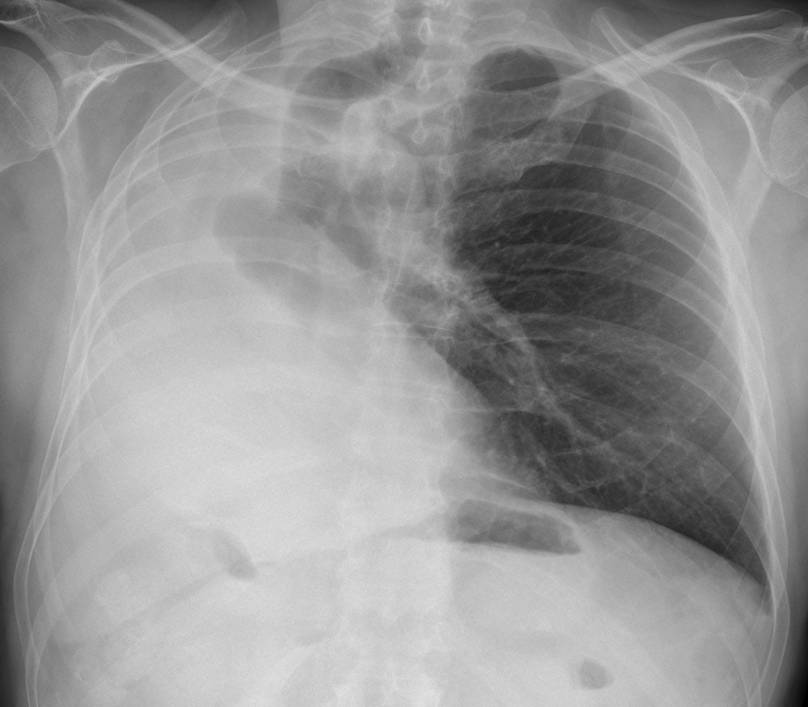
Showing you the last case before Summer vacation (July and August). Presenting radiographs of a 47-year-old man with moderate dyspnea.
1. Collapse of right lung
2. Right pneumonectomy
3. Congenital absence of right lung
4. None of the above
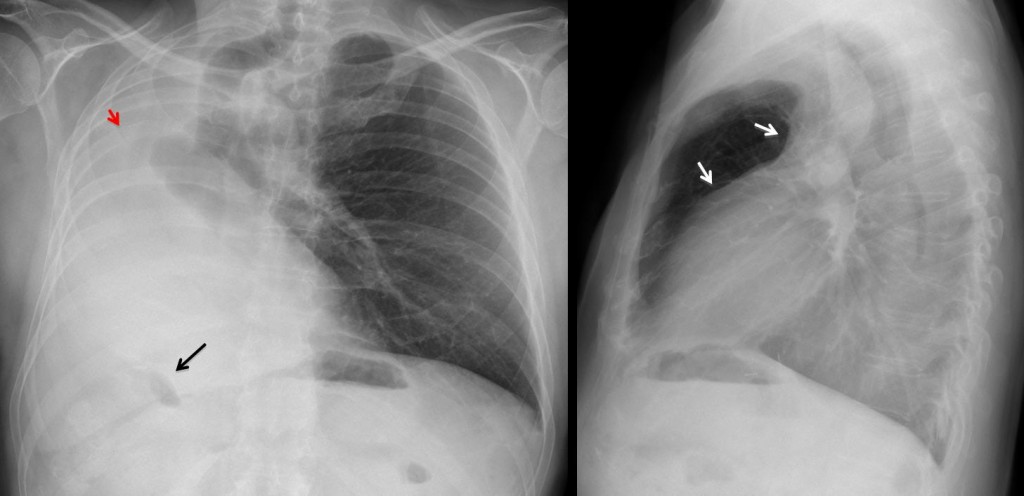
Fig. 1
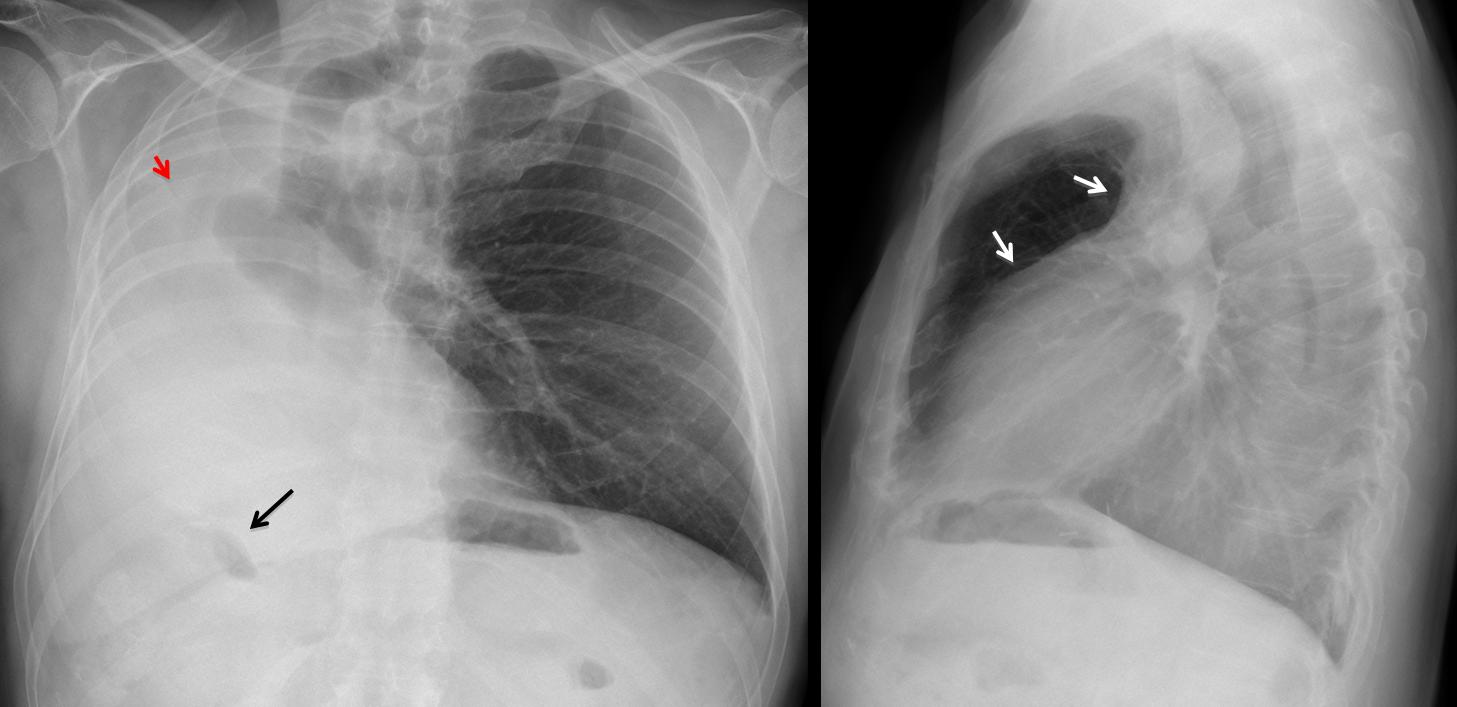
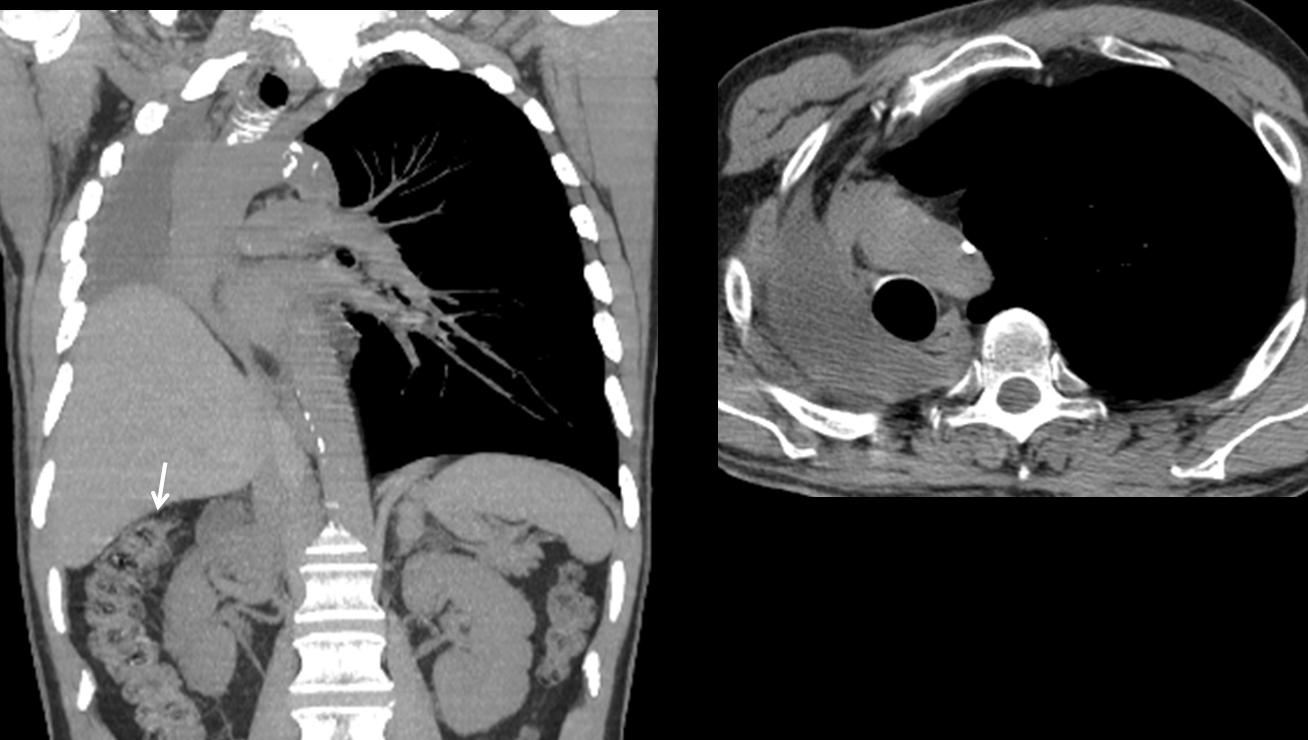
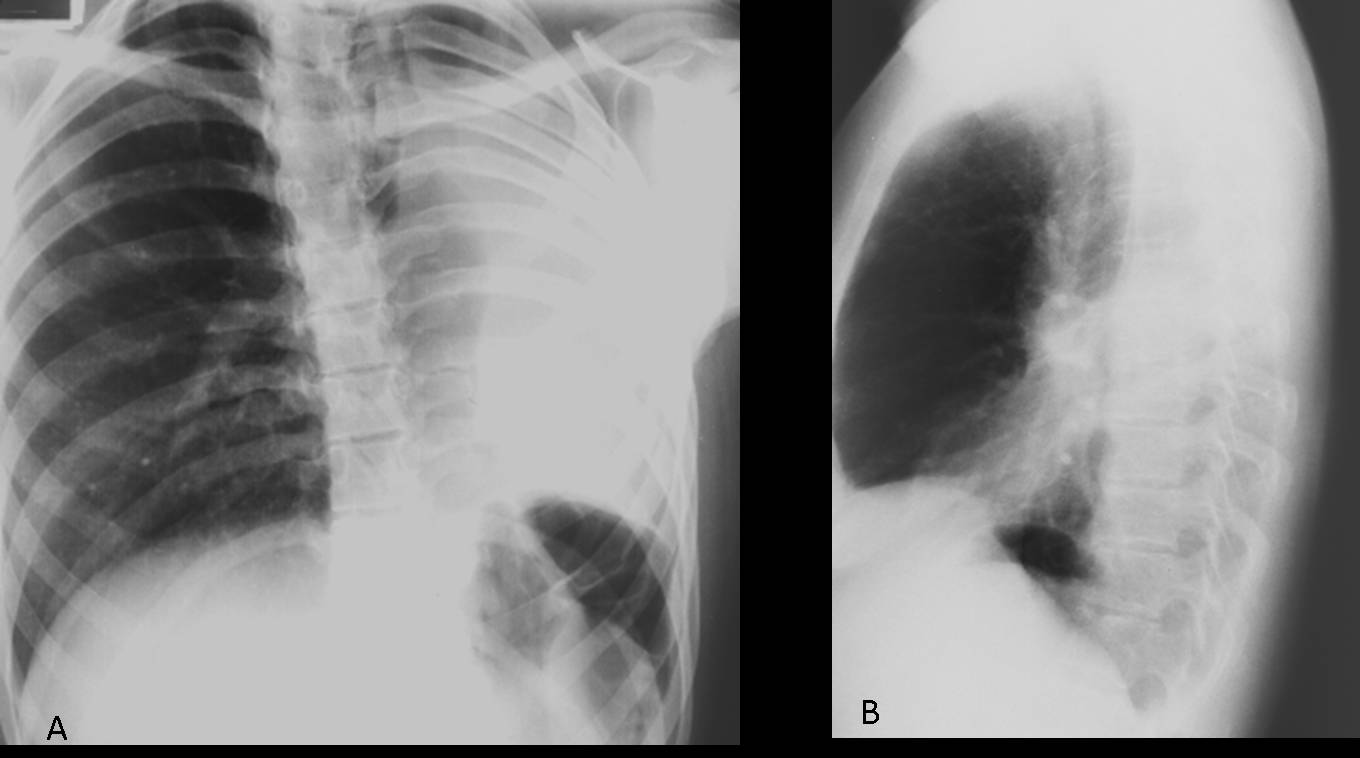
Findings: White hemithorax with marked shift of mediastinal structures. Elevation of right hemidiaphragm, indicated by the high position of the hepatic flexure of colon (arrow). Lateral view shows anterior herniation of opposite lung (arrows). All these findings indicate a considerable volume loss of right lung, which is consistent with all three diagnoses offered. However, in this particular case, the slight positional asymmetry of the sixth rib (red arrow) suggests a previous pneumonectomy.
CT shows the post-pneumonectomy space filled with pleural fluid, confirming the diagnosis. The liver partially occupies the right hemithorax. Note the marked elevation of the hepatic flexure (arrow).

Fig. 2
Final diagnosis: right lung pneumonectomy
The differential diagnosis of a white hemithorax mainly includes lung collapse and massive pleural effusion. The diagnosis is easily established by determining the position of the mediastinal structures, among which the trachea is the easiest to visualize. Massive pleural effusion will displace the trachea towards the opposite side, whereas loss of lung volume will attract the trachea to the affected side.
Other signs of volume loss are diaphragmatic elevation, as signaled by air in the hepatic flexure or in the gastric fornix on the left side and varying degrees of anterior herniation in the lateral view.
Pneumonectomy is one of the most common causes of white hemithorax with volume loss. Aside from the clinical history, look for postoperative changes at the ribs and surgical clips.
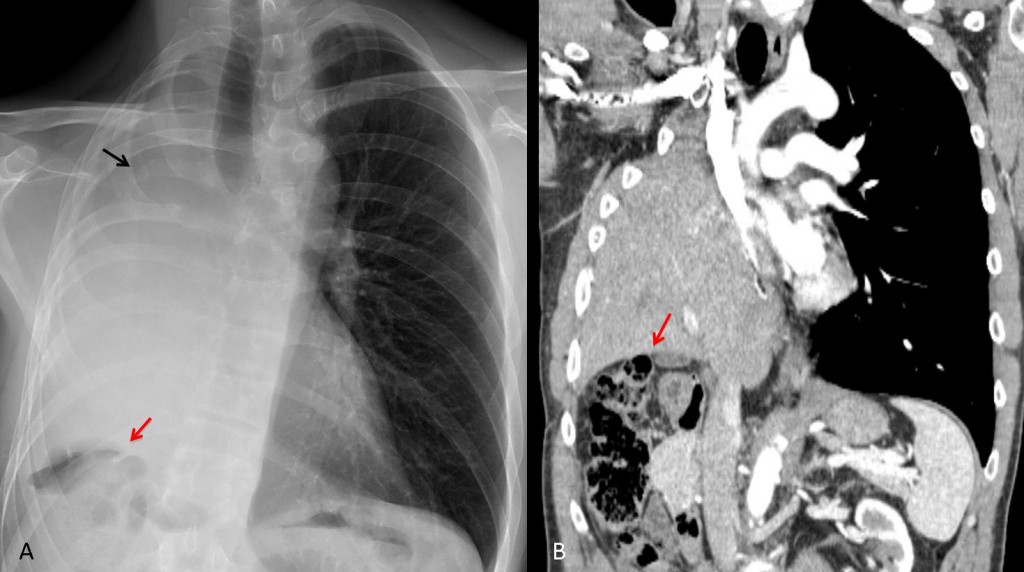
Fig. 3
Fig. 3. 54-year-old male after right pneumonectomy with diaphragm resection. The liver is herniated into the right hemithorax. Note the postoperative changes at the right sixth rib (A, black arrow) and the high position of the hepatic flexure (A, B, red arrows)
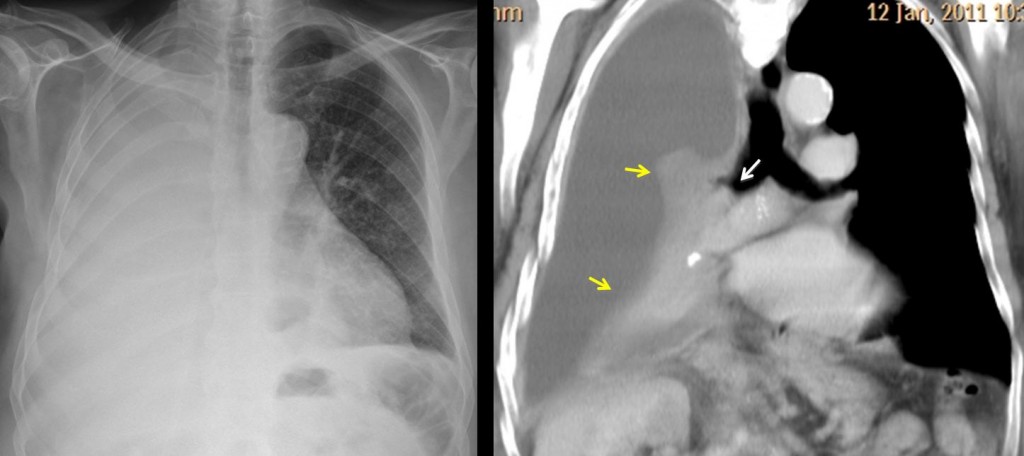
Fig. 4
Fig. 4. In patients who have not undergone surgery, carcinoma of the main bronchus with complete lung collapse is the most common cause of white hemithorax. Mediastinal shift is usually not very marked because the associated pleural effusion compensates for the volume loss. Thus, it is not unusual for the trachea to stay in the midline, as in this case.
CT shows the endobronchial tumour (white arrow), with lung collapse (yellow arrows) and associated pleural effusion.
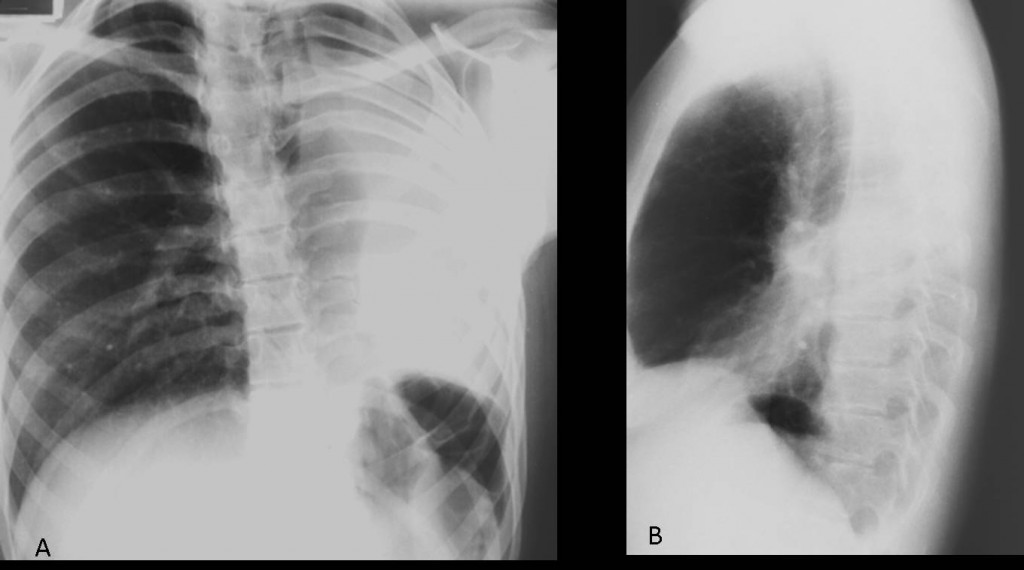
Fig. 5
Fig. 5. Congenital lung malformations are not uncommon findings in adults. Agenesis of one lung may affect either side. A small airless hemithorax is seen, with crowding of the ribs and herniation of the contralateral lung across the anterior clear space (A,B arrows).
In an asymptomatic patient with no previous surgery, these features should suggest agenesis of the lung.
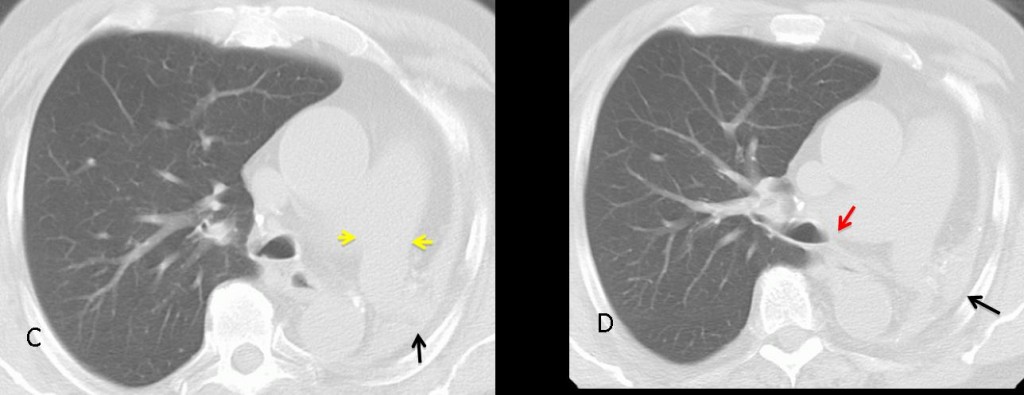
Fig. 6
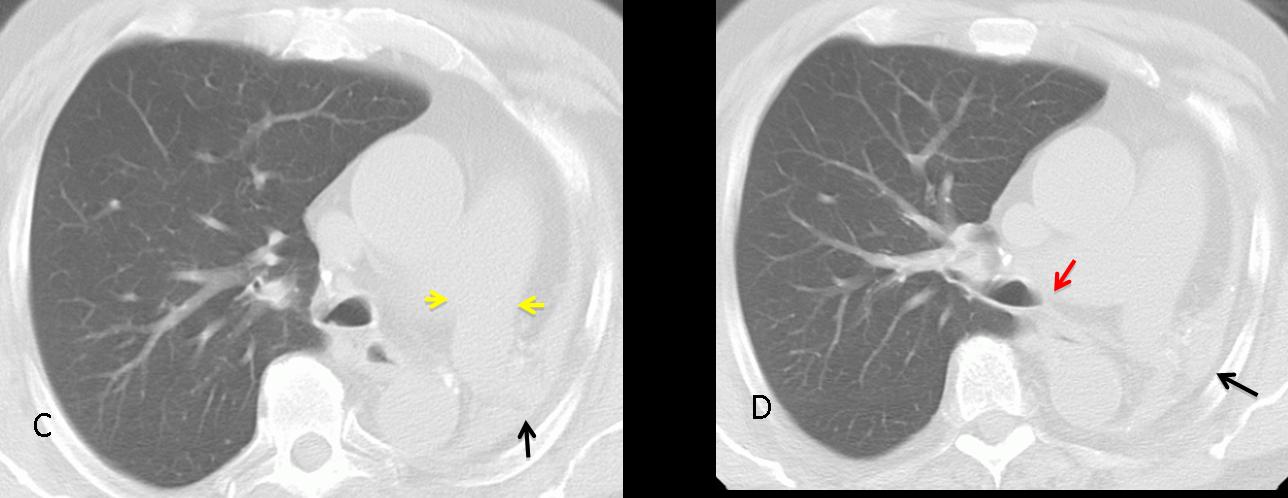
Fig. 6. CT shows a small remnant of hepatized lung tissue (C,D back arrows). The left main bronchus is absent (D, red arrow), although the homolateral pulmonary artery is usually of normal size (C, yellow arrows). Note the herniation of the right lung behind the sternum.
Most patients are asymptomatic and no treatment is necessary. Surgical resection is indicated for the few patients with lung remnants and recurrent infection.

Follow Dr. Pepe’s advice:
- A white hemithorax with mediastinal shift towards the affected side suggests a central carcinoma with secondary collapse or a previous pneumonectomy.
- If no clinical information is available, look for postoperative changes at the ribs and surgical clips.
- In an asymptomatic patient with no previous surgery, consider congenital agenesis of one lung.
Case prepared by Dr. Pepe





Left lung herniation. Signs of decreased volume in the right hemithorax.
Dx – collapsed right lung.
Rt. Lung Collapse
Colapso pulmonar derecho
CONG:ABSCENT RT LUNG
I agree.
#3
Congenital absence of right lung- opacity of the right hemithorax and displacement of the heart and mediastinum to the right. Also we find the tracheal displacement to the right and a congenital anomaly of the right principal bronchi.
Right pneumnectomy
Atelettasia polmone dx , da adenoma bronchiale( sino a prova contraria)
The PA view shows complete opacification of the right hemithorax with shifting of the trachea, mediastinum and cardiac silhouette to the right. Lateral view shows a widened retrosternal space corresponding to displacement of the heart. The right main stem bronchus appears to be both lobulated and truncated possibly representing a rudimentary bronchus. Therefore, this seems to be a case of aplasia of the right lung rather than complete agenesis.
rt pneumonectomy
Right Lung collapse
1. Collapse of the right lung (maybe post-surgical because I see surgical clips in the right upper quadrant)
Rt.lung collapse
Trachea is push out back on the right.
I cant see the right hilum on profile view.
The ribs looks intact on the right.
Moderate dyspnea in right pulmonary collapse?
I think is chronic situation.
Collapse of Rt lung
right lung collapse
Collapse of right lung
I am surprised nobody has mentioned the surgical clips in the lateral view!
But the clips professor is sub diaphragmatic .
Patient had operate for diaphragmatic rupture or tumor?
You are right. Clips are a red herring. Patient had a common operation.
Right pneumonectomy.
.. la DD con un emitorace “opaco”, comprende anche l’agenesia polmonare.Il paziente è stato operato in passato all’addome e sarebbe interessante sapere il precedente rx-torace pre-operatorio;.se anche in quella circostanza si evidenziava lo stesso quadro, allora è lecito pensare ad una agenesia polmonare di IItipo sec.Schneider: presenza di un bronco dx “rudimentale” con sacca area distale(come nel caso in oggetto)