This week I am presenting a lateral radiograph of the cervical spine in a 45-year-old man with cervical pain and an acute spinal cord lesion after a hang gliding accident.
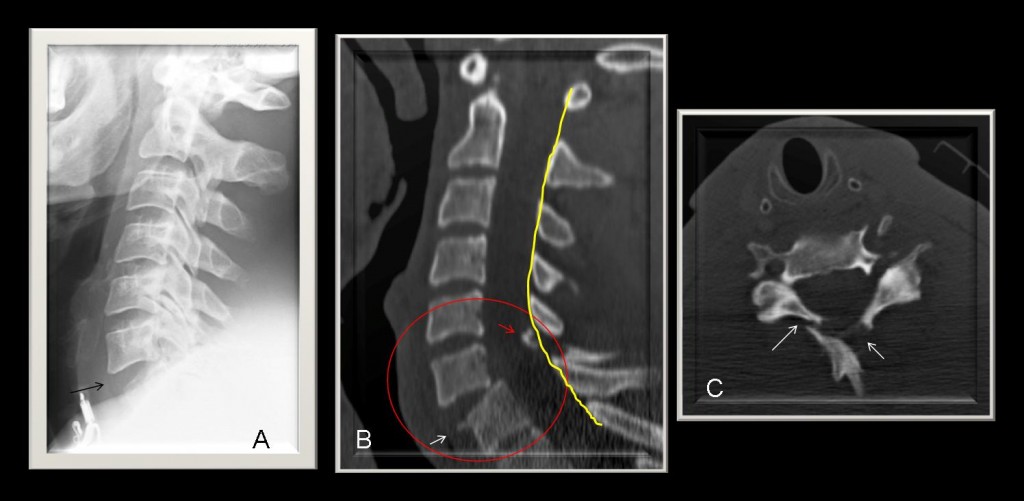
Fig. 1
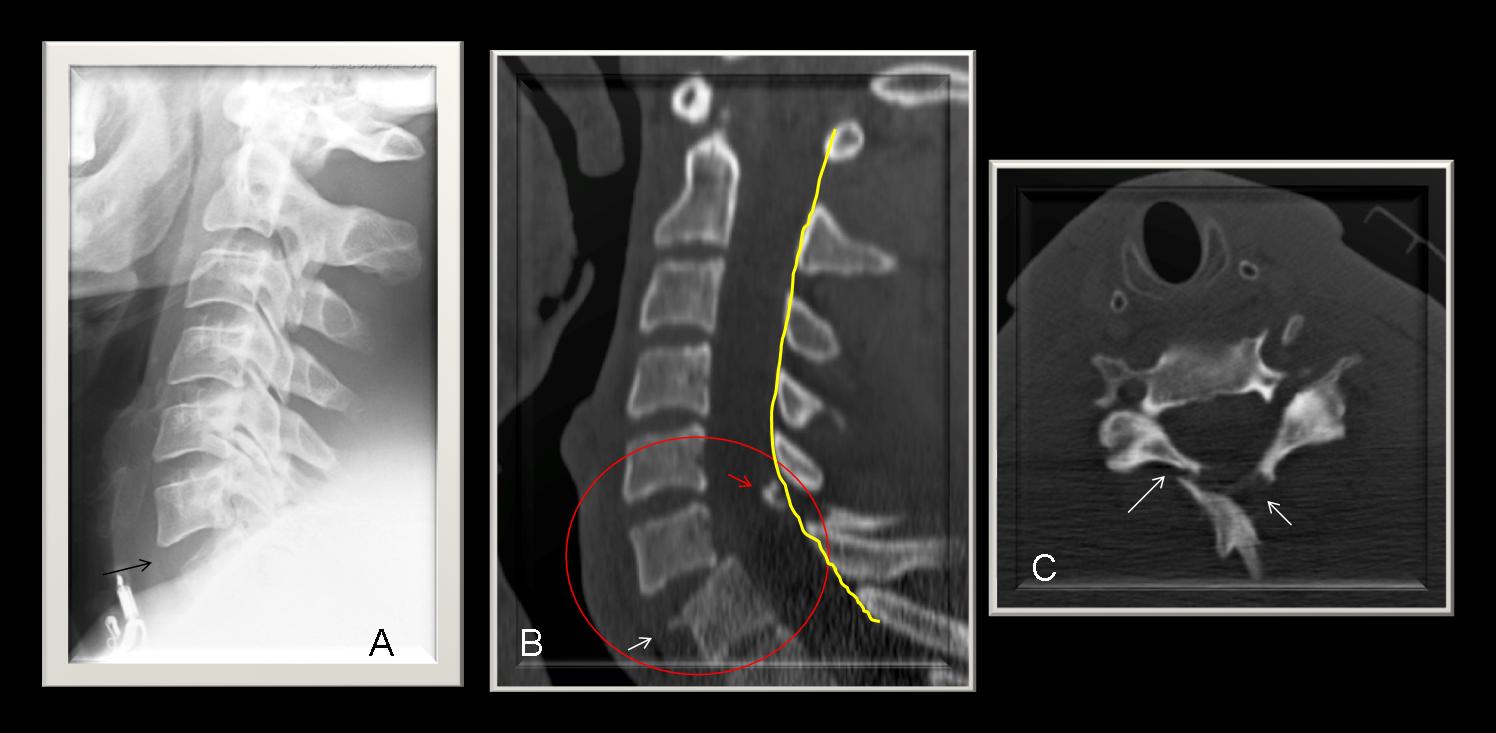
Findings: lateral view of cervical spine shows forward displacement of C6 over C7 with anterior widening of C6-C7 disc space (A, arrow). Sagittal CT confirms anterior widening of C6-C7 disc space and less than 50% anterior translation of C6. Avulsion fragment arising from the anterior aspect of C7 (B, white arrow) and fracture with comminution of the posterior elements (B, red arrow). The spino-laminar line (yellow arrows) is not altered. Axial CT shows comminution of laminae (C, arrows). The lesion was erroneously diagnosed as a flexion fracture because of the anterolisthesis, without considering the anterior diastasis and absence of diastasis of the posterior elements. Cranial halo traction was applied and the radiograph worsened (Fig. 2).
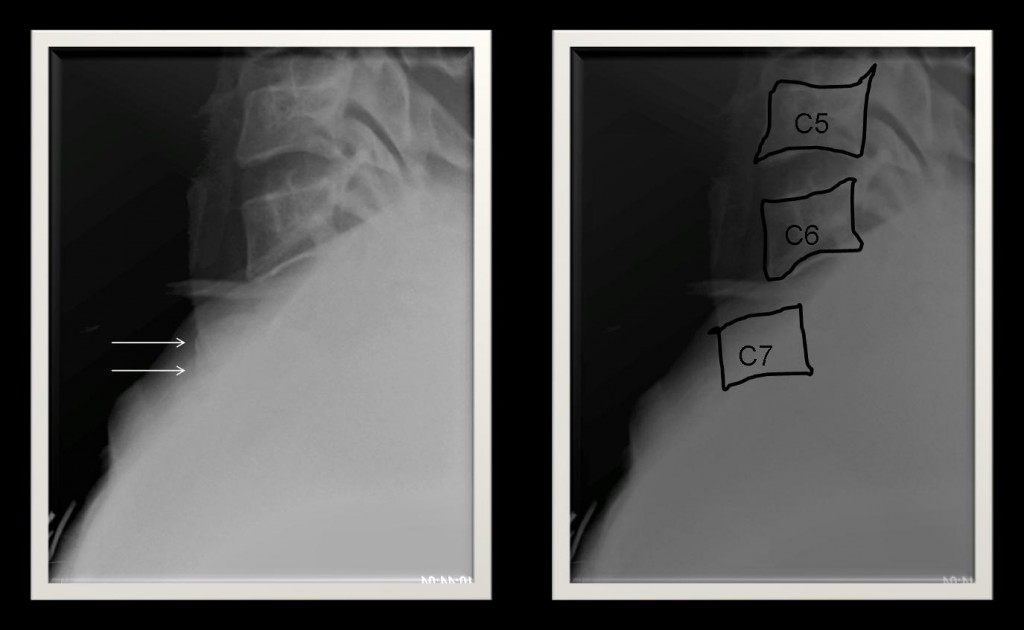
Fig. 2
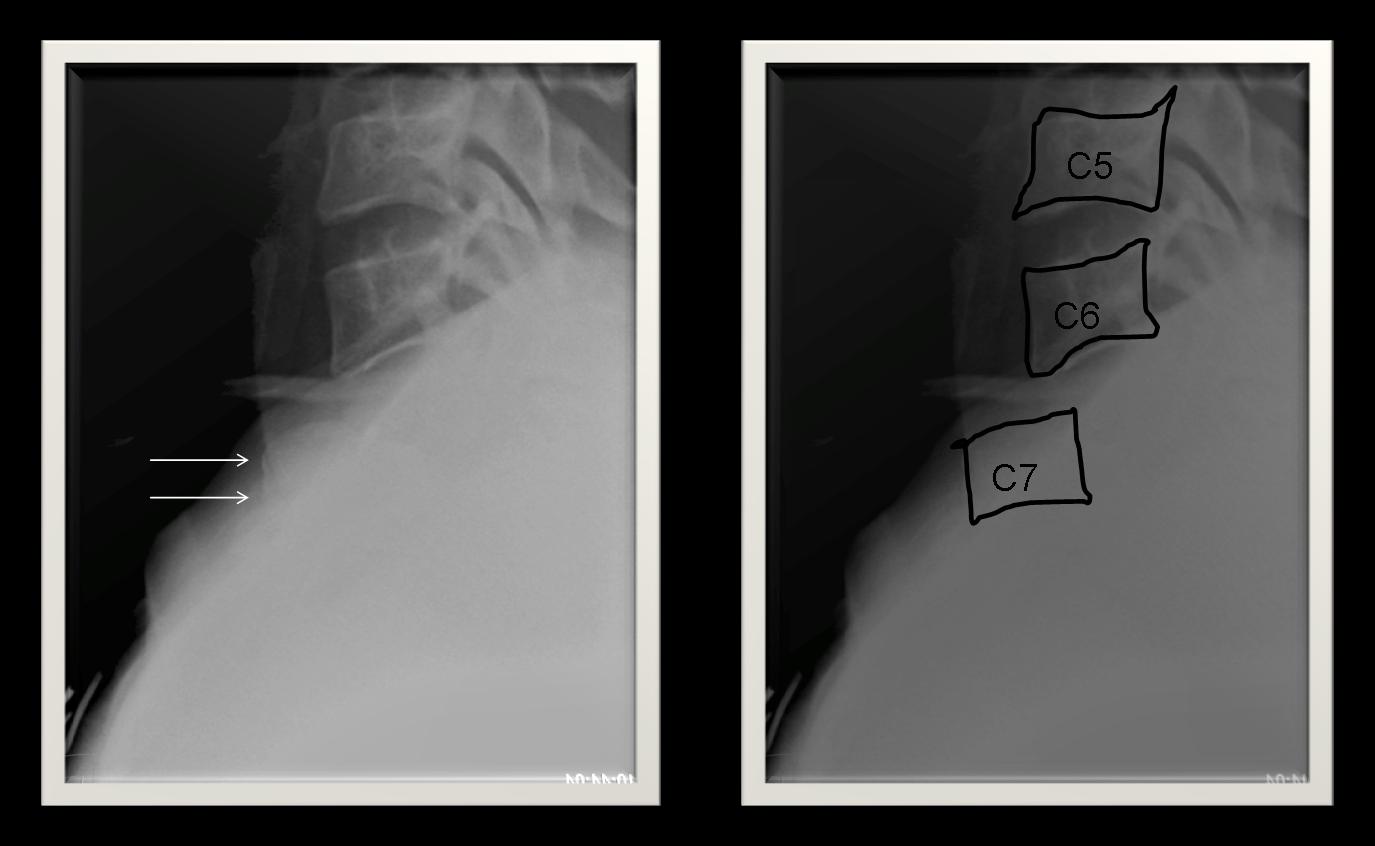
Fig. 2. With the use of halo traction, an increase in malalignment with greater C6-C7 displacement is observed (arrows). Halo traction was removed based on the signs suggesting hyperextension injury. The patient underwent surgery shortly afterwards.
FINAL DIAGNOSIS: Hyperextension fracture – C6-C7 dislocation
Lower cervical spine hyperextension injuries are the result of varying degrees of backward bending, with the articular pillar serving as the fulcrum of motion.
The most common mechanisms are motor vehicle accidents and falls. The anterior disk space is typically widened, and there may be associated fracture- dislocation of the facet joints and pedicles.
Other findings include
– anterior subluxation with normal interlaminar or interspinous spaces.
– normal spinolaminar line.
Cervical spine hyperflexion injuries are the most common injuries to the spine (50%-60%).
They result from varying degrees of forward bending with the posterior third of the intervertebral disc space as the fulcrum.
They produce narrowing of the anterior disk space and distraction of the posterior ligament complex and posterior disk space (Fig. 3).
Other findings include
– anterior subluxation with widened interlaminar or interspinous spaces.
– abnormal spinolaminar line.
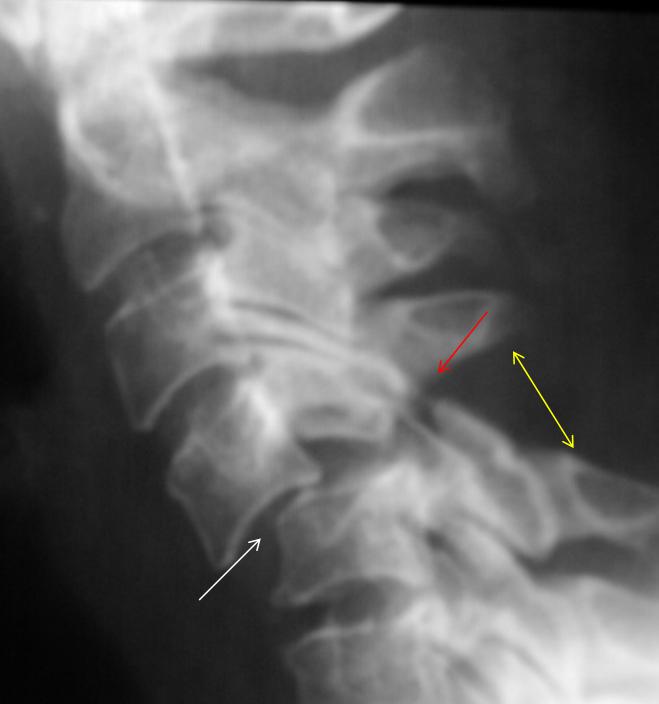
Fig. 3
Fig. 3. Hyperflexion injury. Lateral view of cervical spine shows forward displacement of C4 over C5 with anterior narrowing of C4-C5 disc space (white arrow).
There is widening of the facet joints with bilateral interfacetal dislocation and locked facets (red arrow), as well as widening of the interspinous and interlaminar spaces (yellow arrow).
Lower cervical burst fracture is caused by a mechanism of vertical compression.
Findings include
– vertical fracture line that extends through the height of the affected vertebral body
– disruption of both the superior and inferior endplates
– vertebral body comminution with retropulsion of its posterior fragments
– no signs of distraction of the posterior elements
– unilateral or bilateral laminar fracture.
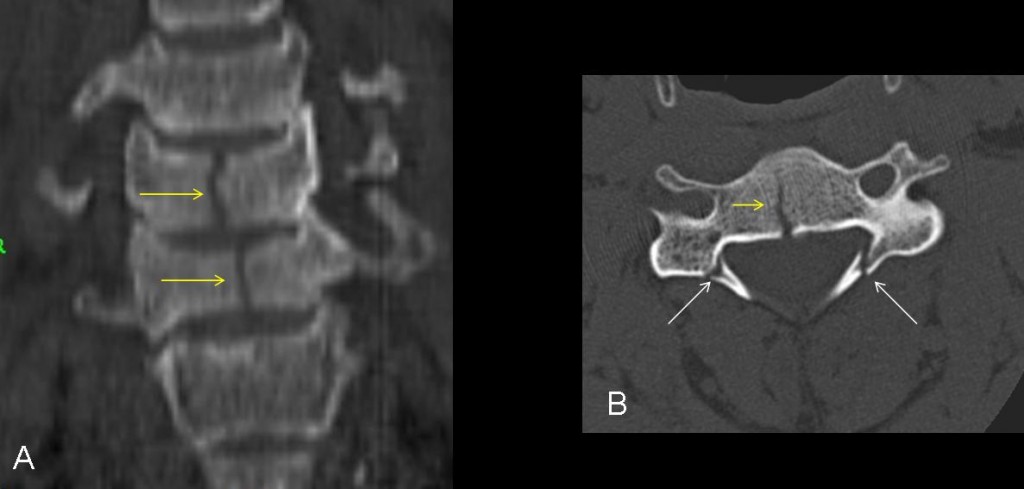
Fig. 4
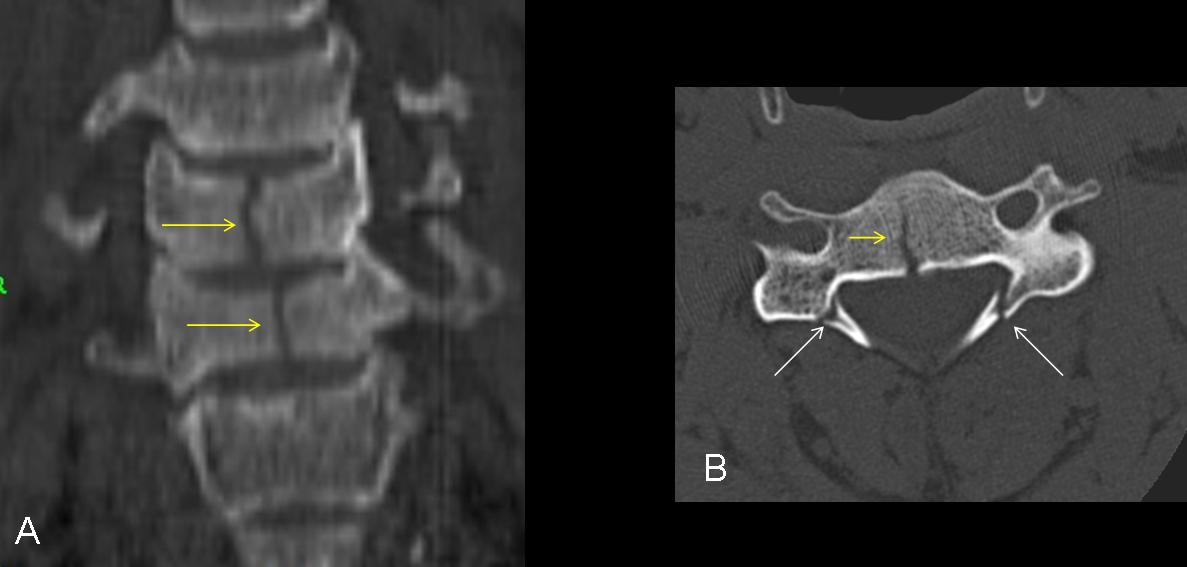
Fig. 4. Burst fracture of the lower cervical spine. (A) Sagittal CT shows a vertical fracture line that extends through the height of the affected vertebral bodies with disruption of the superior and inferior endplates (yellow arrows). (B) Axial CT shows the linear vertebral body fracture and bilateral laminar fractures (arrows).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Hyperextension injury usually opens the anterior disc space.
- Hyperflexion injury usually decreases the anterior disc space.
- In hyperextension lesions, the interlaminar line and interspinous space are preserved, whereas in hyperflexion lesions, there is posterior disruption with diastasis of the posterior elements.
Recommended reading: Imaging Evaluation of Adult Spinal Injuries: Emphasis on Multidetector CT in Cervical Spine Trauma. Radiology 2012;263(3): 645-660.
Case prepared by Lourdes Casas, MD



Locked facets
we don’t see C7. repeat of the x-ray?
None of the above.
Would you care to give a diagnosis?
1. Flexion injury (Consistant with hitting the ground with force while prone) – compressed C7 and luxated facets of C5/6
Chance fracture due to hyperflexion
C6 psterior elemnts disruption due to hyperflexion
Although the C7 is not adequate visible, we can see a widening of the intervertebral space on C6-C7 anteriorly but not posteriorly. There is misalignment of the CS column at both anterior and posterior vertebral line. There is not obvious fracture in the posterior elements of the vertebrae. Hyperextension injury at the level C6-C7.
Vi è un chiaro non-allineamento della linea vertebrale “anteriore” a livello di C7; vi è inoltre un aumento dello spessore dei tessuti molli prevertebrali a tale livello ( superiore ad un corpo vertebrale).La radiografia è inoltre incompleta perchè essa, in caso di trauma , deve comprendere anche la giunzione C7-D1.Quindi lesione ligamentosa e-o tramatica a questo livello , da definire con tac.Ricordarsi dell’acronimo: AABDT(Adeguata rx-Allineati bordi ossei-Disco-Tessuti molli prevertebrali).
e vero.
Hyperextension injury at the C6, posterior CS columnq processus spinosus
flexion lesion.fractura lamine vert.C6 with anterior sublux.