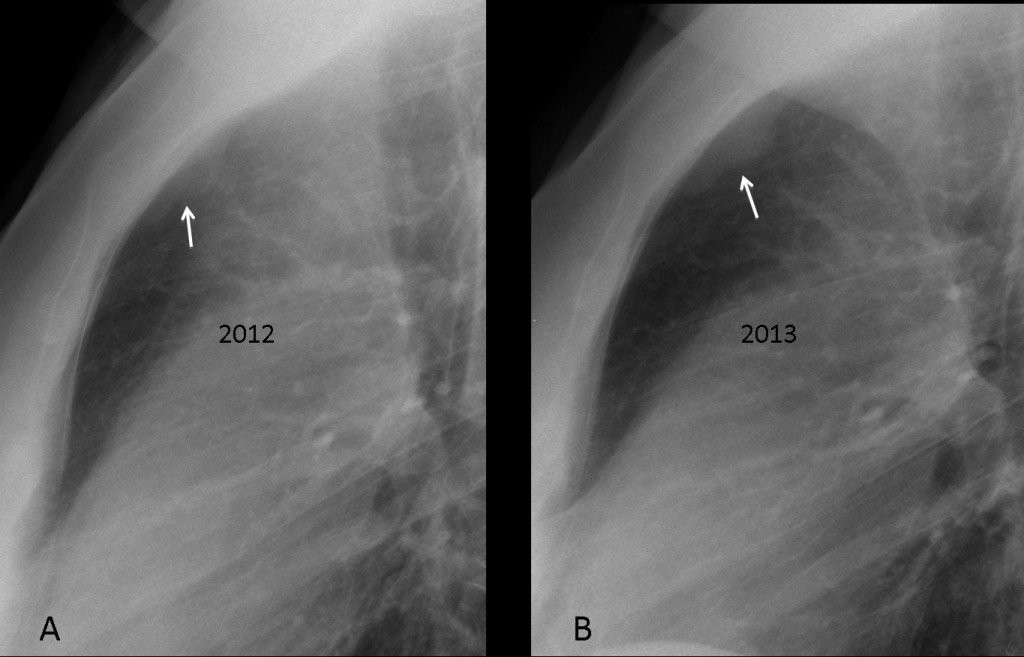
Fig. 2
Sagittal and axial CT confirms the presence of the mass (arrows).
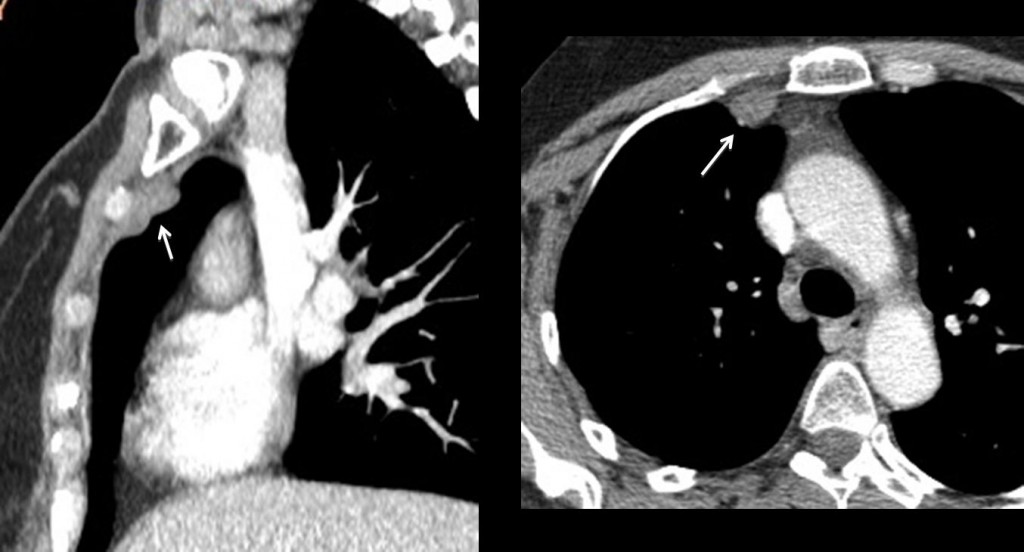
Fig. 3
Final diagnosis: metastases to internal mammary nodes. No other metastases were seen.
I am presenting this case to emphasise the importance of looking in the lateral view at the blind areas in the PA chest radiograph. The metastases were overlooked in the initial exam and were found one year later by somebody more thorough. Congratulations to Katerina, as the sole discoverer of the lesion.
Teaching point: always look at the anterior clear space in the lateral view. Significant findings may be discovered, as in this case.
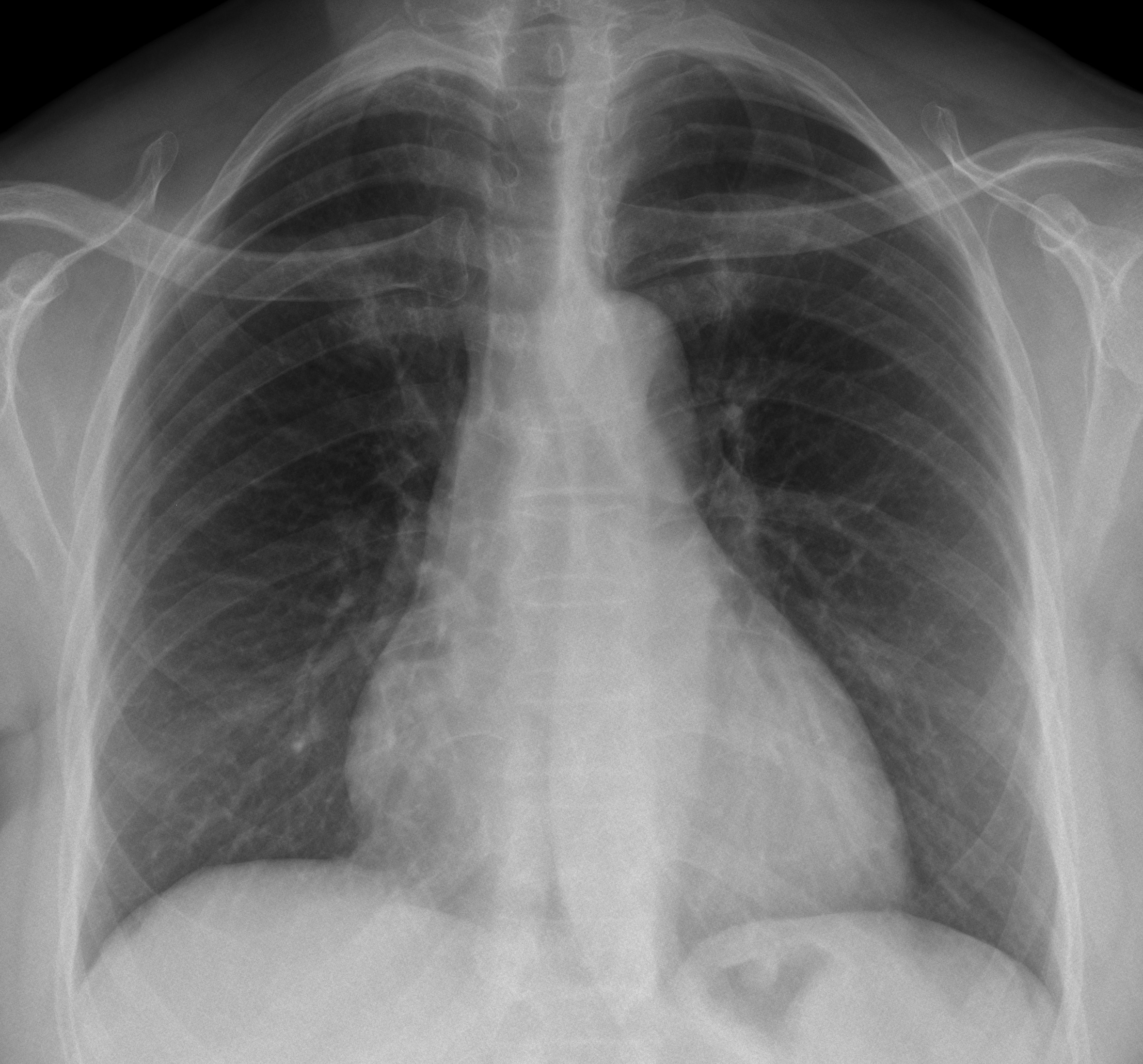




PA chest radiograph rotated.
Heart size at the upper limits of normal.
Not identified or consolidativas nodular lesions in the lung parenchyma.
Pleural space unchanged.
Doubtful 8th radiolucent lesion in left posterior rib.
Diffuse osteopenia of the spine.
linear periostitis along the inferior aspects of the lateral portions of the right 4, 5, 6 th ribs – probably post radiotherapy.
mild cardiomegaly and osteopenia.
Congratulations to the two earlier participants. You are very brave! I can feel the others waiting in the shadows for a hint!
Anyhow, you did not mention the abnormality. Good try!
Chest x ray frontal atl view
Status follow up after right breast lumpectomy 3 yeas ago .
Finding
Normal lungs , pleural angels , cardio mediastinal shadow.
No visible rib or vertebral lytic or sclerotic lesions.
A well defined filing defect i s seen though gastric air bubble , could be breast metastatic lesion , or gastric primary tumor , so CT scan is advised .
sternum is ok?
lateral spondylolisthesis T6-T7?
In the PA chest radiograph:
– radiolucent lesion without sclerotic borders on the left first rib (lytic meta?)
– a possible pulmonary nodule projecting at the intersection of the anterior portion of the 2nd rib with the posterior protion of the 5th rib on the right which is not seen on the lateral projection (D/d sclerotic rib lesion)
In the lateral chest radiograph:
– in the retrosternal space there is a radiopaque lesion with lobulated borders which has a broad contact with the pleura and obtuse angles with lung parenchyma (pleural lesion?)
What is the cor, What is distance FFD?
I don´t see well defined the anterior portion of 3rd left rib (osteolysis?)
Scusa il ritardo ma solo ora il mio PC riporta il caso.Una lettura superficiale può dare come normale il caso che presenta diffuse metastasi ossee, come confermerà la scintigrafia. Le lesioni interessano , 1°) corpo sternale, 2°)La scapola di sx,3°) l’arco anteriore della 2 , 3 costa di sx, nonchè la 7;,4°) lesione del corpo vertebrale della 3°,6° 7°; 5°), immagine nodulare sul fondo gastrico.
Meta in lower left lobe (10th segment).
I also think that the lesion is on the back side of the 8th rib (lithic) which can be a metastatic one…
Is that an eosaghageogragh.although its faint may be delayed to show adiverticulum due to traction from lymph node had metastasis
In the lateral chest radiograph – osteosclerotic metastases from breast cancer to the posterior part of the body and pedicle (Th10?)seen as a whole above the diaphragm
may i blame my small cell phone screen for not spotting the lesions mentioned by dr. genchi? however (assuming these are the abnormalties) this is a frightening case – not many people would find these lesions without prior knowledge of their existence i guess.
especially when reading 50+ cases in a short time. seems like a wake up call to pay more and special attention to the bones.
would you consider another bone case?
You are assuming that our colleague is right. Anyway, images are supposed to be seen in a monitor with a good definition. I would not recommend a phone screen.
In the lateral chest radiograph – osteosclerotic brest cancer metastasis to the posterior part of the body and pedicle(Th 10? – first seen as a whole above the diaphragm)
Me llama la atención un aumento de densiddad en los pedículos de las ultimas vertebras torácicas, metas blásticas?
So far, only one person has seen the abnormality. Remember the basic priciples: which areas should be examined in the PA and in the lateral radiographs?
I gess that person is Katerina: “in the retrosternal space there is a radiopaque lesion with lobulated borders which has a broad contact with the pleura and obtuse angles with lung parenchyma (pleural lesion?)”
An extrapulmonary lession in that location with that condition…internal mammary lymphadenopathy.
Good guess…but late.
I´m not in a hurry.
Congratulations Katerina.
nice case! as usual….