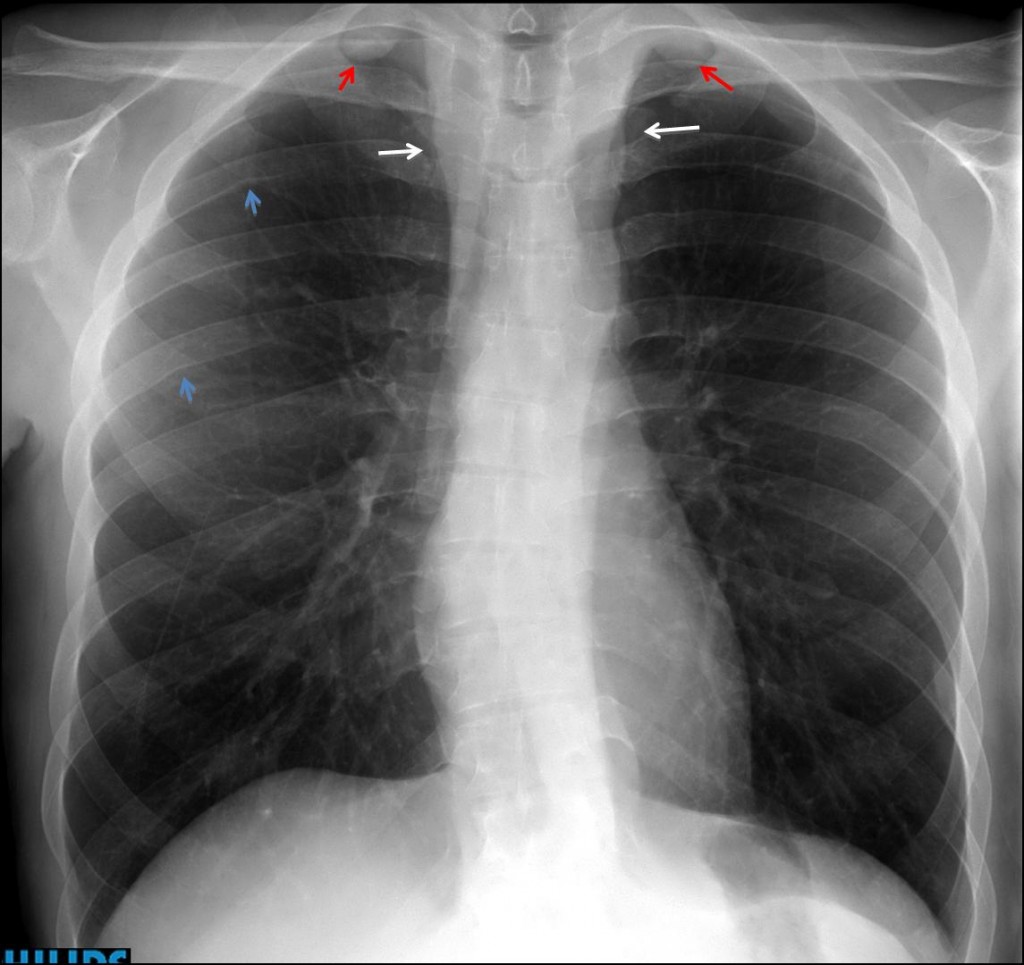
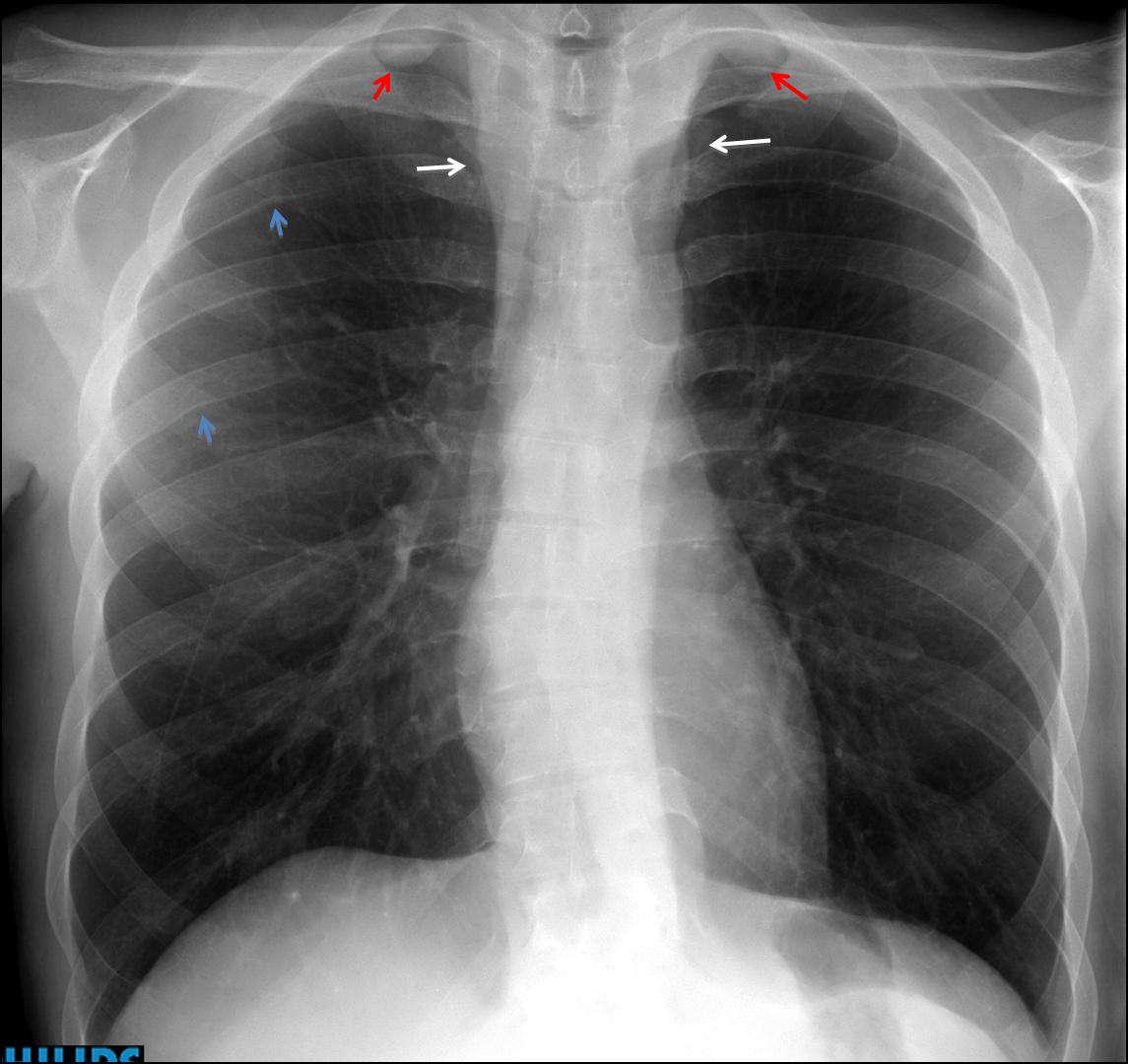
My former disciple Jordi Andreu has contributed this week’s case. Below is a pre-operative PA chest radiograph of a 27-year-old male with a growing perineal mass.
1. SVC obstruction
2. Coarctation of aorta
3. Lymphoma
4. None of the above
Findings: PA chest shows widening of the superior mediastinum (arrows) and two rounded opacities in both apices (
red arrows). Slight rib notching is visible (
blue arrows). The aortic knob looks normal.
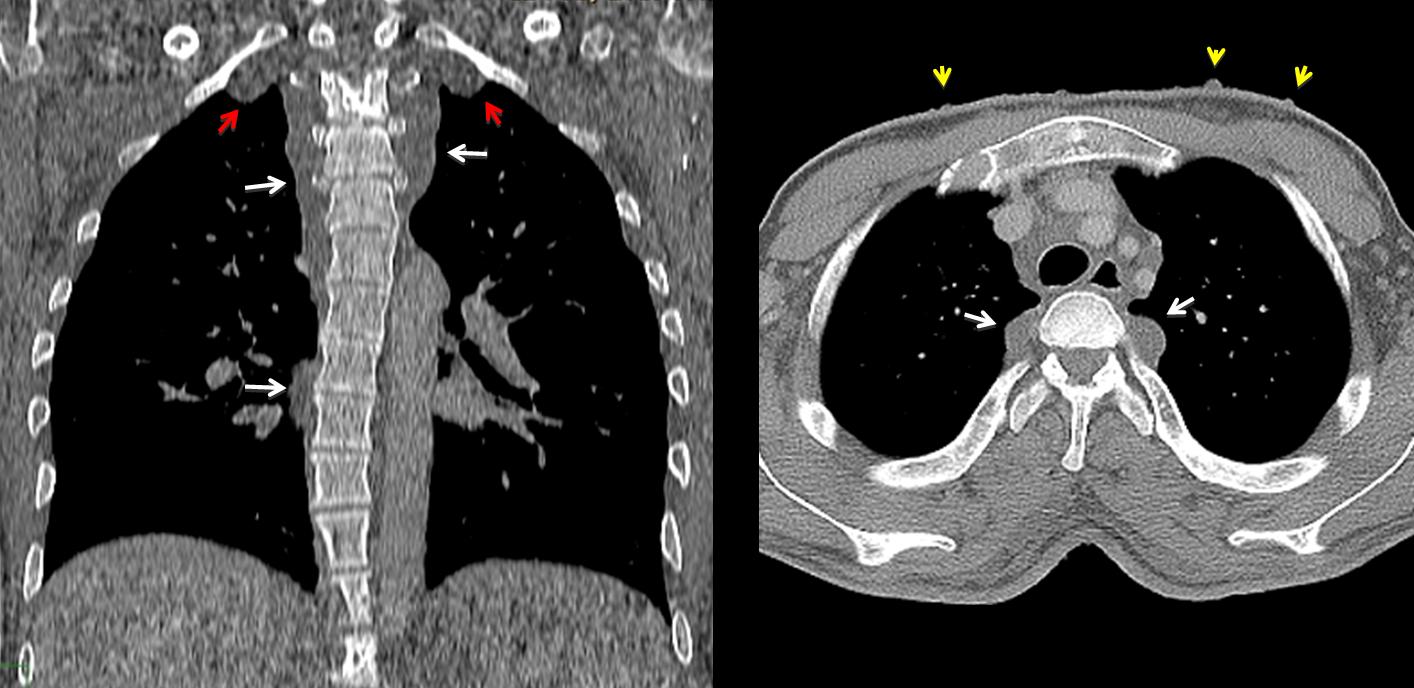
Coronal and axial CT shows soft tissue masses that extend along the posterior mediastinum (arrows) including the extrapleural apical areas (red arrows). The patient had known neurofibromatosis. Multiple skin lesions are visible in the axial CT (yellow arrows).
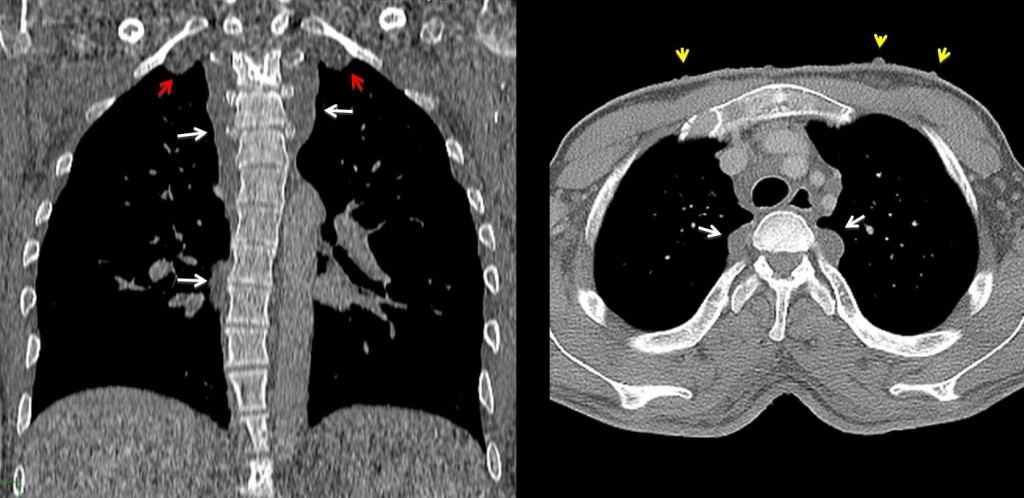
Final diagnosis: neurofibromatosis with sarcomatous degeneration of a perineal lesion.
Congratulations to Katerina, who gave an excellent discussion and made the correct diagnosis.
Teaching point: remember that aortic coarctation is not the only cause of rib notching. Be sure that the patient has hypertension before suggesting coarctation.


2. coarctation of aorta
coarctation of aorta with inferior rib notching and scoliosis
TOS( Thoracic Outlet Syndrome ) da costa cervicale accessoria, bilateralmente: Fascio vascolare del Collo ( ECD dei tronchi sovra-aortico, con prove dinamiche degli arti superiori per rilevamento polso radiale).
there is notching of the ribs under 3 rib bilateral und scoliosis.we dont see the aortic comb.
dilatation of pulmonary hilum but not in periphery.
we see both nipples und dilatation of superior mediastinum.
i thing coarctation of aorta
There is widening of the upper mediastinum bilaterally and increased density, probably due to vascular structures (lymphadenopathy is not that symmetrical).
Also there are dense structures projecting on the apices, of soft tissue density – therefore i am not convinced of accessory ribs… Also vessels? Enlarged collaterals?
In addition the rib notching… I choose coarctation.
Tricky case with only AP view ….
at first glance it seems like coarctation of the aorta
but …
– bilateral widening of the superior mediastinum continues above the level of the clavicles to join with
– symmetrical dense extrapulmonary lesions which project at the apices (not accessory ribs)
– widening of the left paraspinal line
– no tracheal deviation
so …
these findings can not be situated in the anterior or middle mediastinum.
They must be situated in the posterior mediastinum (neurogenic tumors? extramedullary haemopoiesis?)
so …
I choose 4.none of the above
Like Katerina, I think there is widening of superior mediastinum extending to both apices.
I also choose 4. The presence of another mass at the perineum suggest a diffuse disease like neurofibromatosis, plexiform neurofibromas?
Coarctation of aorta with figure of 3 sign and inferior rib notching
Perchè non è stata mostrata la LL? Il “trucco” è tutto li’? Una immagine di sovrapposizione di qualcosa che è appesa al collo ?Una ” trappola” del professore?
It is not a “trappola”. Since it was a pre-operative study, only a PA was taken. In my opinion, PA and lateral should be obtained always; but not everybody agree.
4
C’mon, you can do better!
So far, nobody has asked if the patien has hypertension!
L’origine della ipertensione: nefro-vascolare?
4. none of the above
Scoliosis, ribs notching, bilateral apical extrapulmonary lesions, and mediastinal widening can be seen all together in a patient with neurofibromatosis (NF) like this one.
I wouldn´t say this patient have pulmonary hipertension (PH).
Are there any association between NF and PF?
Nipples are a bit assymetric. May be one of the “nipples” is a cutaneous neurofibroma.
I think that the patient has no arterial hypertension, and no difference in arterial pressure between upper and lower extremities. Do you agree, Mr Muppet?
Yes, you are right. As you were before. Congratulations
Thank you professor. I am anxious to see your next case …