This case was sent by my good friend Alberto Villanueva. Muppet made the diagnosis right away (he is gifted!) and wants to share the images with you. They belong to a 17-year-old boy with moderate dyspnea.
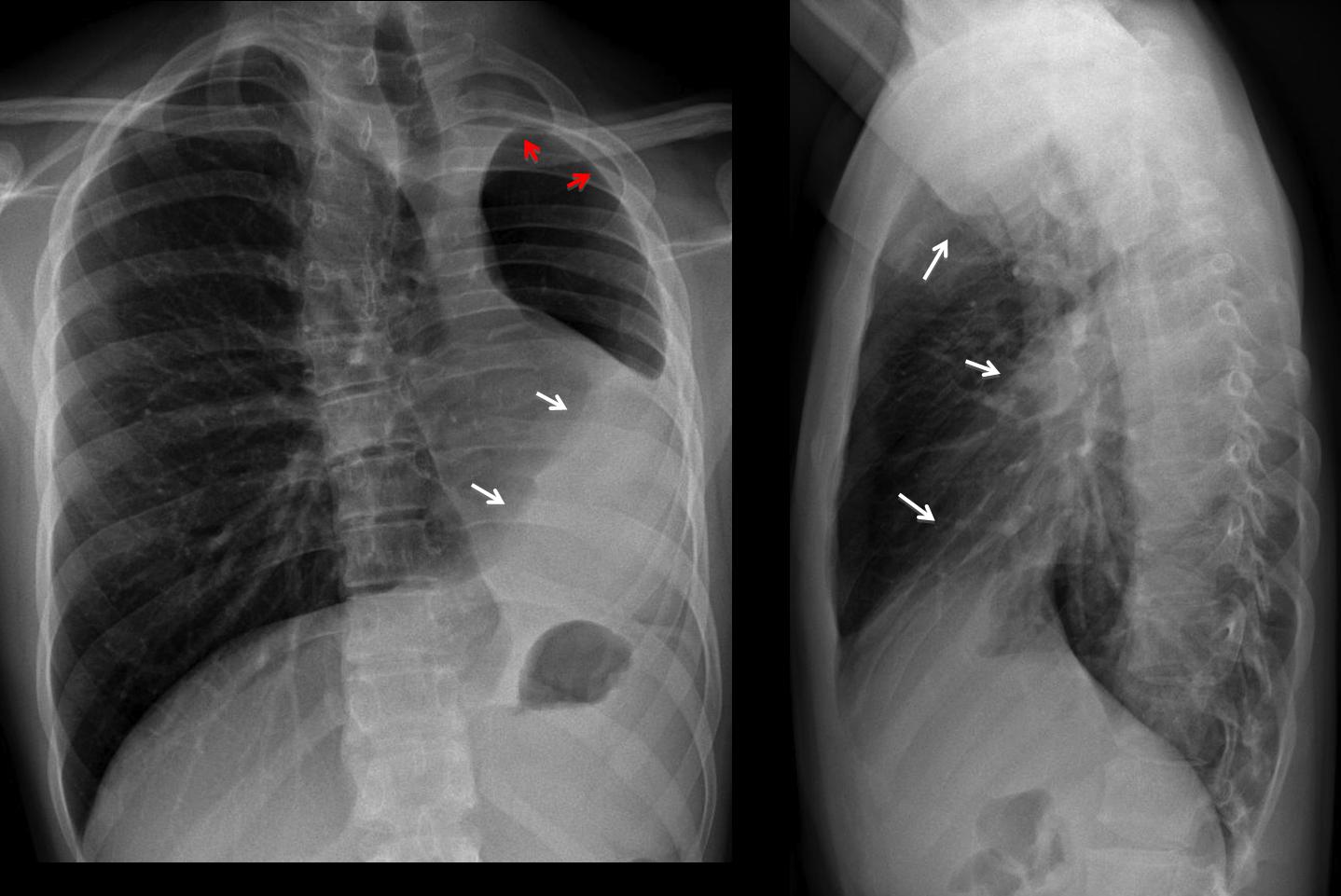
PA film shows a small left hemithorax with a triangular opacity at the base (arrows). There is apparent pleural thickening at the apex (
red arrows). Marked mediastinal shifting is seen. On the lateral view, the anterior clear space is much enlarged (arrows).
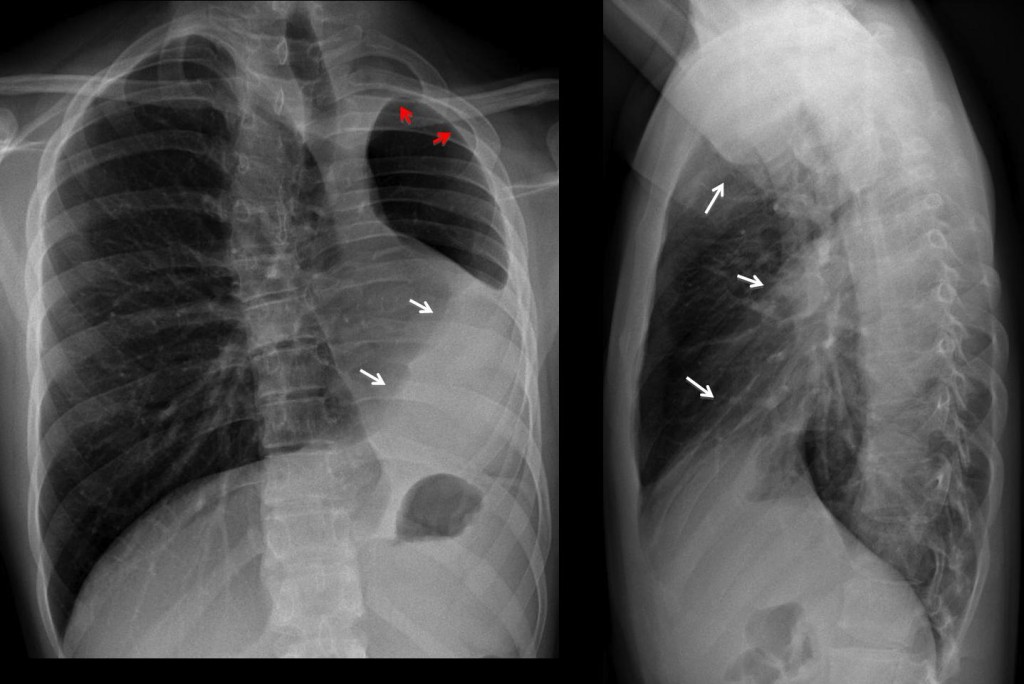
Fig. 1
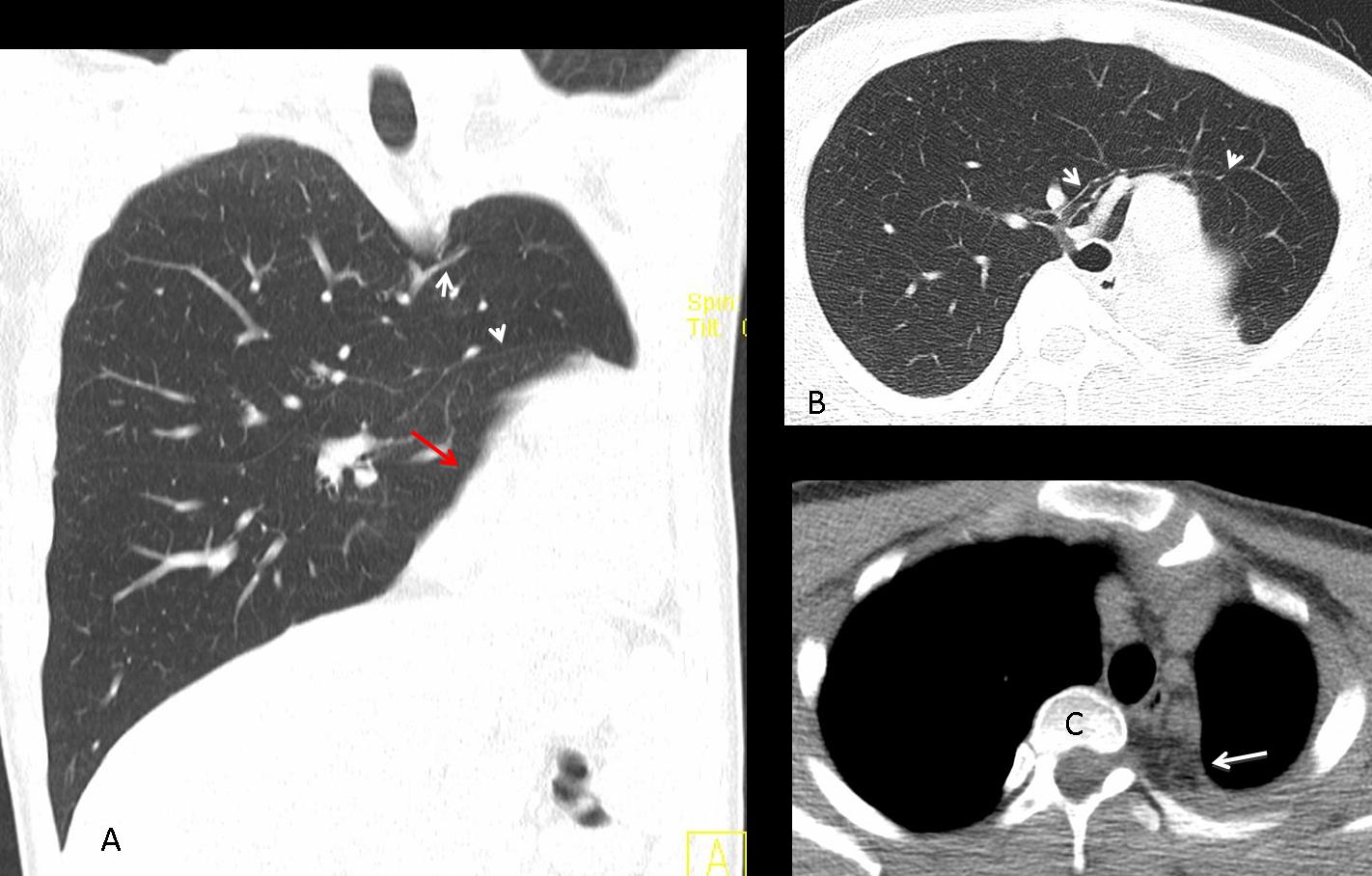
Although the radiographic appearance is puzzling, the images are very suggestive of congenital agenesis of the whole left lung (see Mata et al. European Radiology 6:403-414, 1996). In some cases of agenesis, there is marked expansion of the contralateral lung, which herniates through the anterior clear space and occupies the opposite hemithorax, making with the left chest wall. Bronchi and vessels cross the midline (Fig 2 A, B arrows). The triangular opacity at the left base is due to the rotated heart (Fig 2 A, red arrow). The apparent apical pleural thickening is mostly due to expanded extrapleural fat compensating for the volume loss (Fig 2 C, arrow).
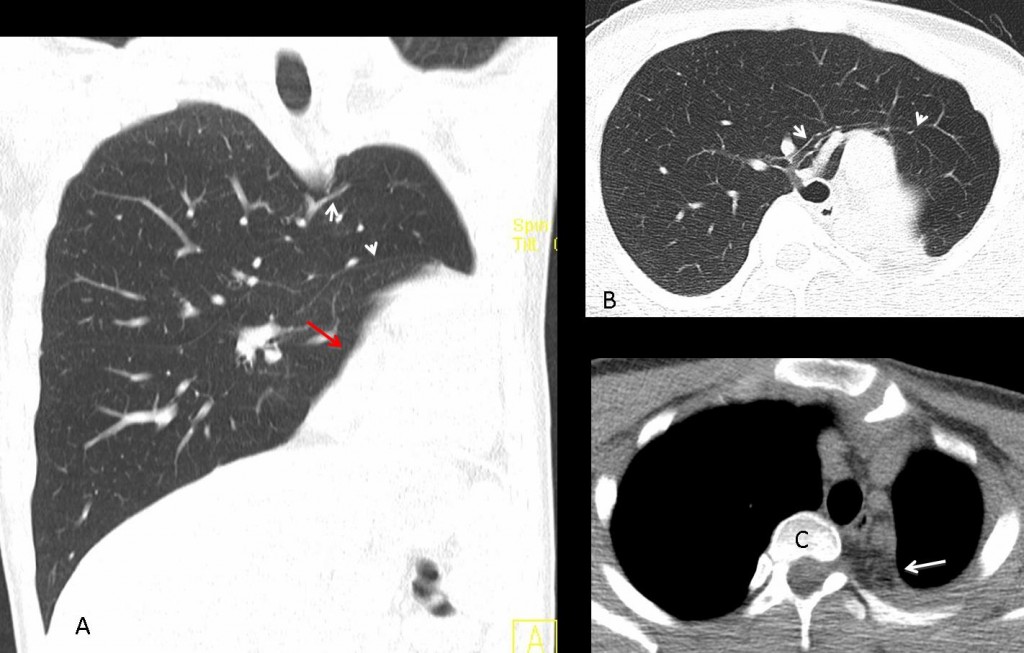
Fig. 2
Final diagnosis: congenital agenesis of left lung (atypical presentation)
Congratulations to Xose, who suggested the right diagnosis
Teaching point: usually, agenesis of one lung presents as a white hemithorax with shifting of the mediastinum towards the affected side. Occasionally, the contralateral lung expands markedly, giving the wrong impression of partial volume loss of the affected side, as in the present case.




3. LLL collapse
chest x ray , frontal and lateral views.
findings:
reduced left lung volume .
reduced intercostal spaces .
mild right convex scoliotic deformity .
cardio-medistinal sift to the left .
trachea is shift to the left , the left main bronchus is not clear .
compensatory increased right lung volume with increased pulmonary vascularity .
small aerated left lung with attenuated vascularity ?? Could be bronchial arterial flow .
left scapula is low positioned relative to the right side ..
homogenous opacification of left lower lung zone with silhouetted left hemidiaphragm, obliterated left pleural angel.
No evidence of rib fractures or resection or previous operation.
Opinion
Picture is suggestive of left lung hypoplasia , with low positioned shoulder .
Mediastinal shift to the left, the left lung much smaller with markedly diminished vascular structure. Options 2&3 can be ruled out, Option 1 is a possibility but i choose no. 4:
Possibly congenital absence of left pulmonary artery.
I am nor saying it’s the right answer; but why are you eliminating chronic pleural thickening?
i ruled out chronic tb pleural thickening because the lung or actually both lungs show no residual tb related opacities or granulomas.
Complete left lung colapse + Right lung herniation
I do apologize for been quite lazy to describe all signs.
– Opacification of the left lower lung zone which obliterates the left hemidiaphragm
– Apparent pleural thickening on the left
– Gastric bubble in place
– Small left lung with diminished vascularity
– Displacement of the mediastinum to the left
– Compensatory hyperinflation of the right lung
“The apparent pleural thickening (as you noted in case 6) is secondary to extrapleural fat, which increases and expands to compensate for the diminished lung volume”.
Option 1 is ruled out because as you also said in case 6 :”hypogenetic lung syndrome, secondary to congenital absence of one or two lobes of the lung, almost always occurs on the right side”.
Primary lung hypoplasia is rare and the most common intrathoracic cause of secondary lung hypoplasia is congenital diaphragmatic hernia (especially when it is located on the left side).
I think that the patient has a secondary left lung hypoplasia due to a congenital diaphragmatic hernia, which has been repaired.
Good thinking, but the patient had no congenital hernia, nor was operated on.
Thank you for your comment professor and for giving me the chance to try again!
After a second thought, I see that on the lateral Xray the large area of increased opacity and sharp anterior border, which overlies the thoracic spine, descends till the lower border of the gastric bubble, whereas the left hemidiaphragm is completely obscured (not only its posterior edge). So, it can not be a displacement of the left major fissure due only to LLL collapse, nor an increase of the extrapleural fat.
On the PA xray, there is a pleural-based lobulated area of increased opacity which projects over the left scapula and is continued with the increased opacity area projecting on the left lower lung zone. I think also that I see an air-bronchogram sign projecting on the cardiac silhouette close to a line which must be the posterior (displaced) junction line.
Is it chronic Tb pleural thickening ? may be in conjunction with LLL collapse? Did I mixed it up? I envy the Muppet …
I also envy the Muppet.
Answer tomorrow.
the boy is not in pain? is somethink chronic right?
3 option is off. i cant see the heart and the left hemidiaphragm.where is the heart borders?
there is cardio-mediastinal-pulmonary shift to the left.
there is shift of the right lung to the left hemithorax.
only a part of the left lung can we seen. there is atelektasis or absence of the LLL.
but i think is somethink chronic,somethink congenital.
on the right we have three ribs in two vertebrals or one of these is in hemivertebra?
in congenital diaphragmatic hernia we have vertebral anomalies?
I don’t know. Why don’t you look it up and tell us?
Atelettasia LLL, con iperventilazione compensatoria del polmone dx e “shift” mediastinico….ma non solo!In LL è visibile ispessimento pleurico, posteriormente, nonchè livello idro-aereo, intratoracico.Scoliosi dorsale alta dx-convessa , con difficile visualizzazione del soma di T4e T5.Penso allora, se Mantoux positiva e QuantiferonB positivo, ad una TBC pleuro-polmonare con stenosi bronchiale e fistolizzazione pleuro-polmonare e spondilite specifica.
left lung agenesia
Good. Better late than never
Complimenti al dott.Strangelove. Non avevo mei visto una agenesia polmonare, unilaterale.Pertanto , perdonatemi , alcune cosiderazioni:1) perchè la scoliosi è dx-convessa, a meno che non ci siano anomali vertebrali associate, essa dovrebbe essere sx-convessa e “seguire” l’iperespansione compesatoria verso il lato agenesico,come lo “shift”mediastinico. 2)sono presenti altre anomalie associate nel soggetto, a carico di altri organi?.3)Fa’ parte di una Sindrome malformative?.4)Vi è una anomala asimmetria anche del torace all’esame obiettivo?.GRAZIE!