Dear Friends,
Summer is near and Muppet wants to relax and show easy cases. The present one relates to an 80-year-old male with RUQ pain after embolisation of a liver tumour.
Diagnosis:
1. Pulmonary embolism
2. Pneumonia
3. Subpulmonary fluid
4. None of the above
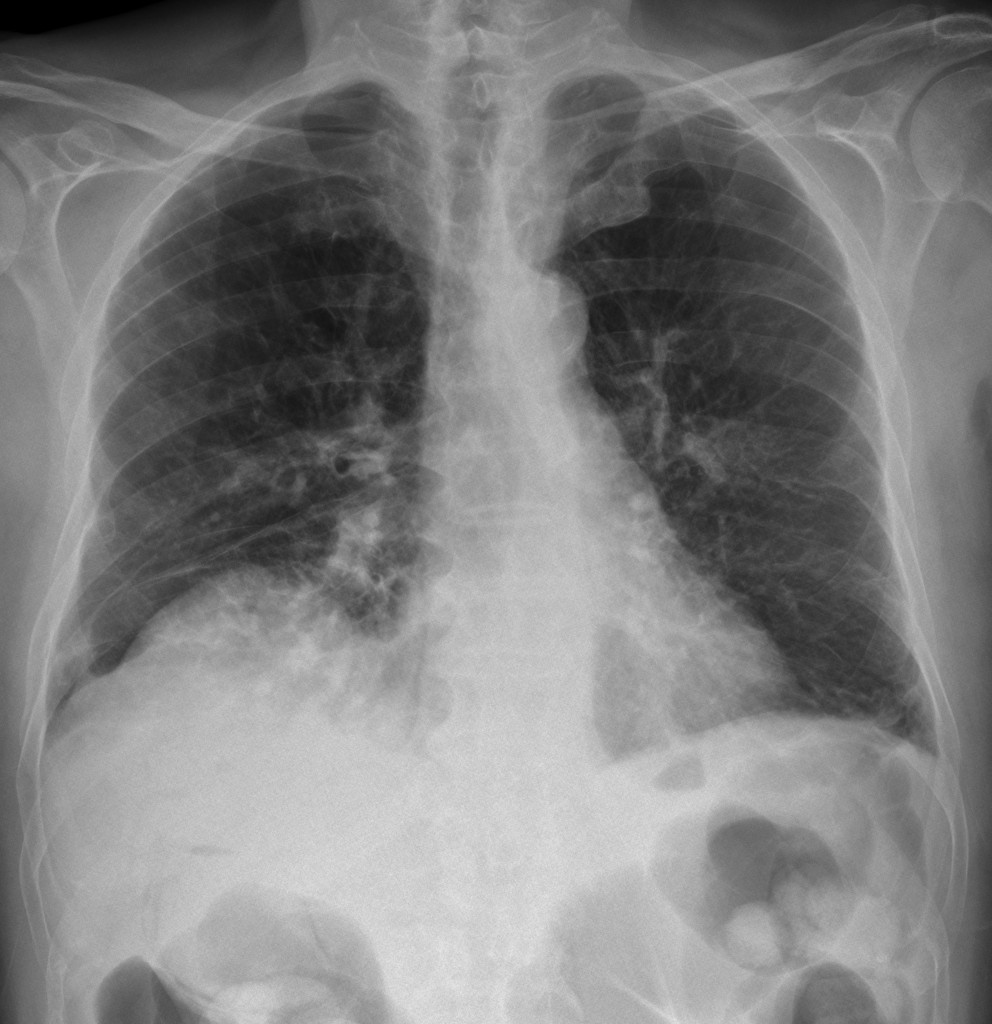
80-year-old male, PA chest
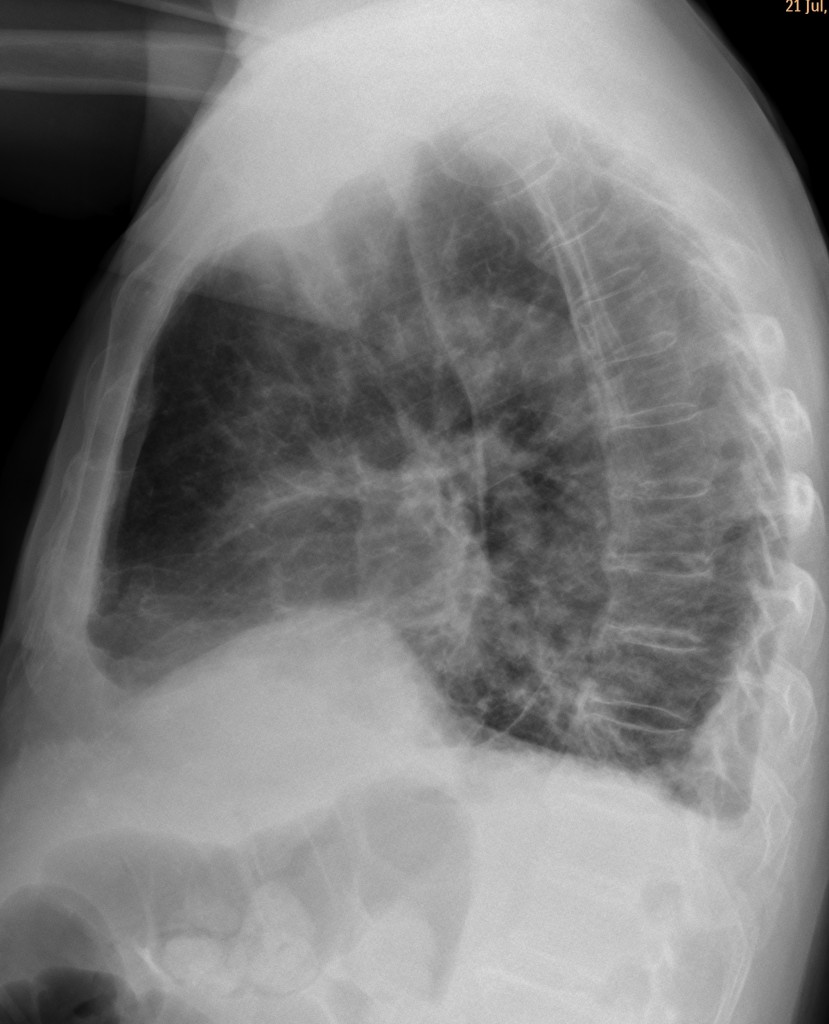
80-year-old male, lateral chest
Leave your thoughts and diagnosis below and look out for the answer next Tuesday.
Click here for the answer to case #68
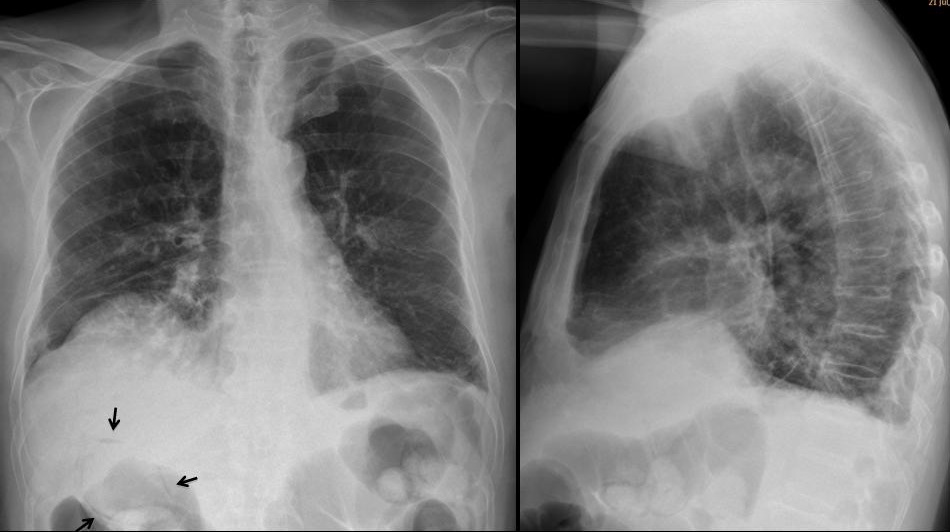
PA chest shows an elevated right hemidiaphragm with ill-defined opacities of the lower right lung. The wall of the gallbladder is outlined by intramural air (arrows). The findings are more obvious in the image that was taken the next day (fig 2 A, arrows).
There is air within the liver (red arrows) and pneumoperitoneum (yellow arrow). CT confirms the intramural gallbladder air (Fig 2 B, arrows) as well as the pneumoperitoneum (B, yellow arrow). The patient died shortly afterwards.
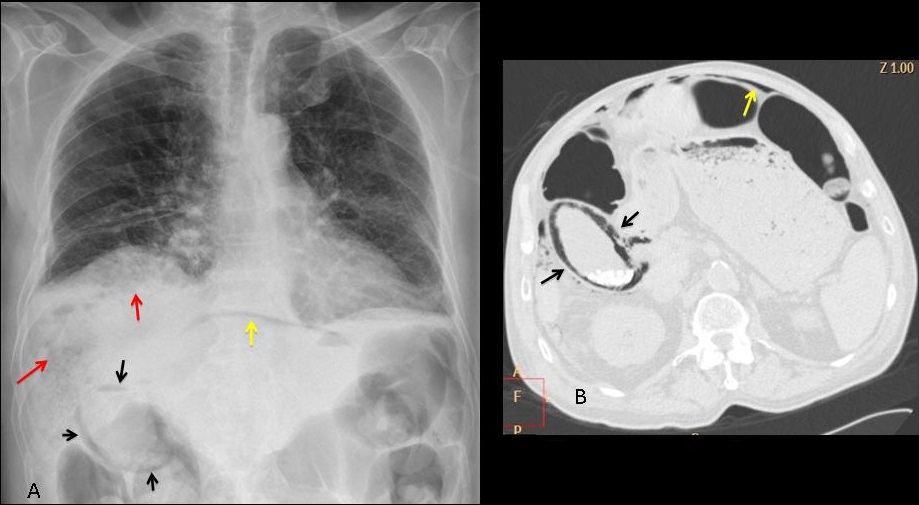
Final diagnosis: gallbladder infarct, secondary to therapeutic embolisation
Congratulations to Dr. Strangelove who made the diagnosis shortly after the case was posted and beat Katerina by 43 minutes.
Teaching point: I was going to stress that you should always look under the diaphragm, but it seems that most of you did.

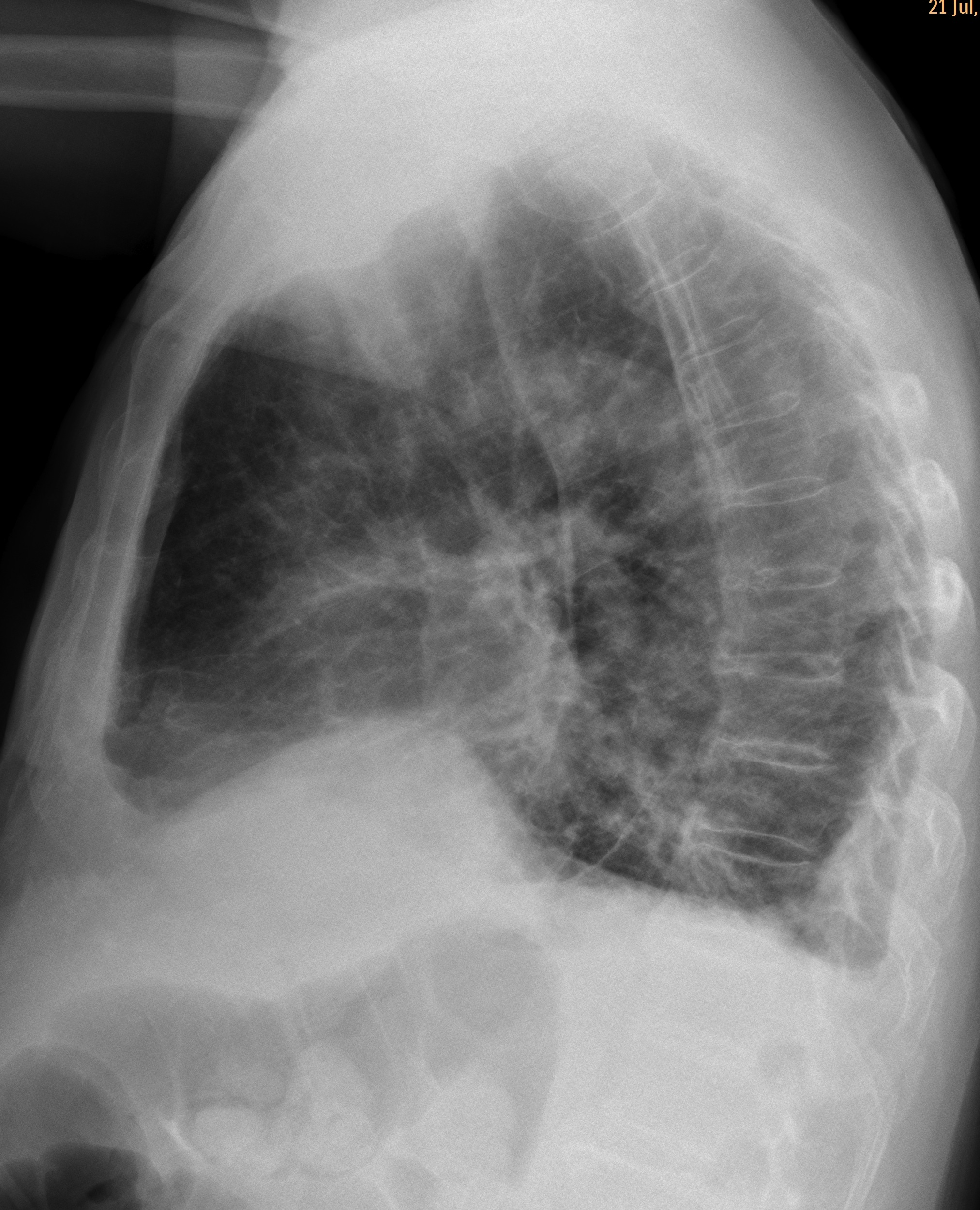


PA and lateral chest radiography shows:
A right side diaphragmatic hump is seen which has smooth well defined outline with an obtuse angle as well as its peripheral location,consistent with extra-pulmonary location;
In view of patient history of embolisation of liver tumour, I think the finding is due to post embolisation sequelae, likely hepatic haematoma.
US and CT abdomen with contrast are recommended .
Emphysematous cholecystitis.
Subphrenic abscess.
Elevation of the anterior-medial portion of the right hemidiaphragm (may be due to eventration, which is common in elderly persons). No lateral peaking of the dome (subpulmonary effusion is ruled off).
Downward shifting of the right hilum, the minor fissure and backward shifting of the right major fissure (reduced volume of RLL – atelectasis).
Pulmonary infiltrates in the RLL and LLL
Air in the biliary tree and may be around the gallbladder (emphysematous cholecystitis due to embolisation?)
subfrenic collection (abscess) with elevation of the right hemidiaphragm.
Right diaphragmatic elevation (sub diaphragmatic compress)with atelectasis of the RLL maybe from the liver tumor (not from ascites)or normal diaphragmatic hump.
small effusion in both costophrenic angles or pleural thickening.
pulmonary infiltrates in LLobes (we must to think for metastasis)
air in the wall of gallbladder or in tumor post embolization?
Una delle complicanze della TACE è la colecistite( in questo caso enfisematosa).La colecistite determina parziale relaxatio diaframmatica, piccolo versamento pleurico e strie disatellettasiche alla base polmonare corrispondente.
dear professor
do you allow me to collect your cases in power point presentation and put here ??
thank you ashraf
If you use them for teaching, it’s OK. Enjoy!
http://www.mediafire.com/?v3417v3ii942bur