Dr. Pepe’s Diploma Casebook: Case 18 – SOLVED!
Dear Friends,
My second case of 2013 relates to a 49-year-old man with shortness of breath. PA and lateral radiographs are shown.


Diagnosis:
1. McLeod syndrome
2. Pulmonary embolism
3. Pneumothorax
4. None of the above
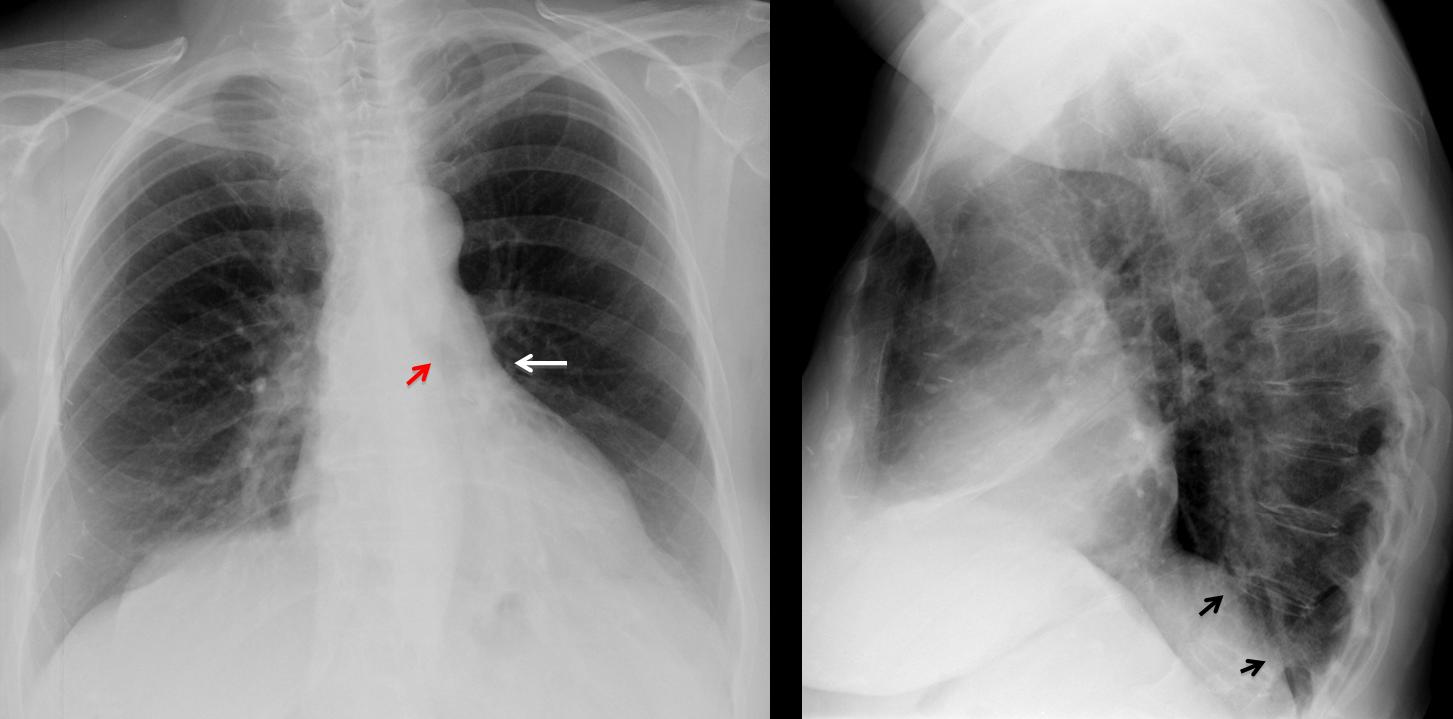
Fig. 1
Findings: PA film shows increased lucency of the left lung. The left hilum appears small because it is descended and hidden behind the cardiac silhouette (arrow). The left bronchus is vertically oriented (red arrow). On the lateral view, there is blurring of the left hemidiaphragm (arrows). These signs are characteristic of LLL collapse with increased lucency of left lung due to compensatory expansion of LUL.
Coronal MIP reconstruction confirms the descent of the left hilum and the vertical orientation of the main left bronchus (arrow). No endobronchial lesion is visible. Coronal CT shows loss of volume of LLL with medial displacement of major fissure (arrow) and bronchiectasis (red arrows). There is compensatory elevation of the left hemidiaphragm.
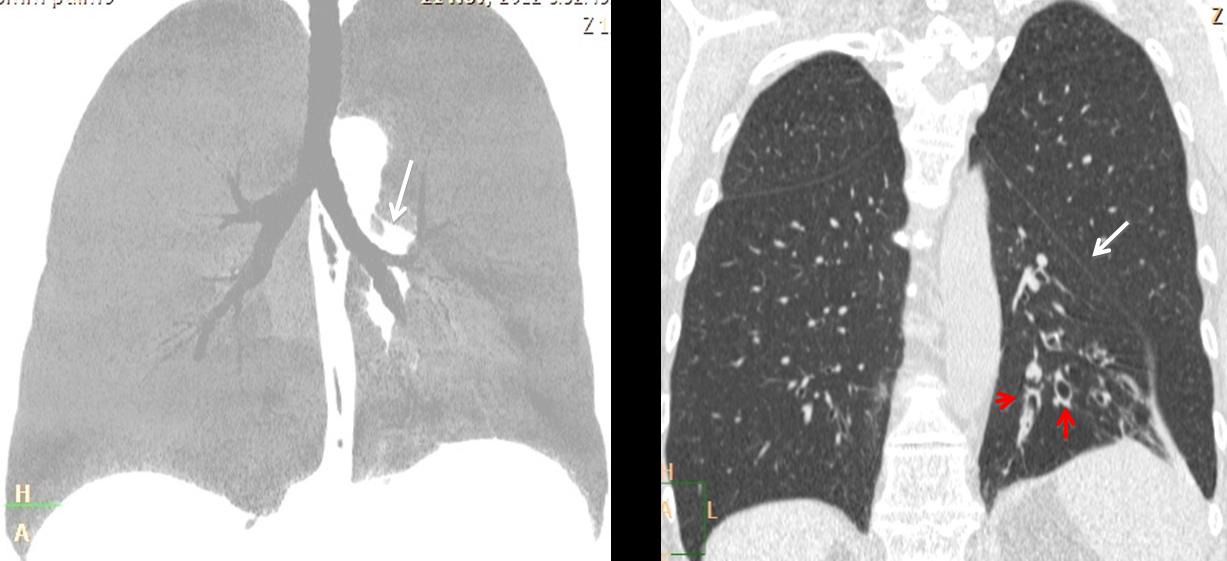
Fig. 2
Final diagnosis: LLL collapse, secondary to bronchiectasis.
The typical appearance of LLL collapse is that of a triangular opacity seen through the heart in the PA view and as posterior lower triangular opacity in lateral view. Additional signs are: descended left hilum, which appears small because it is hidden behind the heart, and increased lucency of the left lung secondary to compensatory expansion of LUL. These changes are described in Fig. 3, below.
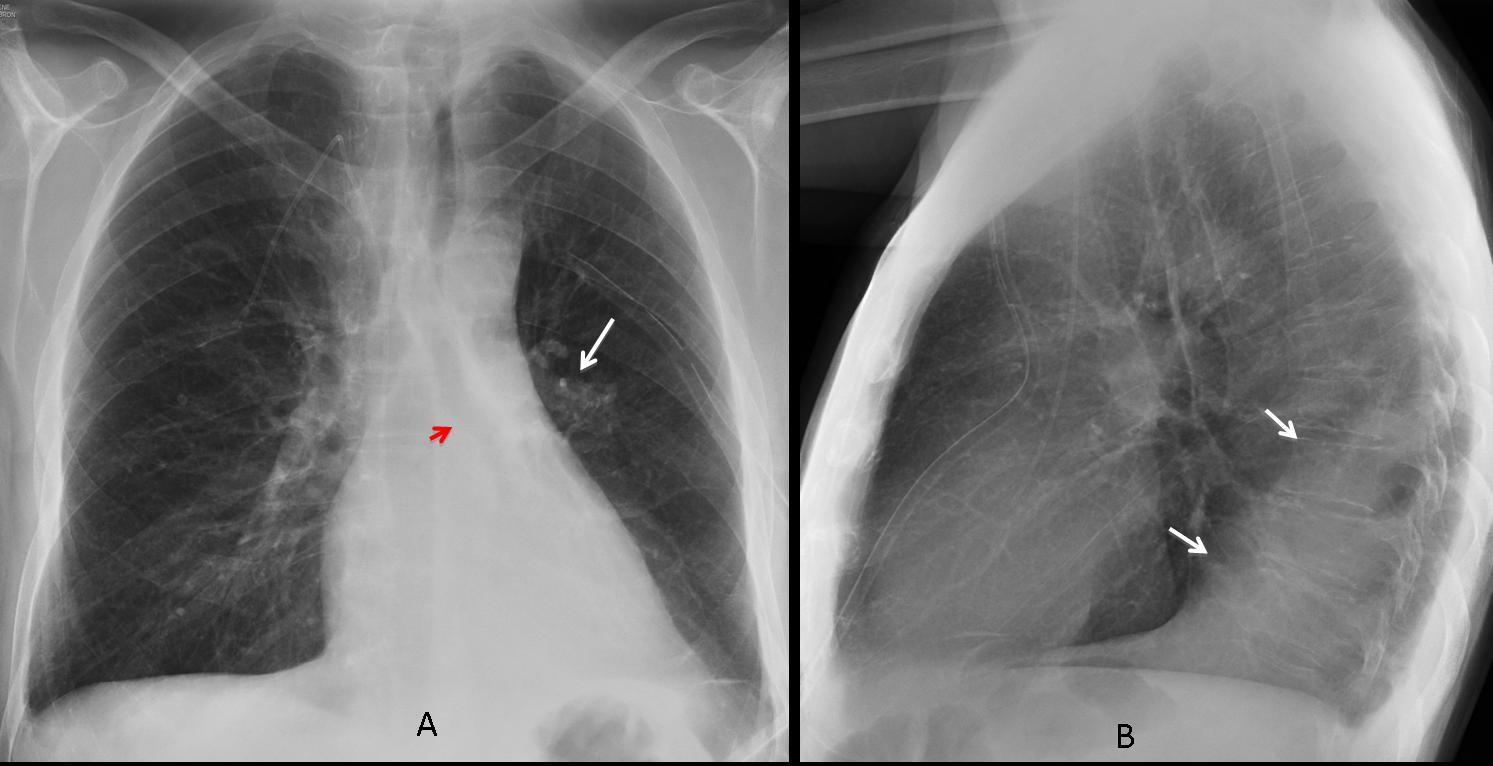
Fig. 3
Fig. 3 A & B (above): transient LLL collapse secondary to mucous plug. PA chest shows the hyperlucent LUL lobe, downward displacement of left hilum (arrow) with vertically–oriented left bronchus (red arrow). Increased retrocardiac triangular opacity, better seen in the lateral view (arrows).
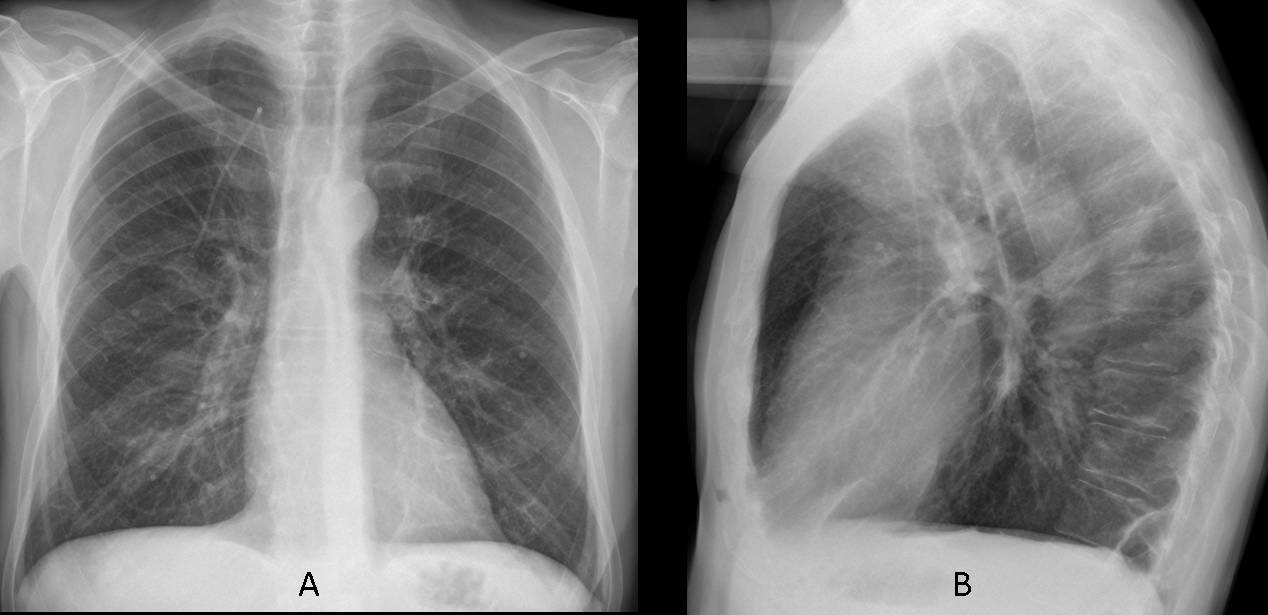
Fig. 4
Fig. 4 A & B (above): radiographs taken six days later, after removal of the mucous plug, show that the left hilum has returned to the normal location and the triangular opacity of LLL collapse has disappeared, as well as the increased lucency of LUL.
In extreme cases of LLL collapse, the increased lucency of the expanded LUL may predominate, giving the deceiving appearance of a hyperlucent left lung. The collapsed LLL lobe is barely visible in the PA view. On the lateral view only blurring of the left hemidiaphragm is seen. The clue to a correct diagnosis lies in correctly identifying the downward displacement of the left hilum (Figs 5-7).
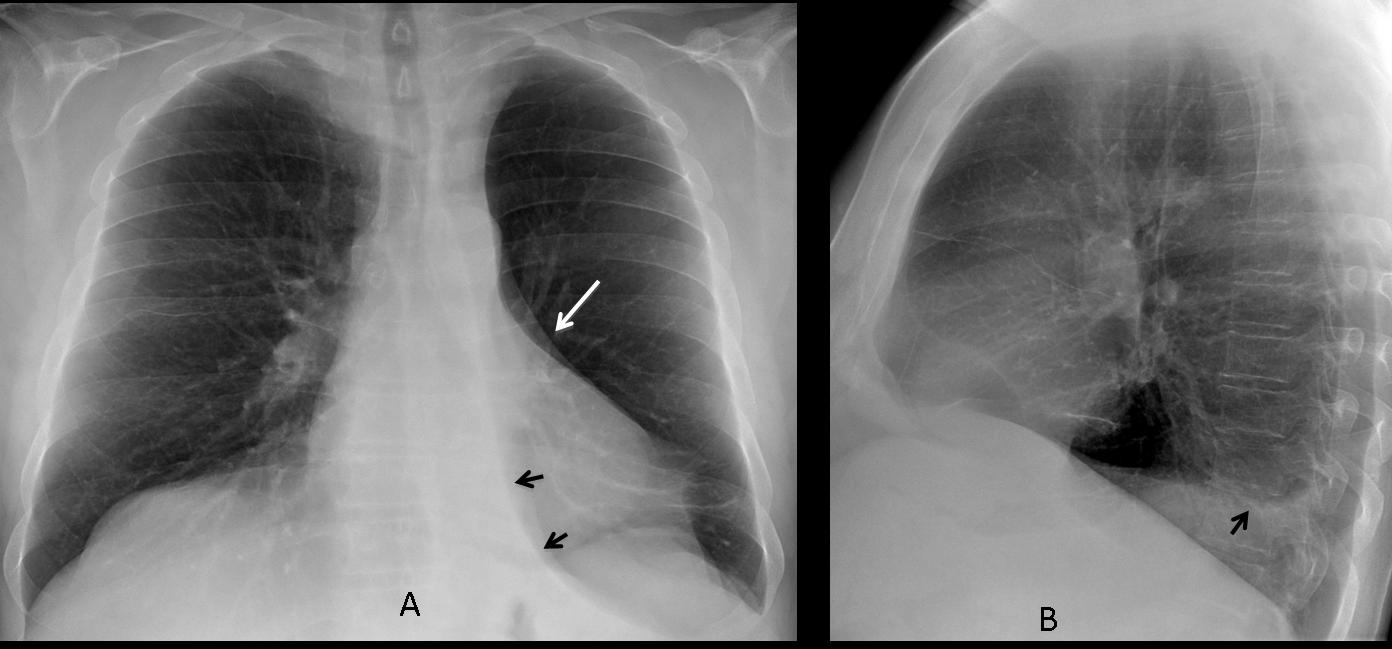
Fig. 5
Fig. 5 A & B (above): pre-op film in an asymptomatic 68-year-old man with marked LLL collapse simulating hyperlucent lung. The collapsed lobe is seen as a small paramediastinal triangular opacity (arrows) and slight blurring of hemidiaphragm in the lateral view (arrow). The clue to the diagnosis is the marked downward displacement of the left hilum (white arrow).
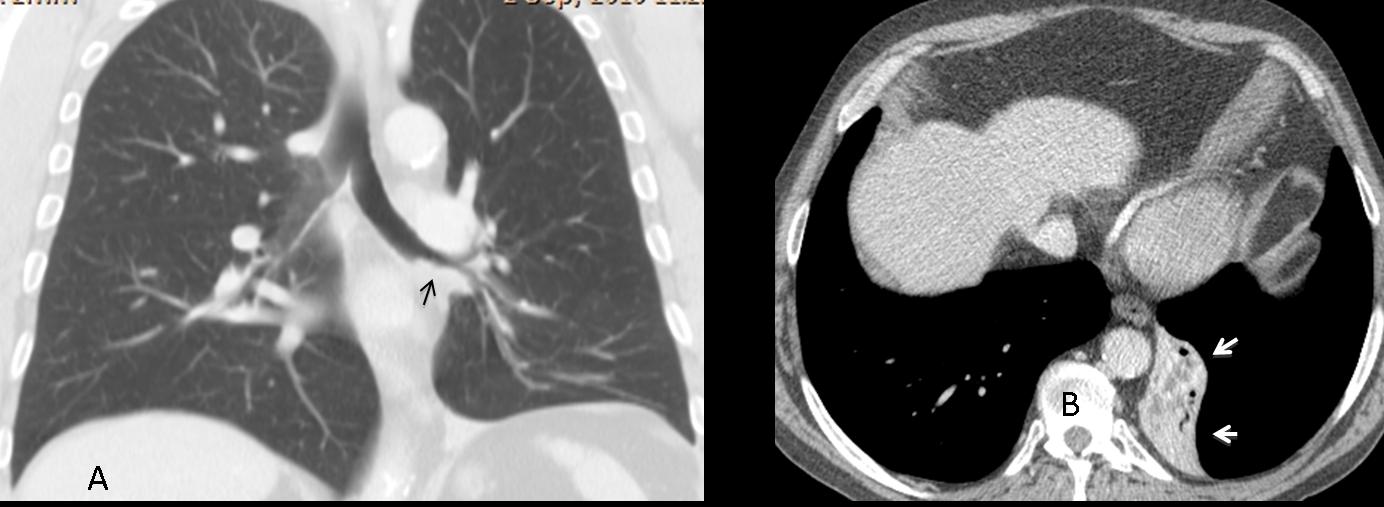
Fig. 6
Fig. 6 A & B (above): coronal CT confirms the downward displacement of hilum and an endobronchial lesion in the LLL wall (C, arrow). The axial view shows the marked collapse of LLL (arrows). Final diagnosis: unsuspected squamous-cell carcinoma of LLL bronchus.
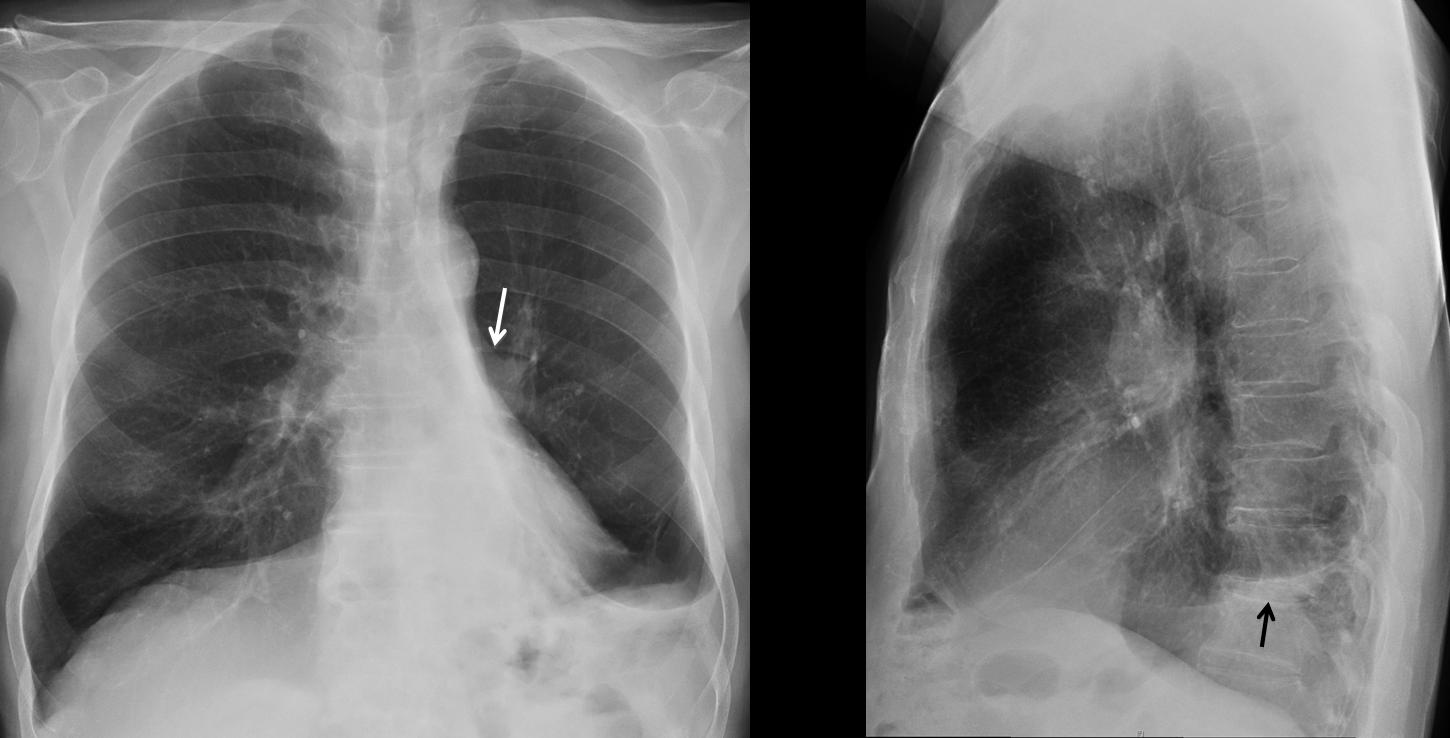
Fig. 7
Fig 7 (above): bronchiectasis with marked LLL collapse. Hyperlucent lung with marked downward displacement of left hilum (arrow) and haziness of hemidiaphragm (arrows). Note the similarity to the previous case.
Although bronchiectasis alone may cause collapse of LLL lobe CT should be done to rule out an endobronchial lesion.
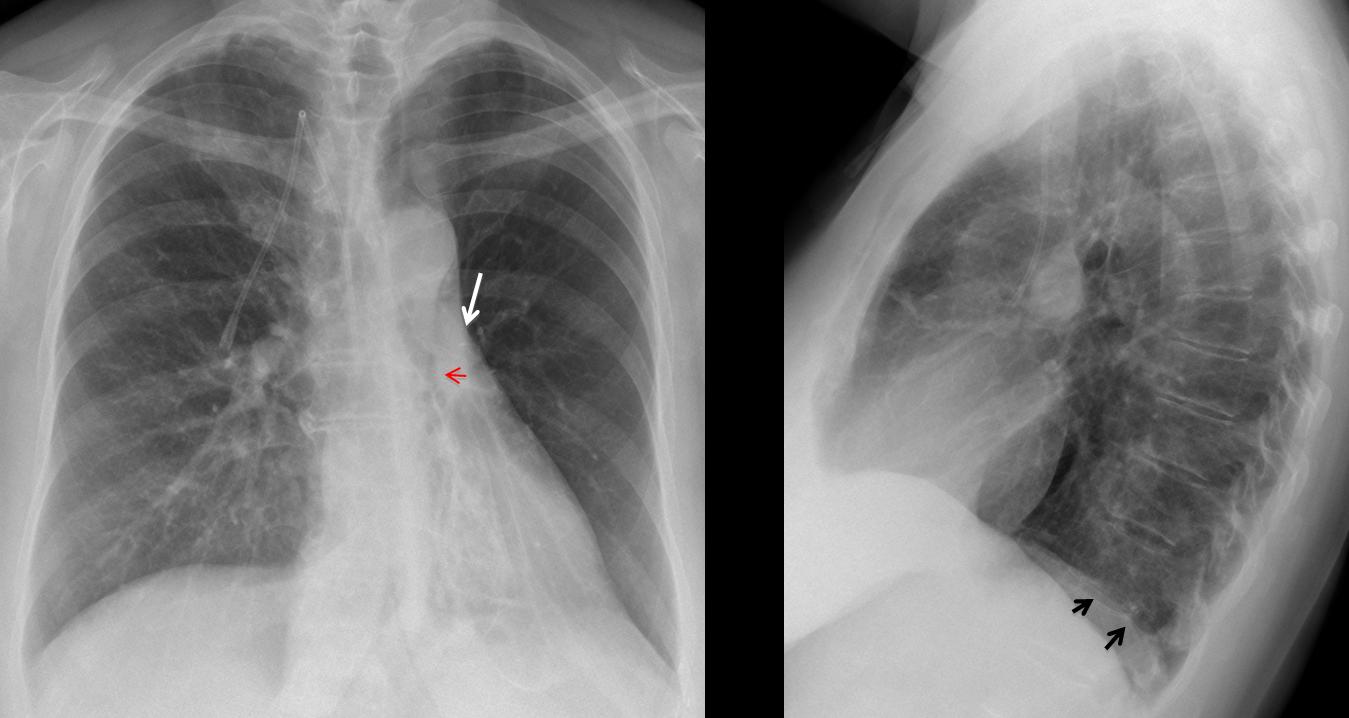
Fig. 8
Fig. 8 (above): 56-year-old female with extreme collapse of LLL attributed to bronchiectasis. Note the marked hyperlucency of the LUL and the downward displacement of the left hilum (arrow). There is a suggestion of an endobronchial lesion in the PA view (red arrow). There is minimal blurring of hemidiaphragm in the lateral view (arrows).
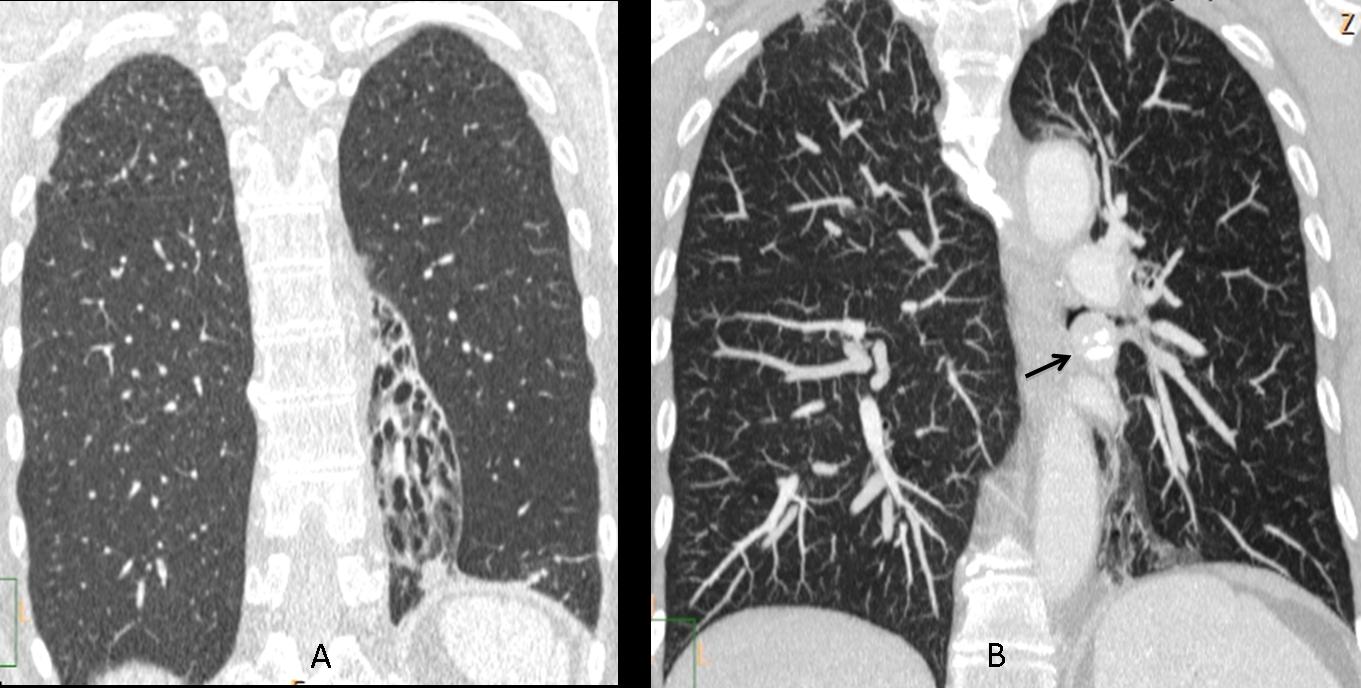
Fig. 9
Fig. 4 A & B (above): coronal CT shows marked LLL volume loss with bronchiectasis secondary to a rounded endobronchial lesion with popcorn calcification (B, arrow). Final diagnosis: endobronchial neuroendocrine tumour.

Fig. 10
Fig 10 (above): surgical resection of LLL may simulate extreme LLL collapse, as in the case above. Note the hidden left hilum, elevation of left hemidiaphragm and triangular paramediastinic opacity. The proximity of the 5th and 6th ribs are a clue to suspect previous surgery (arrow).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- In extreme cases of LLL collapse the compensatory expansion of LUL may predominate, suggesting a hyperlucent lung
- Downward displacement of left hilum, verticalization of left bronchus and haziness of the diaphragmatic contour on the lateral view should suggest the correct diagnosis
- In all cases, CT should be done to exclude an endobronchial lesion
Recommended reading: Unusual pattern of left lower lobe atelectasis. Radiology 141: 331-333, 1981
Case prepared by Dr. Pepe


PE with Westermark sign?
Oligemia of left lung – Westermark’s sign due to pulmonary embolism
Diminished vascularity on the left, the left hilum is lower than usual.
No Westermark sign or hamptons hump visible.
No Pneumothorax either (although there are surgical Clips on the right likely in the thoracic wall- Cause?)
I choose no. 1 swyer-james-mcleod
McLeod syndrome
Swyer James – McLeod
mcleod
Non c’è nè il segno di Westembark, completo, nè il segno di Hampton hump-sign: escludo la Embolia polmonare. Non si vede aria libera in torace. Vi è oligoemia, con iperventilazione , apparente del polmone sx che ha un”volume” inferiore al controlaterale, pur essendo “apparentemente”, iperespanso: quindi sono per la S. di Swyer James -McLeod.
In Westermark sign the oligoemia is more evident. I agree with Mcleod Syndrome.
A word of caution to all of you who answered McLeod: diagnosis cannot be made unless you have an expiratory film that demonstrates air-trapping
In effetti quello che non si spiega è “l’apparente iperventilazione” del polmone sx , con “perdita” di volume dell’emitorace corrispondente e lieve attrazione omolaterale dell’ombra cardio-mediastinica; inoltre in LL si osserva una banda di opacità contro l’immagine cardiaca, nonchè una opacità triangoliforme contro l’ombra cardiaca , alla base polmonare in AP.Pertanto raccogliendo, per buoni , questi altri segni si potrebbe anche supporre una atelettasia del lobo polmonare inferiore sx, ed iperventilazione, per compenso, del lobo superiore.
Since no more answers are forthcoming, I believe final diagnosis can be disclosed. As Genchi Bari said, we are looking at compensatory LUL emphysema, secondary to LLL collapse. It is important to get the findings right to avoid diagnostic mistakes. Detailed answer will be posted shortly.
Congratulations to Dr. Genchi Bari!
Grazie collega dr Pepe ,Il “galactico” sarà contento …..di questo piccolo Bari!