Dear friends,
Muppet is delighted to present a case provided by Dr. Vilar. The radiographs are of a 57-year-old woman with a chronic cough and mild fever who also suffered from TB in the past.
Diagnosis:
1. TB, bronchogenic spread
2. Hypersensitivity pneumonitis
3. Sarcoid
4. None of the above

57-year-old woman with a chronic cough and mild fever who also suffered from TB in the past.
Click here for the answer to case #69
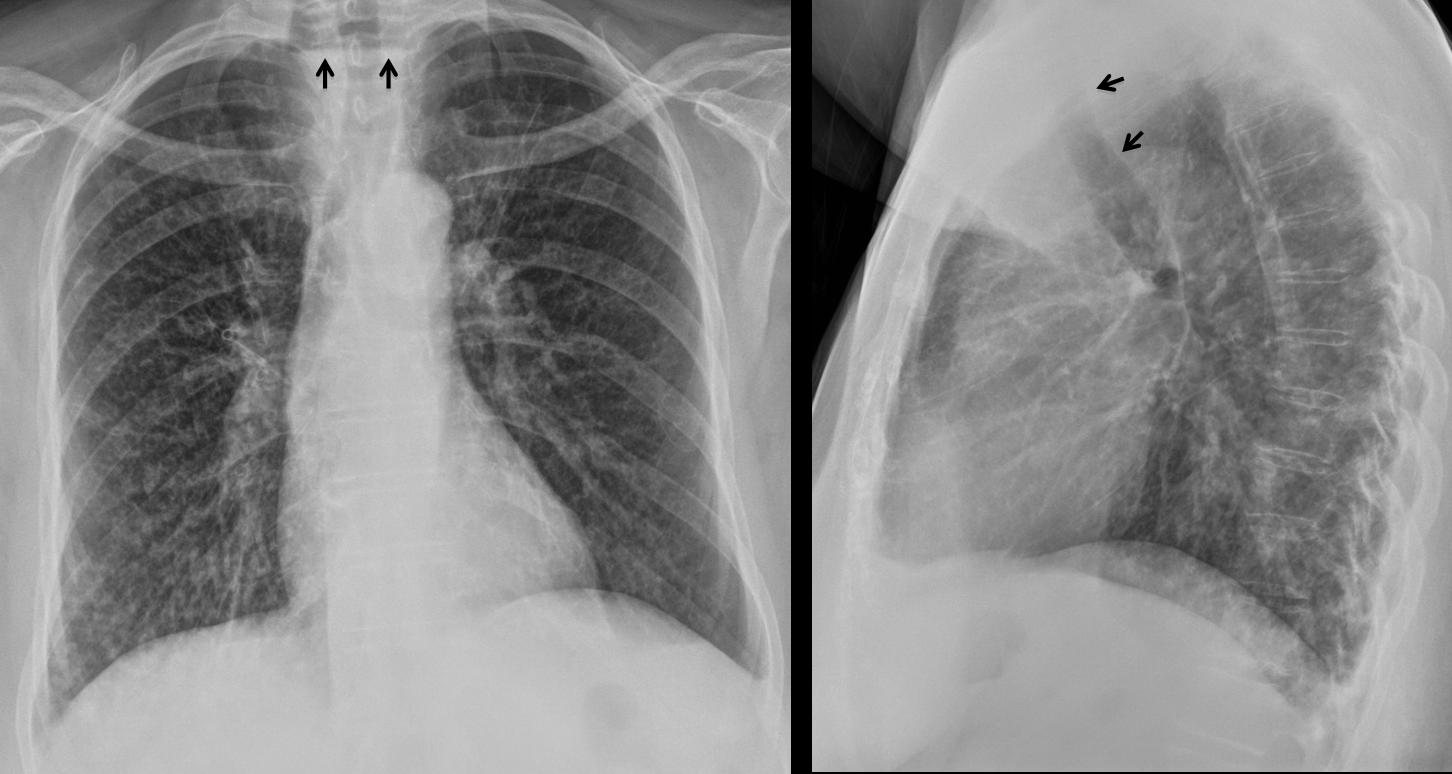
PA chest shows elevation of left hilum, secondary to old TB. There is a diffuse small nodular infiltrate more evident in the right lung, especially in the RLL. An air-fluid level is visible in the upper mediastinum (arrows). The lateral view shows anterior displacement of the trachea (arrows) by a retrotracheal mass.

The findings are highly suggestive of a dilated upper oesophagus or a Zenker’s diverticulum with lung aspiration. Next step is an oesophagogram, which shows a large Zenker’s diverticulum (arrows), with aspirated barium in the trachea (red arrows).
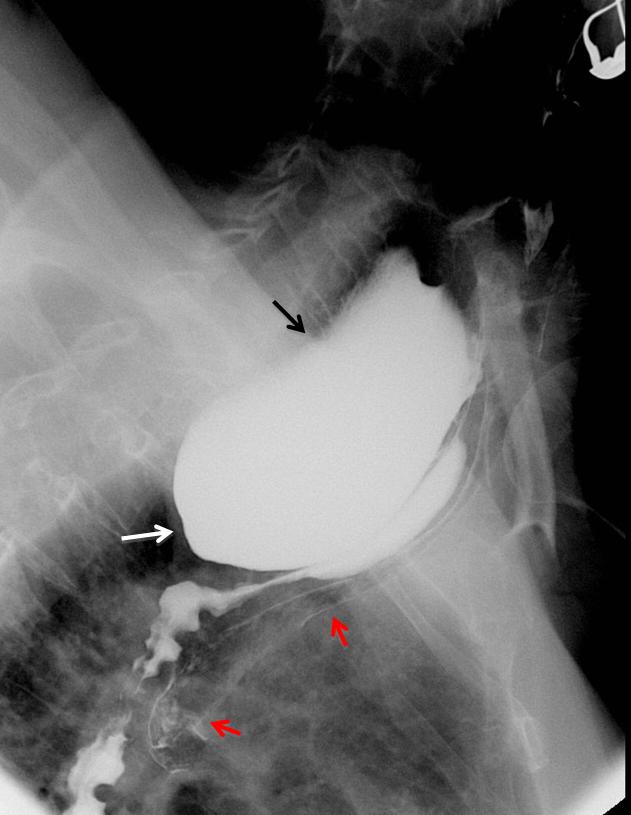
Final diagnosis: Zenker’s diverticulum with bronchial aspiration.
Congratulations to Katerina, who gave an excellent discussion and suggested the right diagnosis.
Teaching point: pulmonary infiltrates in the right lung or RLL should raise the possibility of aspiration. An oesophagogram is an easy procedure to confirm or discard the diagnosis.


It identifies a nodular interstitial pattern in this clinical context is compatible with tuberculosis.
There is no discernible images suggestive of hilar lymphadenopathy or other significant findings.
I will start:
frontal chest raiograph with bilateral wide spread miliary soft tissue shadows(less than 2mm) evenly scattered in both lung feild with no zonal predominancce.No calcification ,no pleural effusion ,no bony anormalities
DD include infective cause( TB.FUNGAL& viral pneumonia),Miliary metastasis,while pneumoconiosis and atypical sarcoidosis come late in the list.
I think miliary TB is the case…based on the previous history of TB with further investigation incluid bronchoscopy with acid and alcohol fast bacilli/culture…we may need CT for multiorgan involvement.
2.None of the above.May be initial caseous pneumonia.Bronchoectatic disease.Diffuse interstitial fibrosis.Overshadowed anterior costo-phrenic sinus.Shifted trachea.Suspicious Ro negative shadow adjacent to trachea-Pneumomedistinum????:)
scleroderma
I agree scleroderma,Because I do not see any thing I usually see,when I am looking,like nodes,or densities other than side view, in front of the aortic arch, seems quite dense so,I also spy’ thickening there in front of the trecha (but yes does look as though it is off to the right if left is right and right is left”.(in Europe like US) ..and possibly why looks öff but on front view looks like it is a steady blurriness,as if it is thickened ?”what do I know..I am seeking my own answers cause,US doctors REFUSE TO EXPLAIN THINGS TO ME! it is disgraceful…
I agree for sklerodermia. At the lateral projection it seems a dilated oesophageus.
At first glance the findings are suggestive of tuberculosis ….
But there is also an air-fluid level projecting at the upper mediastinum at the level of TH3, situated behind the trachea, which is displaced forward. This could be due to a dilated oesophagus due to achalasia, but I don’t see a displacement of the azygooesophageal recess to the right. So I think it must be either a big Zenker diverticulum or upper oesophageal dilatation due to oesophageal carcinoma in the middle 1/3 , which caused aspiration pneumonitis.
I agree scleroderma,Because I do not see any thing I usually see,when I am looking,like nodes,or densities other than side view, in front of the aortic arch, seems quite dense so,I also spy’ thickening there in front of the trecha (but yes does look as though it is off to the right if left is right and right is left”.(in Europe like US) ..and possibly why looks öff but on front view looks like it is a steady blurriness,as if it is thickened ?”what do I know..I am seeking my own answers cause,US doctors REFUSE TO EXPLAIN THINGS TO ME! it is disgraceful…”what is TH3? is that Thoracic ‘as in like T-3?
Why no lymphangitic carcinomatosis due to esophageal cancer?
I don’t think so because there are no Kerley-B lines
I agree. If you don’t see Kerley A or B lines, you cannot make the dianosis of lymphagitis.
There is a diffuse fibronodullar disease most prominent at the inferior lung fields. No prominent lymph nodes. Sarcoidosis i think.
Sarcoidosis, stage 3.
Vi è un evidente livello idroaereo nel mediastino superiore, di origine “digestiva”( in AP). Esso si vede in LL , dietro la trachea, anteriorizzta, e sembra terminare con aspetto filiforme.Tale dato si associa ad opacità micronodulari polmonari, sopratutto in campo polmonare medio-basale dx.Penso allora ad un CR esofageo con metastasi polmonari.Un sorso di Gastrographin è utile completamento alla diagnosi.PS: non sento piu’ Alice!
i am thinking along the lines of katerina and genchi 🙂
Sarcoid – no (no adenopathy, no fibrotic changes)
tb – again no adenopathy, changes too uniform for bronchial spreading and not a miliary pattern either.
hypersensitivity pneumonitis – maybe but there are no clues in patients history
given the cough and fever i vote for aspiration bronchiolitis due to large zenker’s.
Reticulonodular pattern and fluid level in upper esophagus. Could be Scleroderma because it can produces both things. No Tb at all.
Reticulo nodular infiltrates both lung fields predoninantltly right side.
No obvious hilar or mediastinal lymphadenopathy seen.
No evidence of consolidation or pneumothorax in either side.
Cardio mediastinal countour is unremarkable.
No obvious pleural effusion.
Features are more in favour of inflammatory/infective in etiology.
D/D : Endobronchial Tuberculosis.
Further investigation by HRCT.
its miliary tuberculosis.
Image of upper oesophageal dilatation, probably due to distal estenosis due to esclerodermia, or preestenotic dilatation due to a middle 1/3 oesophagic carcinoma, or, less probably, a Zenker diverticulum with pneumonitis due to aspiration.
interstitial lung disease…..likely scleroderma
Legionnailes’ disease? Further investigasion.
Non specific interstitial pneumonia pattern and air fluid level in the upper part of chest. ( because of achalasia) are highly suggestive of Sclerodermia.
Diffuse bilateral infiltration + Compression over the lower trachea, tracheal bifurcation & the left main bronchus from the left side pushing them to the right+Lateral view shows decreased caliber of the Lt main bronchus—-> TB bronchogenic spread
She has a reticulonodular pattern. My differential diagnosis is TB vs lymphangitic carcinomatosis. According to past medical history, it could be reactivation of TB but it need an epidemiologic antecedent (contacts). However, i think that my second diagnosis take more interest because TB increase the risk for cancer.
Oesophageal carcinoma . Dilatation if oesophagus at the lateral X-ray.
Carcinomatosis lymphangitix
Chronic aspiration pneumonitis from Zenker diverticulum.
Besides diffuse minute reticulonodular opacities seen overall lung fields, there are an air fluid level seen at superior mediastinum causes widened of it and mass effect in the form of anterior displacement of trachea; denoting dilated esophegus.
Elevation of left hemidiaphragm, going with decreased volume.
The constellation of appearance and correlation with chronic cough in female patient are highly suggestive of chronic interstitial lung disease SCLERODERMA Vs MYCOBACTERIUM TUBERCULOSIS secondary to dilated esophagus.
Barium swallow and CT chest are recommended.
Reticulo-nodular infiltrates in both lungs.
No hilar or mediastinal lymphadenopathy.
No consolidation in the lungs to be seen.
No pleural effusion.
BUT: air-fluid level at level Th2 in front of the trachea, probably in the esophagus DD big Zenker, Achalasia or tumor. The infiltrates in the lung could be carnimatosis/aspiration pneumonitis.
So answer 4. CT needed
Wouldn’t you rather do an esophagogram first?
Sunt medic pediattu .Am 58 ani ,sunt din Romania . Apreciez la si empatizez cu initiativa dumneavoastra . Cu respect Dr. Ana olareanu
Thank you very much for your kind words.
Mitico professore, grande numero di risposte: è un record ….anche se mancano gli ” aficionades ” classici( Maria ed Albert!)
Alice, Katerina and you are the three Musketeers!
Blog has betwenn 500 and 1000 entries, but the great majority elects to remain incognito.