Dr. Pepe’s Diploma Casebook: Case 47 – SOLVED!
Dear Friends,
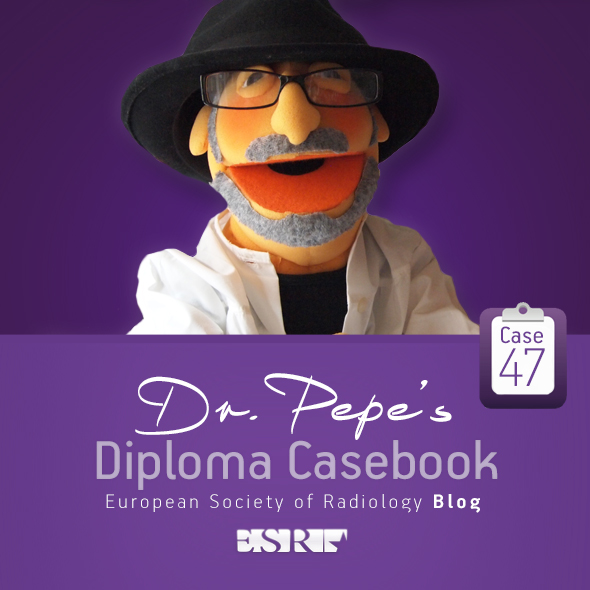
Today I’m showing a vintage case, seen thirty years ago when I was a promising young staffer. The images below belong to a 57-year-old missionary living in Africa and undergoing yearly controls at our institution for unilateral hyperlucent lung.
Leave me your thoughts and diagnosis in the comments section and come back on Friday for the solution.
Diagnosis:
1. Swyer-James/Macleod syndrome
2. Bronchial tumour
3. Pulmonary artery stenosis
4. None of the above

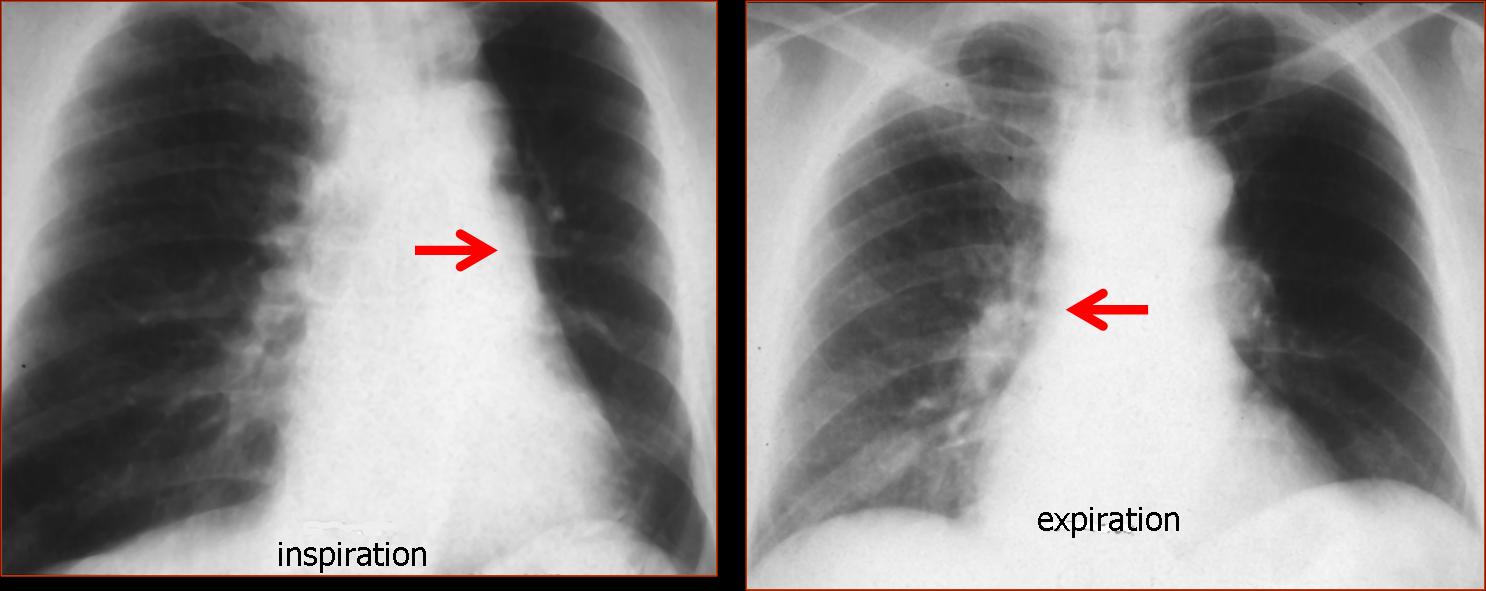
Fig. 1
Lateral view shows a tracheal mass (A, arrows), better seen in the tomogram (B, arrows) and the axial CT (C, arrow). The mass partially obstructed the origin of the left main bronchus; hence, the air-trapping.
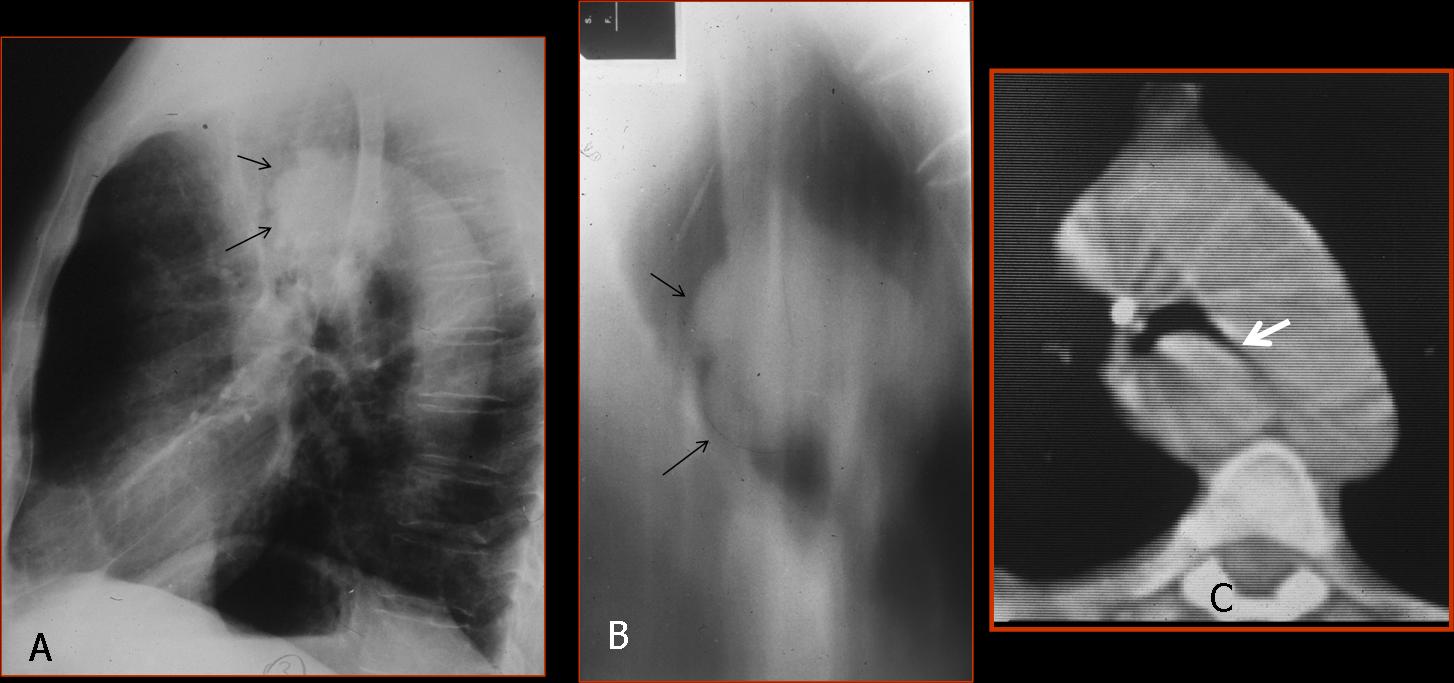
Fig. 2
Final diagnosis: adenoid cystic carcinoma of the trachea and left main bronchus.
This case is a good example of the so-called unilateral hyperlucent lung (UHL), a radiological finding of increased darkness of one lung with or without decreased vascularisation. Unilateral hyperlucent lung is discovered in the PA chest radiograph. The lateral view helps to identify ancillary findings, as in the present case.
The causes of UHL can be classified as follows:
1. Increased lung air
2. Decreased pulmonary vascularity
3. Pneumothorax
4. Chest wall abnormalities
5. Technical factors
In UHL caused by increased lung air, the initial approach is to separate obstructive from non-obstructive causes. This is easily accomplished with inspiratory and expiratory films, which will demonstrate air–trapping in the obstructive cases.
The most common cause of obstructive UHL is an endobronchial lesion causing partial obstruction of the main bronchus with resultant air-trapping. The main offenders are tumours, as in the present case, and foreign bodies in children (Fig. 3).
Fig. 3
Fig. 3 (above): foreign body aspiration in a 5-year-old child with dyspnea. Inspiration film looks normal; expiration demonstrates trapping of air in the right lung, with mediastinal shift towards the left. Bronchoscopy demonstrated an aspirated peanut in the right main bronchus.
Inspiration/expiration films are of value for identifying which lung is affected. The inspiration film in the case below (Fig. 4) shows a hyperlucent right lung, making it suspect of disease. On expiration, however, the right lung empties, whereas the left lung remains the same, indicating air-trapping on the left.
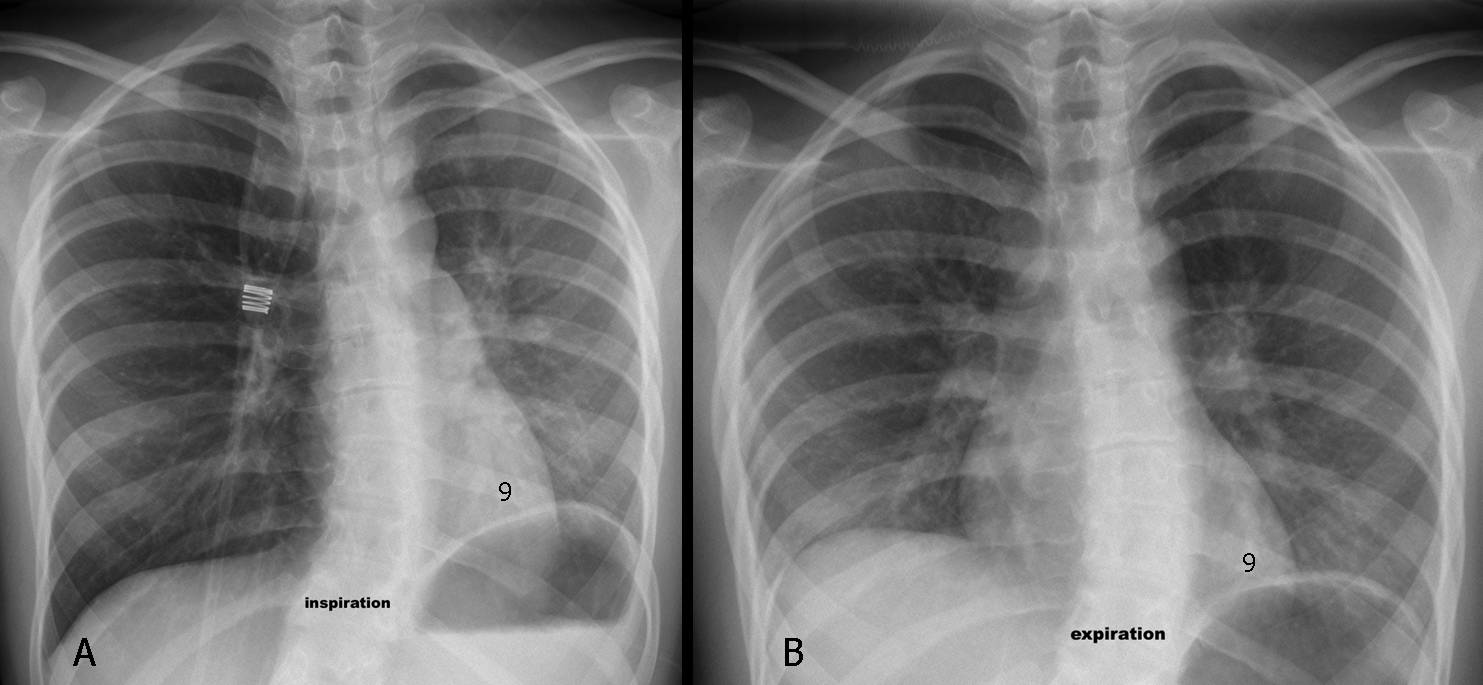
Fig. 4 (above): a 17-year-old girl with asthma and severe dyspnea. Inspiration/expiration films (A,B) show obvious air-trapping of the left lung. Notice that the left hemidiaphragm is always at the level of the 9th rib. Sagittal CT (Fig. 5, below) shows inspissated mucus in the left main bronchus (A, arrows) as the cause of the symptoms. After the mucus cleared, the chest returned to normal (B).
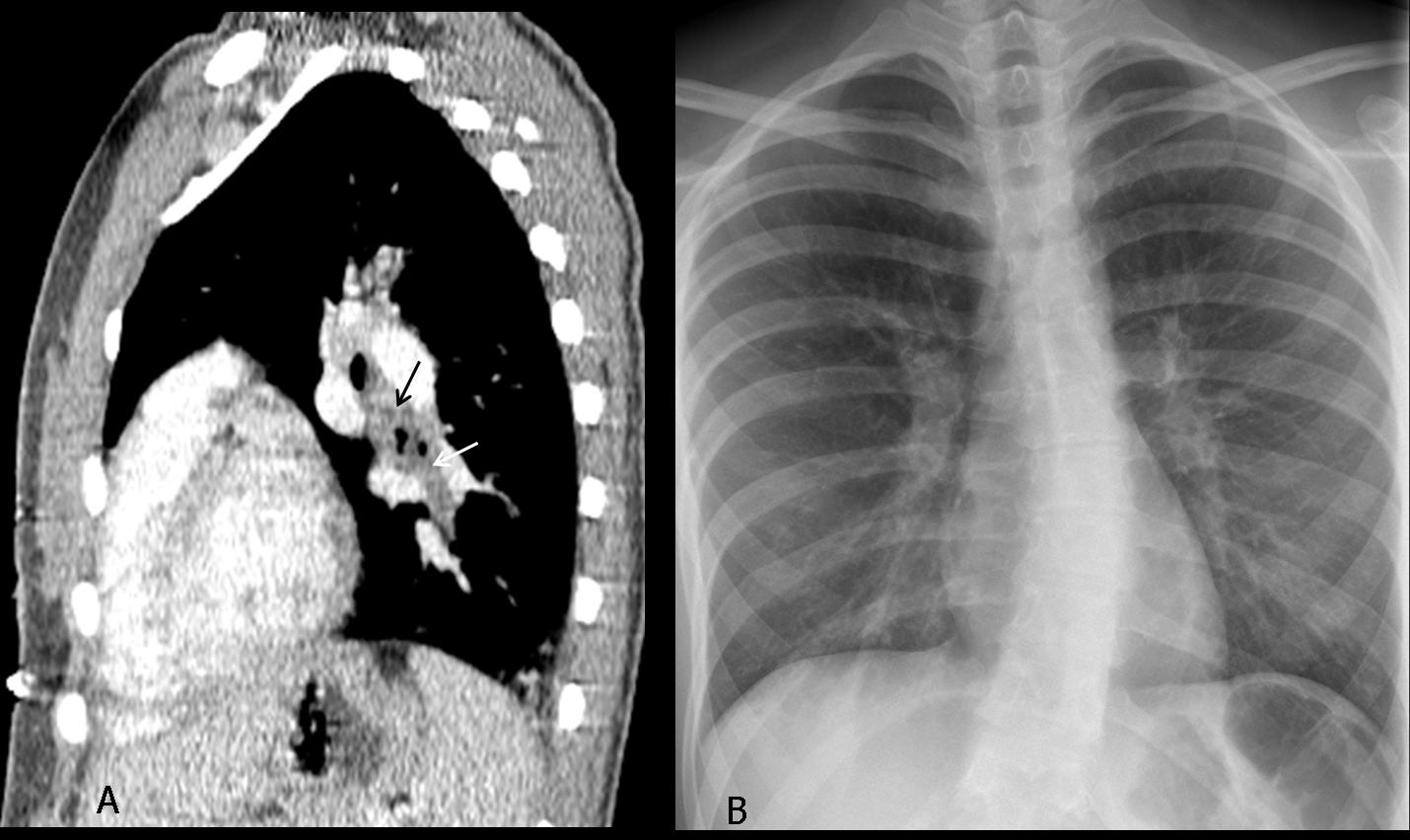
Fig. 5
Swyer-James/McLeod syndrome is a well-recognised, but uncommon, cause of obstructive UHL. In these patients, the main bronchi are permeable and the air-trapping is secondary to peripheral bronchiolitis after viral infection in childhood. Personally, I have seen very few cases of this syndrome in adults (Fig. 6).
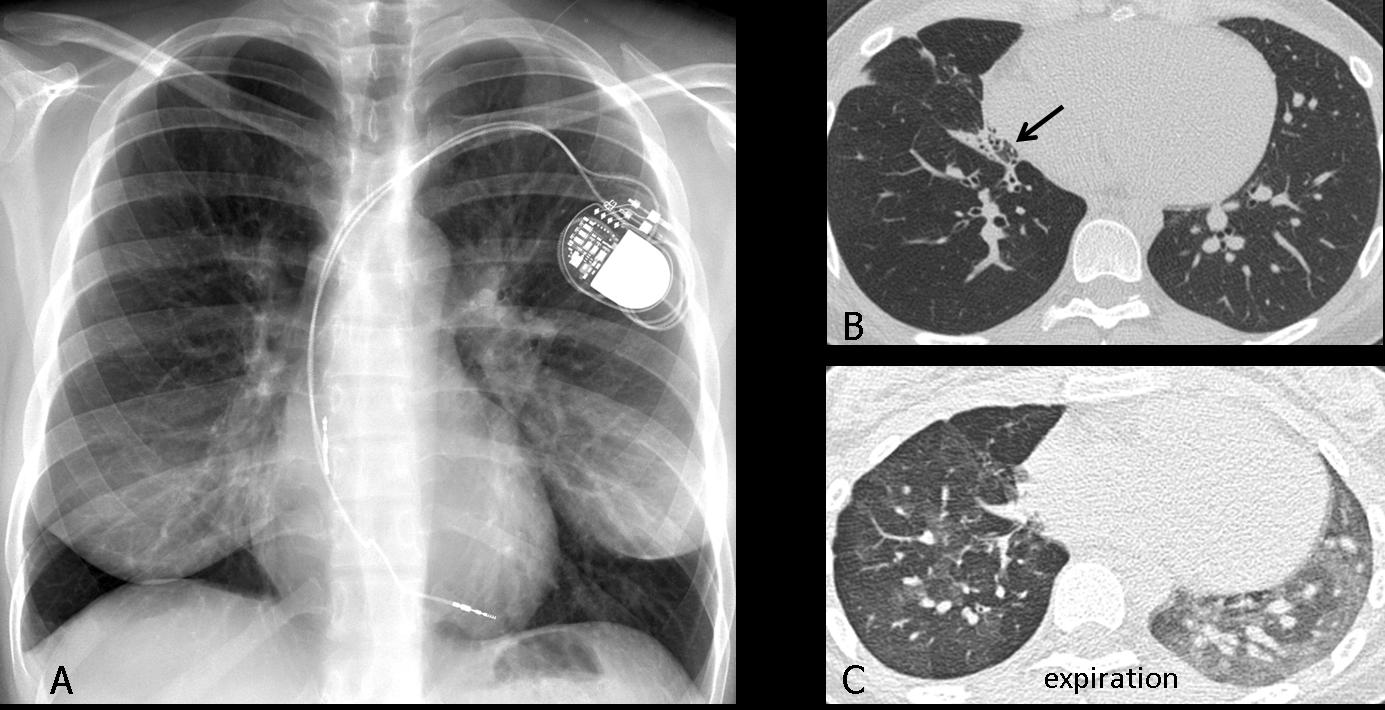
Fig. 6
Fig 6 (above): 47-year-old woman with Macleod syndrome. PA film shows a hyperlucent right lung with decreased vascularity (A). CT images show decreased vascularisation and bronchiectasis (B, arrows). Expiration CT shows air-trapping (C).
Non-obstructive UHL is due to compensatory overinflation secondary to a collapsed lobe or previous lobectomy. Obviously, the expanded lung empties well and does not trap air on expiration. Signs of collapse are usually obvious; if they are not, they should be sought to avoid making an erroneous diagnosis (Fig. 7).
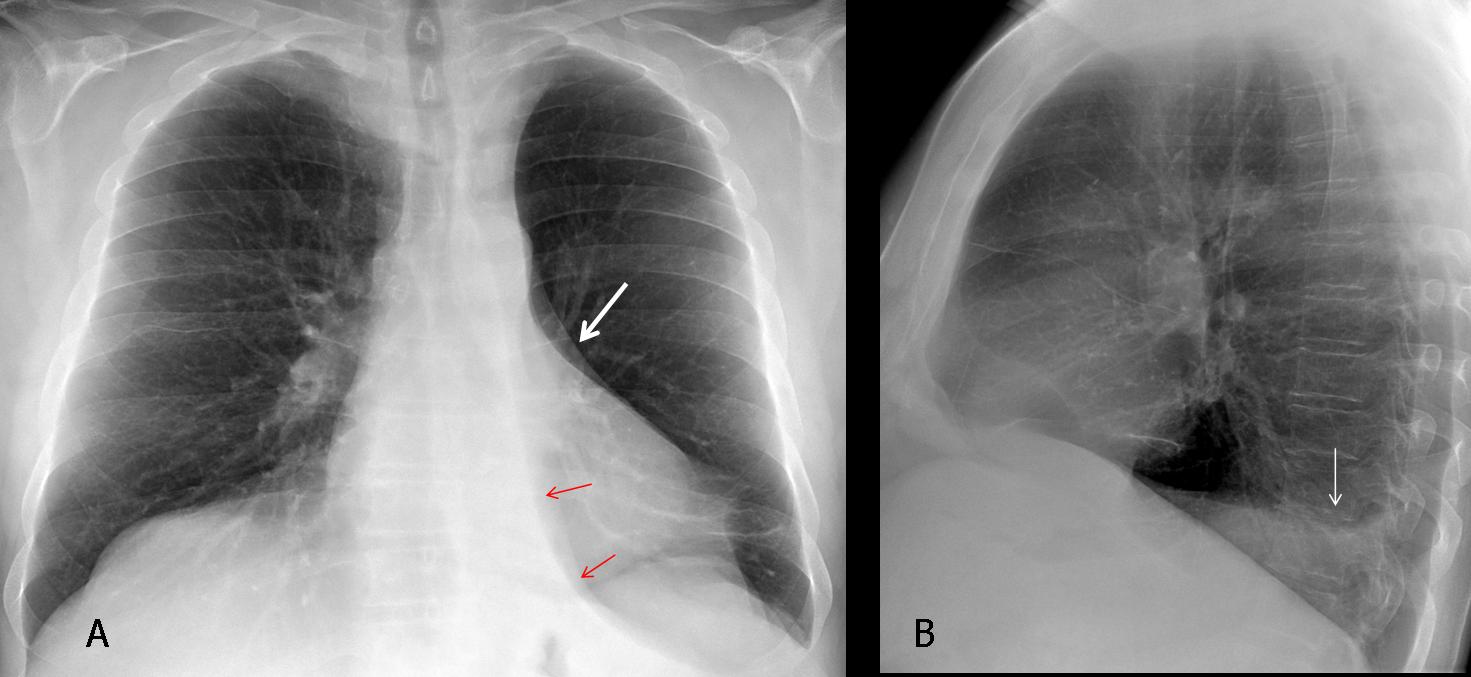
Fig. 7
Fig. 7 (above): 67-year-old man with moderate cough. PA radiograph shows what appears to be a left hyperlucent lung. Close observation shows a markedly descended hilum ( A, white arrow) and a triangular shadow (A, red arrows), which represents the collapsed LLL. The lateral view shows obliteration of the posterior hemidiaphragm by the collapsed lobe (B, arrow).
Axial CT demonstrates the marked LLL collapse (C, arrow), secondary to an endobronchial lesion at the origin of the LLL bronchus (D, arrow). Diagnosis: bronchogenic carcinoma.
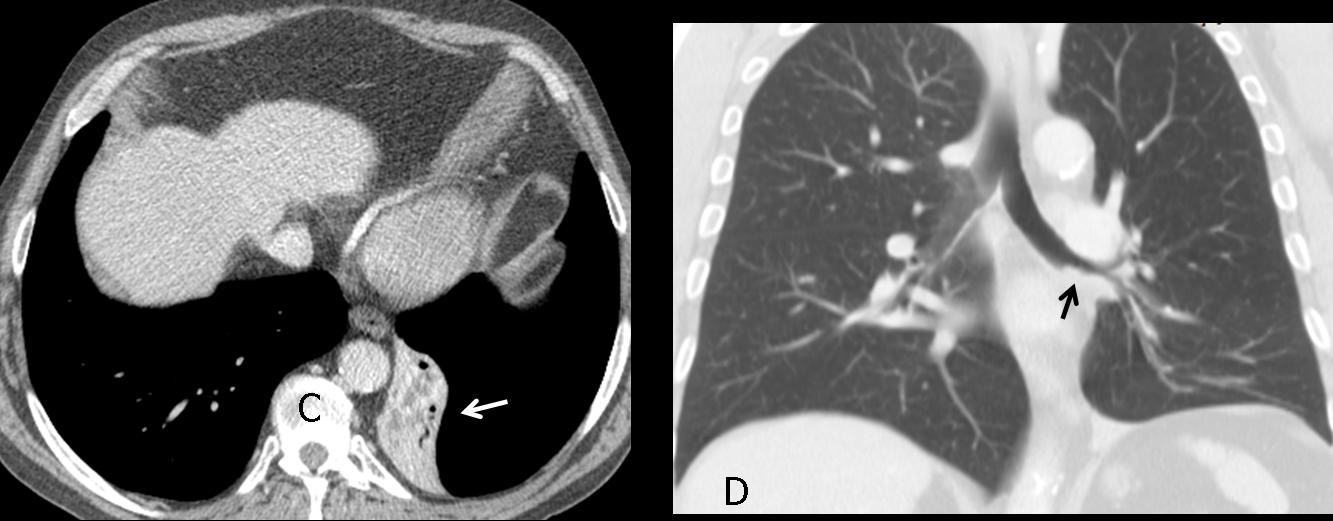
Fig. 8
Time for a test. These radiographs belong to a 23-year-old diabetic male with acute dyspnea. What would your diagnosis be?
1. Pneumothorax
2. Pulmonary embolism
3. Central carcinoid
4. None of the above
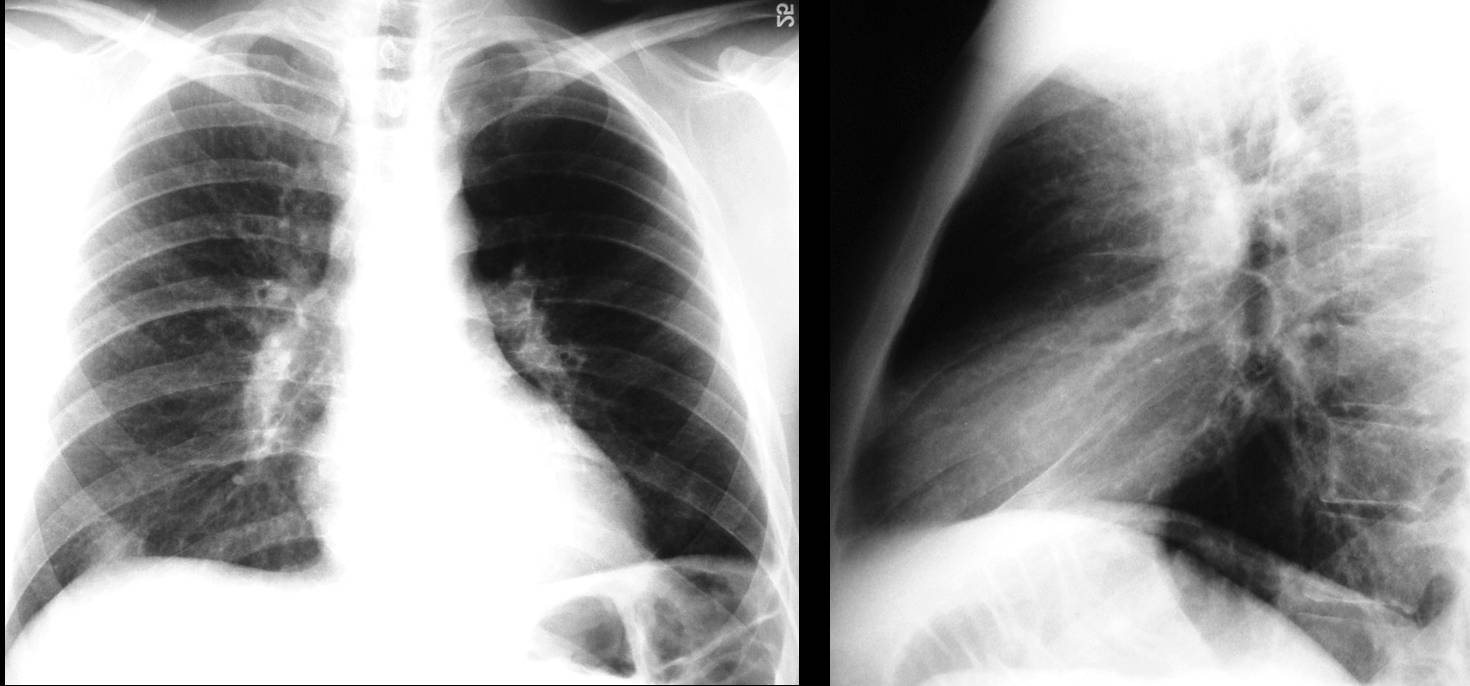
Fig. 9
This is a case of UHL secondary to decreased vascularity. The pulmonary artery and its branches contribute to the opacity of the lungs, and any cause of unilateral decreased pulmonary vascularity (arterial stenosis, pulmonary embolism) will appear to the eye as unilateral hyperlucent lung (Fig. 10). Of course, expiration films will not demonstrate air-trapping.
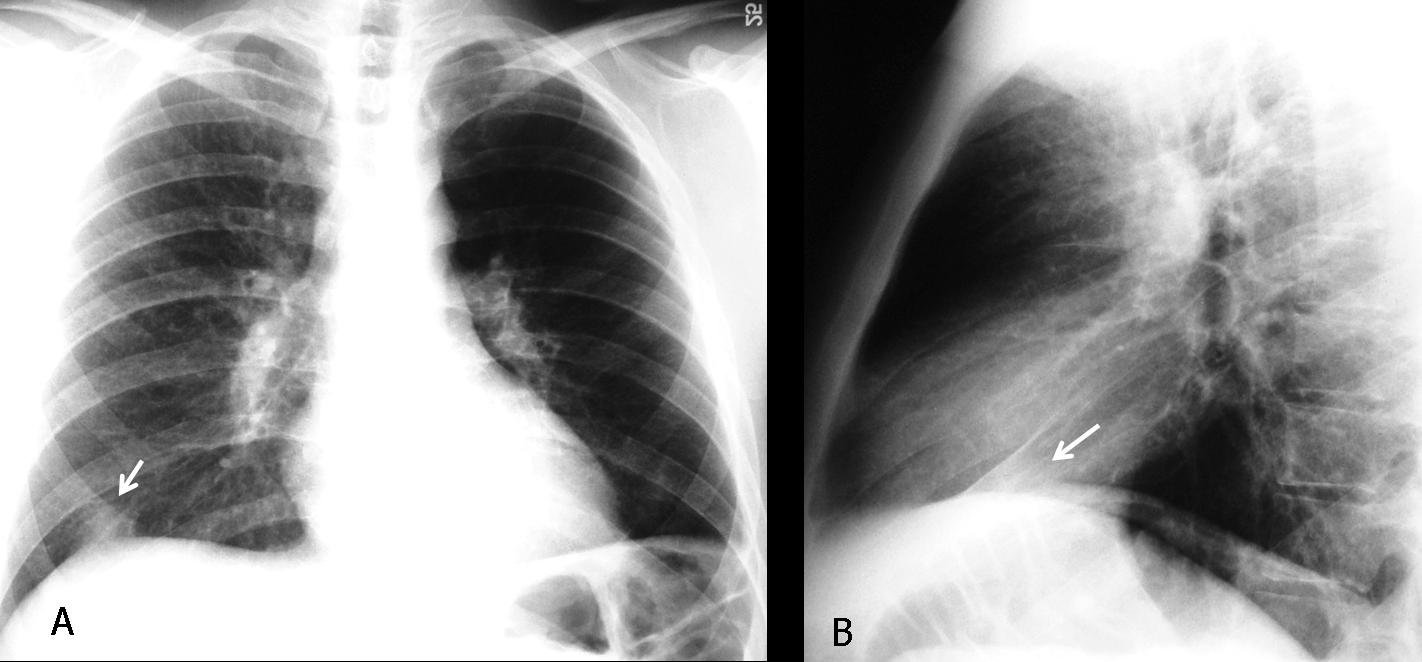
Fig. 10
Fig. 10 (above), findings: hyperlucent left lung with markedly decreased vascularity. There is a pleural-based opacity at the right lung base (A,B, arrows) whose morphology suggests a Hampton hump. CT (Fig. 11, below) confirms bilateral pulmonary emboli (A, arrows) and the typical shape of a pleural-based infarct (B, arrow).
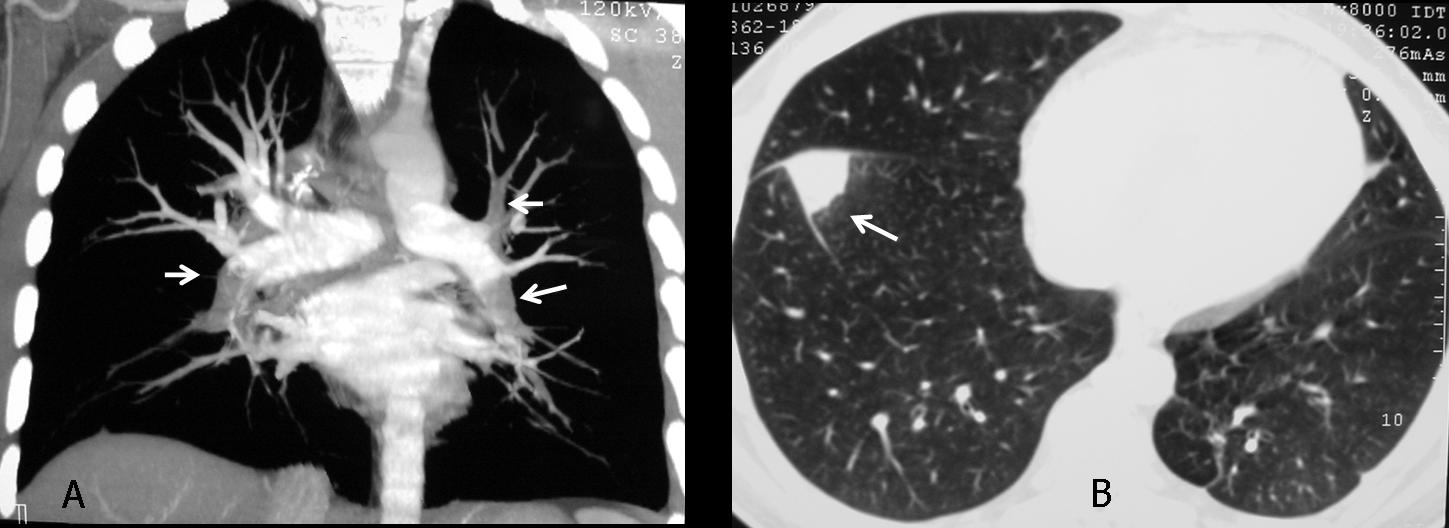
Fig. 11
Pneumothorax is a common cause of hyperlucent lung. The signs of a large pneumothorax are evident and the diagnosis is difficult to miss. The affected hemithorax is hyperlucent, and the collapsed lung appears as a stump in the parahilar area (Fig. 12 A, arrow). In another patient (B), tension pneumothorax is pushing the mediastinal structures towards the opposite side, hiding the pulmonary stump. Note in this case the telltale V sign, typical of pneumothorax (B, arrows).
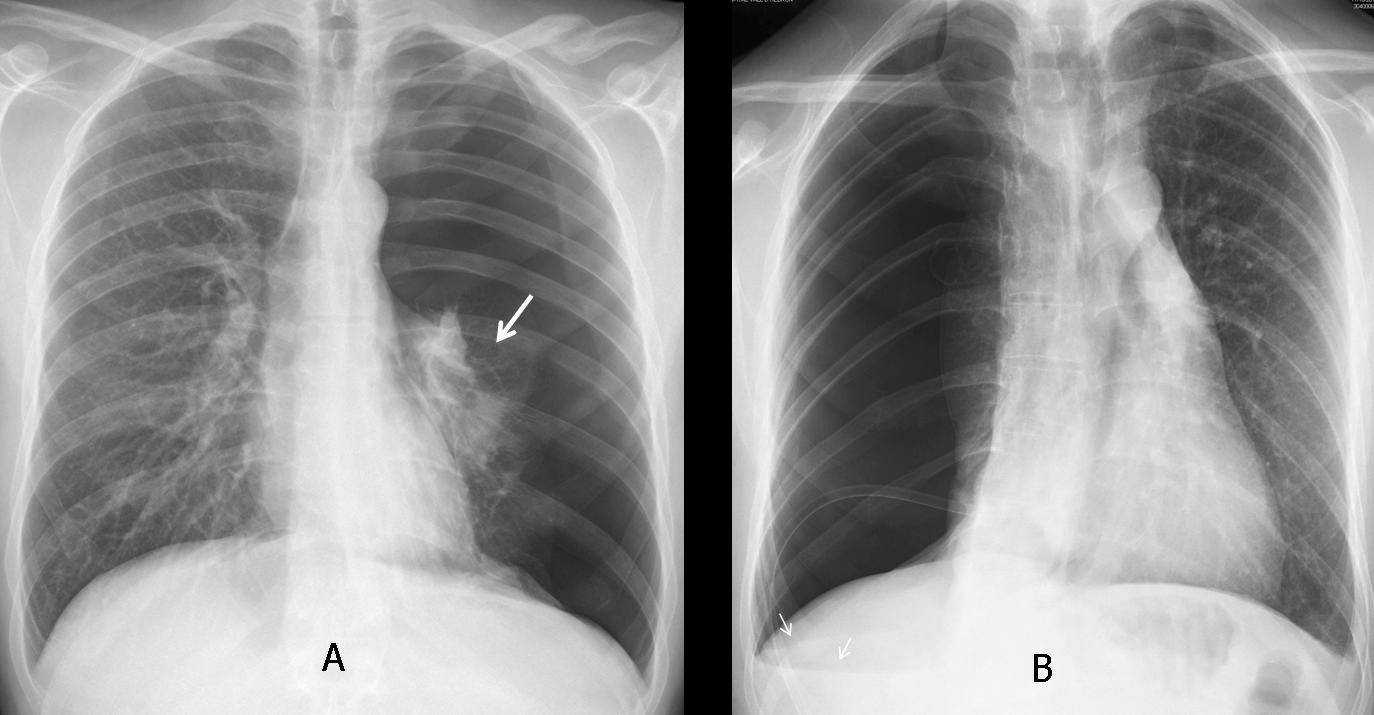
Fig. 12
Chest wall abnormalities, such as mastectomy or the rare congenital absence of the pectoralis major muscle (Poland syndrome), are responsible for increased unilateral lung lucency by decreasing the thickness of the superimposed soft tissues.
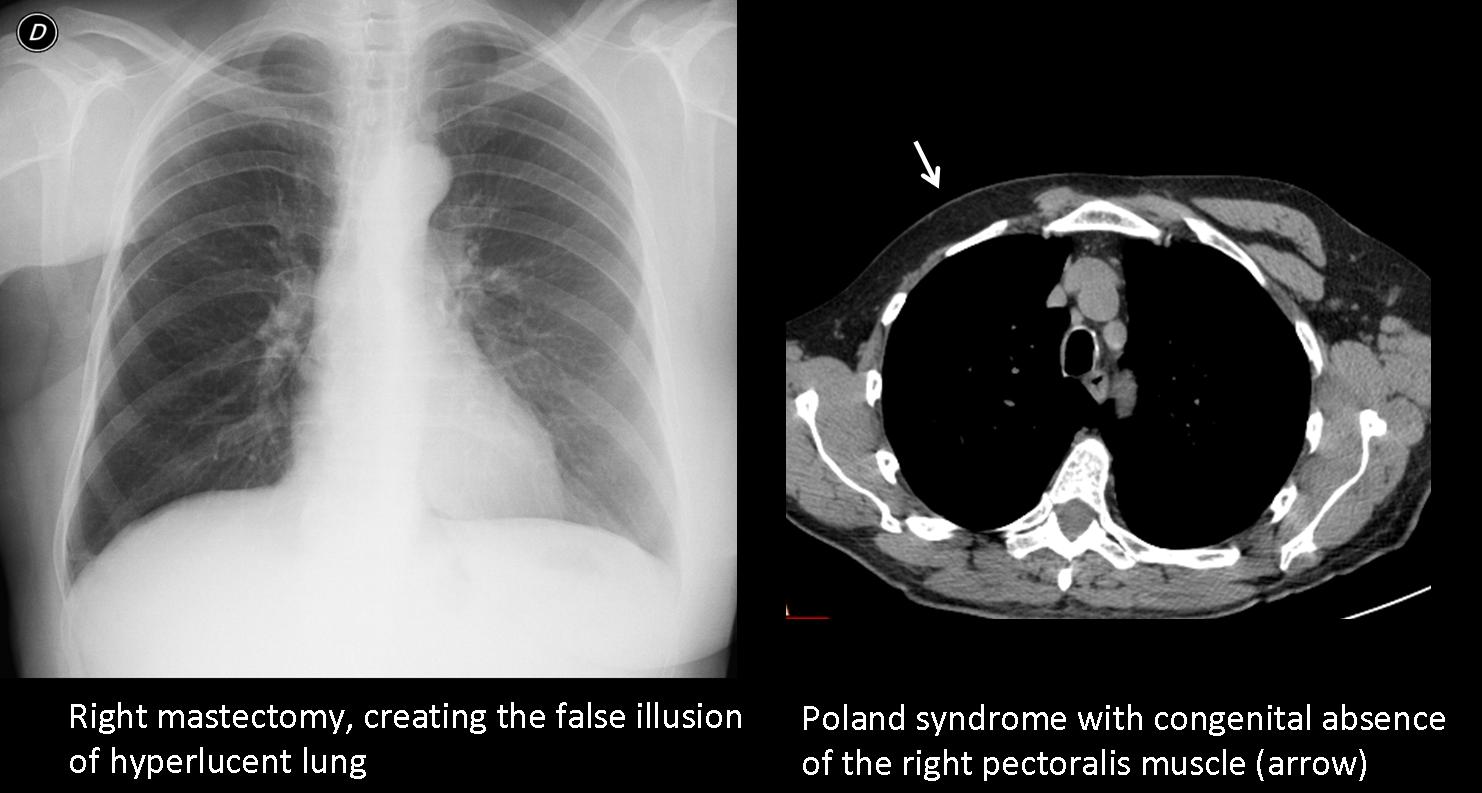
Fig. 13
Last, but not least, technical factors such as slight oblique positioning of the patient and/or a mis-centered x-ray beam can cause spurious increased unilateral lucency of one lung. In my experience, this is probably the most common cause of UHL and should be excluded before engaging in a more detailed investigation.

Fig. 14
Fig. 14 (above): two patients with hyperlucent left lung due to a miscentered x-ray beam. In A, note how the soft tissues of the shoulder are also darker, suggesting unequal penetration of the x-ray beam.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Obstructive UHL is caused by endobronchial lesions or, rarely, by peripheral bronchiolitis.
- To investigate obstructive UHL, inspiratory/expiratory films are mandatory.
- Other pulmonary causes include compensatory overinflation and decreased pulmonary vascularisation.
- The most common causes of UHL are technical factors, mastectomy, and pneumothorax.


In inspirazione vi è lievissimo shift cardiomediastinico a sx, mentre in espirazione vi è air-trapping del polmone sx; la “vecchia” broncografia dimostra una ipoplasia del bronco principale di sx.Quindi escludiamo la S.diSJ-mc Leod che è una conseguenza di bronchioliti , con ipoplasia vascolare; escludiamo la stenosi arteria polmonare, perché non dimostrata; escludiamo il CR bronchiale in relazione alla regolarità della stenosi bronchiale:rimane una ipoplasia polmonare bronchiale, con air-trapping da pori di Khon per le collaterali di areazione.
Wanishing-lung o Sindrome di Giano, dovuta ad ipoplasia arteria polmonare con conseguente rarefazione del disegno polmonare ed “air-trapping” attraverso i pori di Khon.
There is hyperlucent left lung with shifting of the mediastinum to the left side during inspiration. Huperlucent lung remains in the image during expiration. Pulmonary arteriogram shows no appearance of the LUL pulmonary artery and descending pulmonary artery is seen partially. Hyperlucent lung is due to diminished vascular blood flow. Because it is long term disease- patient ungergoes yearly controls- I vote for Swyer-James syndrome.
Hi, Prof. I hope that you are fine
I see in this case that there is hypoinflation of the left lung in the inspiratoty film with markedly attenuated its bronchovascular markings. In CT angio study, there is marked hypo-perfusion of the left lung in a symmetrical manner with relatively small left pulmonary branch in comparison to the right branch , this is consistent with Mcleod syndrome
sorry , not a CT angio, It is a conventional pulmonary angiography
Hello prof.
I will go here with Swyer-James /Macloed syndrom.
There is hypoinflation in the left lung with compensatory hyperinflation in the right lung as seen in the inspiratory film and air trapping in the left lung as seen in the expiratory film.which Is believed to be a sequale to old bronchiolitis.
And there is left pulmonary artery hypoplasia as shown in the conventional pulmonary angiography.which also described in Macleod syndrom.
There is hyperlucent left lung with shifting of the mediastinum to the left side during inspiration.
we have lost of volume of the left lung with expiration too.(elevetion of the left hemidiaphragm.)
there is not Swyer-James syndrome.
on the frontal view we have enlarged of the pulmonary’s hilum and donuds sing on the lateral view.
on the pulmonary arteriogram, main branches of pulmonary arteries looks good but we can t see after main left pulmonary arterie but only a few branches of the LUL.(or hypoplastic or obstructive) the missionary of Africa is a good information (i am sure…) but i don t now yet how to make the conection.
9 rib fracture on the right.
That the patient is a missionary is not relevant. Sorry if it mislead you.
i am change my mind is Swyer–James–MacLeod syndrome
Both radiographs show hyperlucent left lung, with reduction of bronchovascular pattern. There is normal diagphram function allthough left dome is elevated, it may result from volume loss of the left lung. Mediatinum is shifte to the right during inspiration, indicating that the lung is not only of a reduced volume, but also is not ventilated equally with the opposed side. What is more, we see the reduced branching of the left pulmonary artery, but the pulm. trunk and main left pulm. artery are normal in size – it neglect the congenital cause of the problem visualized.
Summarizing: lef tung of a reduced volume, limied ventilation and blood supply, resulting from not congenital reasons.
All my votes for Swyer-James Syndrome.
BTW. Do I see contast agent in patient’s aesophagus on the lateral CXR?
No, there is no contrast in the esophagus.
I believe your interpretation of the findings is correct.
You overlooked the cause.
I imagine many of you are waiting for a hint. Will give you two:
1. Correct diagnosis has not been mentioned.
2. Look at the films
4.None of the above
It’s a Case of Unilateral bullous emphysema of lung.
There is mild left side cardiac and mediastinal displacement, smaller hemithorax; absent pulmonary artery shadow; ipsilateral hemidiaphragm elevation; ipsilateral absent or grossly diminished pulmonary vascular markings; and contralateral lung hyperinflation and herniation beyond the midline and no air trapping on the expiratory chest radiograph. SO I WOULD SUGGEST IT TO BE A UNILALATERAL PULMONARY ARTERY AGENESIS
The principal differential diagnosis is Swyer-James or McLeod’s syndrome in which the affected hemithorax may or may not be small, the expiratory radiograph shows air trapping,
nice case professor….really tough one !
although you mentioned that there was air trapping in expiratory view..but i was unable to appreciate.
Anyway thanks again for the nice teaching points.
.
looking forward for your next case.
There is not air trapping.
simple the right lung is working and the left no.
is not Swyer–James–MacLeod syndrome
-In unilateral bronchial obstruction the mediastinum shifts towards the abnormal lung on inspiration and towards the normal lung on expiration.case 58
-On the Left Pulmonary Artery Hypoplasia the most frequent findings on the chest x-ray include decrease in size of the affected hemithorax and compensatory hyperinflation of the contralateral hemithorax, elevation of ipsilateral diaphragm and ipsilateral shift of mediastinum.
the problem is that we can see the main branch of Left Pulmonary Artery that is no atresia.(it was great..)
is not bronchial tumor.
i think is a kind of hypoplasia or a chronic stenosis of the artery
Do not elaborate. Look at the lateral film
answer is 4
..in AP l’ilo di sx non sembra corrispodere all’arteria polmonare che è ipoplasica( vedi angio-pneumo); in LL si conferma una opacità ilare di ndd.Potrebbe trattarsi di un broncocele, conseguente al difetto vascolare, mentre l’ipertrasparenza “bloccata” trattarsi di un difetto di svuotamento respiratorio conseguenziale.
i will say somethink else because is the last day.
the aortic arch it looks like be in both sides of the trachea.
a double aortic arch with compression of the airway?
is very difficult case profesor and the films it doesn’t help
sorry 🙂
Actually, you saw the lesion in the PA view. Looking at the lateral view, the tumor is very obvious, projecting over the tracheal lumen.
The films do help: the diagnosis was made in the plain film and later confirmed with CT and bronchoscopy after the tumor has been overlooked for a few years.
Unlike you, I believe the case is easy if you look at the lateral view, as I did thirty years ago.
sorry for my bad english.
i mean the quality of the films….
professor i love the films too 🙂
i think my quality is not good because the mass was there and i didn’t saw it.
i will try harder next time.
ps: i am sure thirty years ago you was the same great mind as you are now.
Your English is OK. The important thing is to discover the lesion and to make an educated guess.
I do not have a great mind: just apply basic knowledge.
It is difficult case.
My previous post where I voted for Swyer syndrome was not published.
Lateral and PA film both show hyperlucency mainly in the area of left upper lobe, mainly it’s ventral parts. No signs of chest surgery. How about some limited no-tension pneumothorax? Lobe affected by bullous changes? I give up:)
But excuse me , it is a case of air trapping by a bronchial and left bronchus mass, so what is the mechanism of vascular attenuation ??
If the lung is not working properly, the blood supply diminishes accordingly.