Dr. Pepe’s Diploma Casebook: Case 26 – SOLVED
Dear Friends,
Today I’m showing a case of a 63-year-old man with left heart dysfunction and angor.
Diagnosis:
1. Myocardial tumour
2. Apical hypertrophic cardiomyopathy
3. Myocardial infarction and thrombus
4. None of the above
Post your thoughts below and look out for the answer on Thursday.
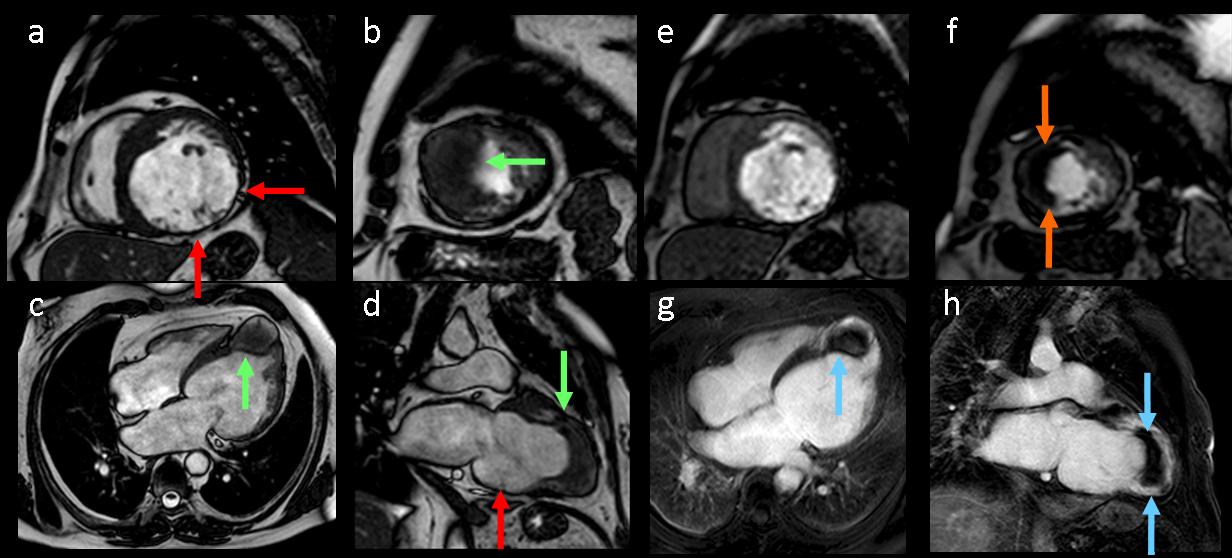
Fig. 1
Findings
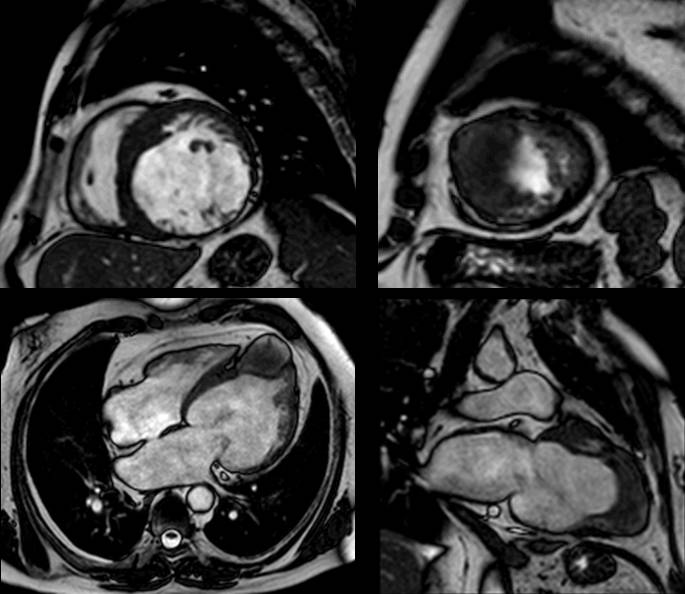
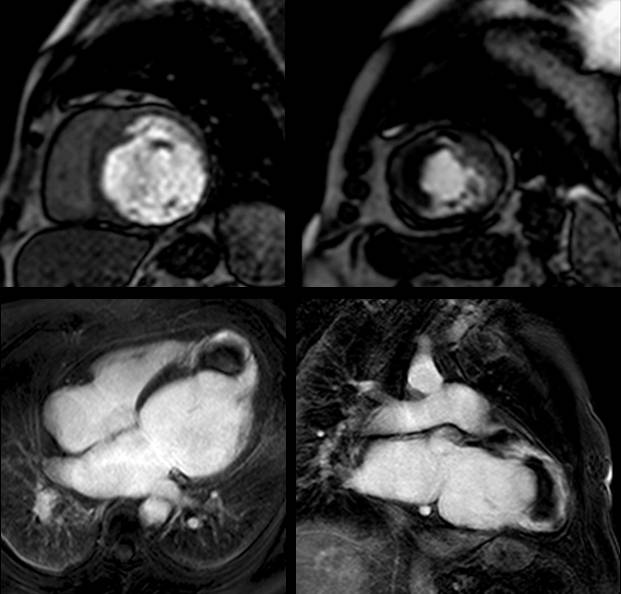
Figure 1 (a-h): End-diastolic steady-state free precession cine-MRI basal short-axis (a), apical short-axis (b), four-chamber (c), and two-chamber (d) views show dilated left ventricle and asymmetrical thickness of the left ventricle wall, with thinning (red arrows). An anterior hypointense apical mass (green arrows) can also be seen. On basal (e) and apical (f) short-axis views at dynamic first-pass perfusion during administration of gadolinium contrast, the apical mass does not enhance (orange arrows). Four-chamber (g) and two-chamber (h) delayed T1-weighted inversion recovery sequences obtained after contrast injection show hypointensity of the apical mass and transmural enhancement of the apical wall (blue arrows).
- Focal hypertrophic cardiomyopathy and myocardial tumor show enhancement after contrast administration
- Focal thinning of the myocardium in a segmental distribution is a feature of scar due to infarction
- Apical intracavitary thrombus is the most frequent intracavitary mass in patients with infarction
- Thrombus does not enhance during perfusion
Final diagnosis: Myocardial infarction and thrombus
Myocardial scar
Ischaemic heart disease is a cause of myocardial thinning. Thinning of the myocardial wall at rest is a reliable feature of scar tissue resulting from myocardial injury. The entire process of scarring usually takes about four months to develop from the time of acute injury.
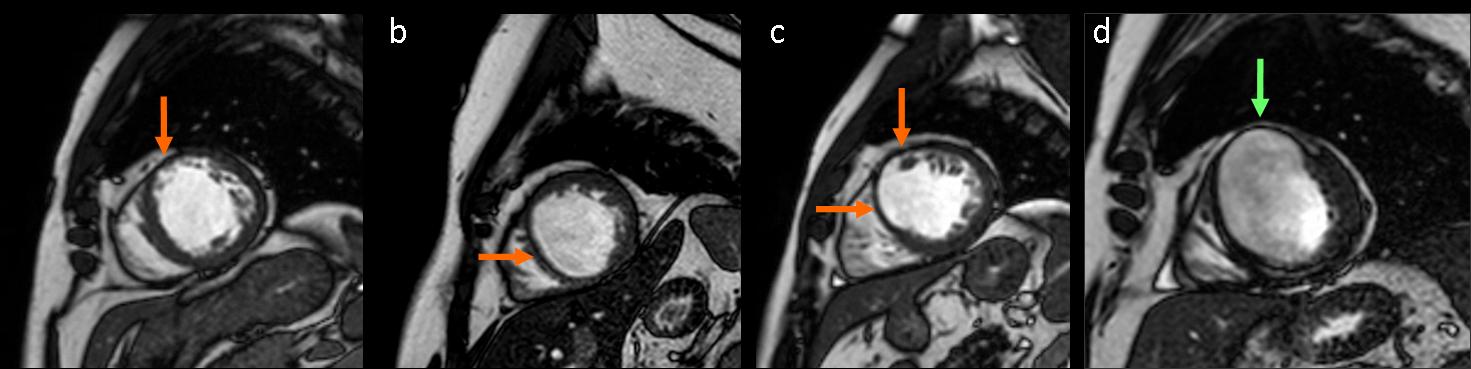
Fig. 2
Figure 2 (a-d): short-axis steady-state free precession cine-MRI in four different patients shows myocardial thinning due to scar (arrow) in the anterior apical segment (a), in the septal apical segment (b), in the anterior and septal apical segments (c); scar and aneurysm formation at the anterior wall of the left ventricle (arrow) (d).
Scarring of the myocardium is the cause of akinetic and dyskinetic areas, aneurysm formation, or left ventricular dilatation.
Figures 3a to 3d show two-chamber, steady-state, free precession cine-MRI images in four different patients show myocardial infarction with scar, aneurysm formation, and left ventricular dilatation.

Fig. 3a

Fig. 3b
Fig. 3c

Fig. 3d
Delayed enhancement
Myocardial necrosis is characterised by delayed enhancement, typically seen at the subendocardial myocardium and extending toward the epicardial myocardium. Infarct severity is related to the transmural involvement.

Fig. 4
Figure 4: Four different patients with myocardial necrosis. Short-axis T1-weighted inversion recovery sequence obtained after contrast injection. Note different degrees of delayed enhancement from subendocardium (a) to transmural (d) (arrows).
Delayed enhancement: Prognostic value
The extent of hyperenhancement has prognostic value: transmural extension, number of affected segments, and detection of no-reflow phenomena are hallmarks of improvement.
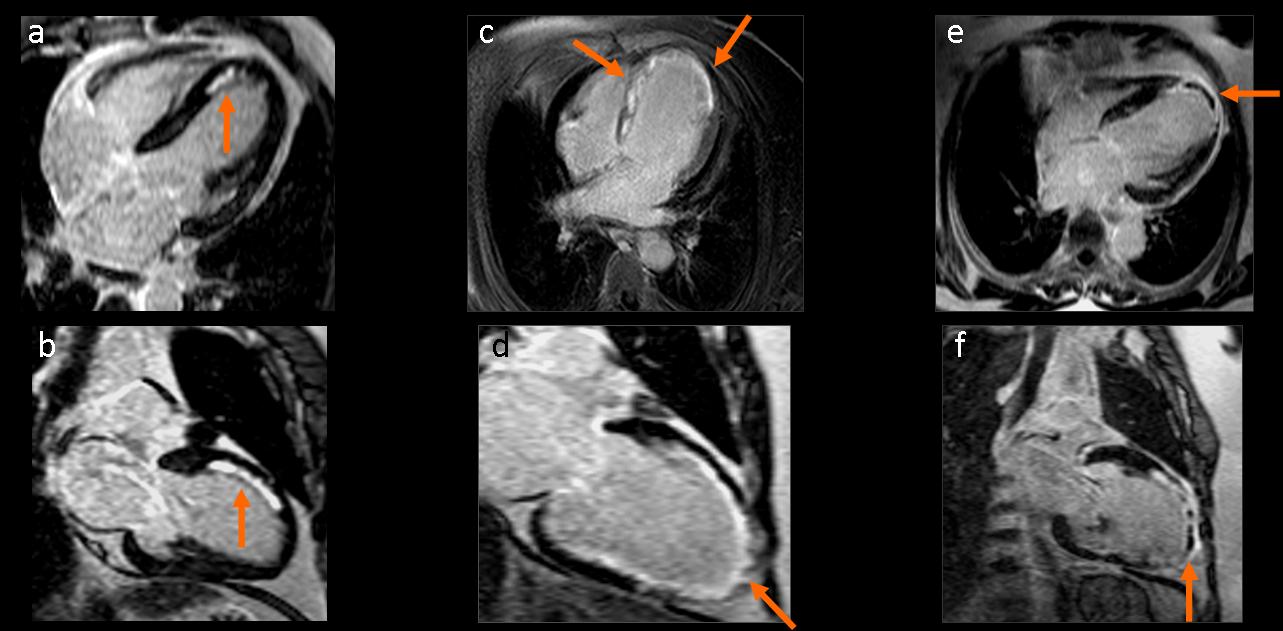
Fig. 5
Figure 5. Delayed enhancement MR image in 6 different patients: (a, b) Subendocardial enhancement of less than 50% of the myocardial wall (arrows). (c, d) Transmural enhancement indicates non-viable myocardium (arrows). (e, f) hypoenhanced area (arrows) within hyperenhanced myocardium is consistent with microvascular obstruction.
Mitral regurgitation
Ischaemic cardiomyopathy is a cause of ‘functional’ chronic mitral regurgitation, resulting from left ventricular and annular dilatation and abnormal left ventricular wall motion. Less commonly, papillary muscle dysfunction or rupture due to myocardial infarction is the cause of acute mitral regurgitation.
Figures 6a and 6b (below): a 50-year-old man with a history of myocardial infarction. Steady-state free precession cine-MRI in four-chamber (a) and long-axis (b) views shows myocardial thinning (orange arrows), dilated left ventricle (yellow arrows), and hypointense area in the left atrium during systolic ventricular phase due to turbulent flow of mitral regurgitation (red arrows). Note bilateral pleural effusion (green arrows) and tricuspid regurgitation.

Fig. 6a
Fig. 6b

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- The most common cause of myocardial thinning is infarct scar
- Transmural extension and number of segments showing delayed enhancement have prognostic value in patients with myocardial infarction
- Thrombus is the most frequent intracavitary mass
- Chronic mitral regurgitation is a complication of infarction
Suggested reading:
- Characterisation of myocardial viability using MR and CT imaging. Eur Radiol. 2007;17:1433-44.
- Ischemic cardiomyopathy: value of different MRI techniques for prediction of functional recovery after revascularization. AJR 2004;182:95-100.
Case prepared by Rafaela Soler MD


myocardial infraction with thrombus.