Dr. Pepe’s Diploma Casebook: Case 50 – SOLVED!

Dear friends,
Today I am presenting radiographs and CT of a 27-year-old male with fever and malaise. Leave me your thoughts and diagnosis in the comments section and come back on Friday for the answer.
Diagnosis:
1. Teratoma
2. Thymoma
3. Lymphoma
4. None of the above
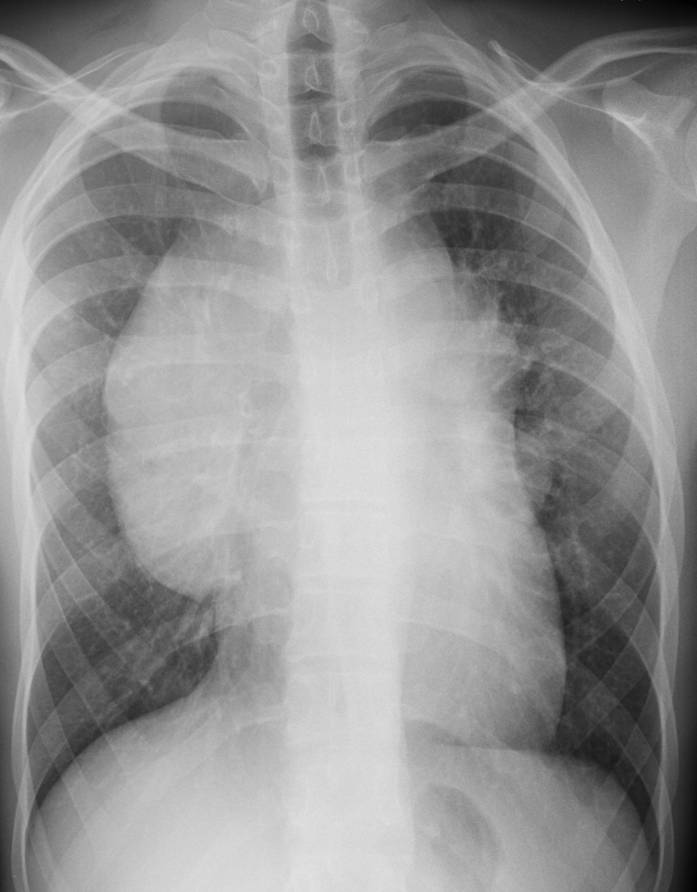


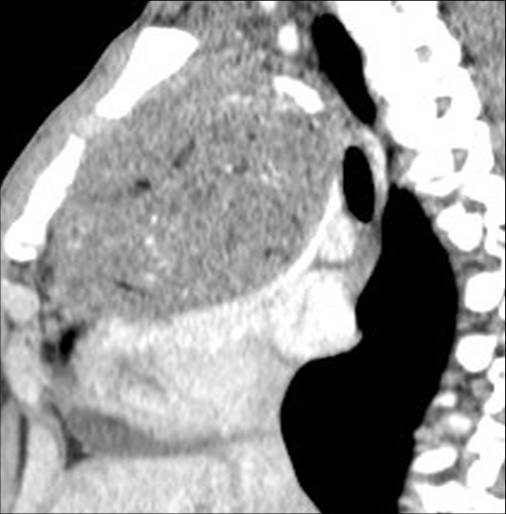

Fig. 1
Findings: Chest films show a mass located in the anterior/superior mediastinum. CT depicts areas of fat density (A,B, white arrows) and coarse calcifications (A,B, red arrows). Of the possible diagnoses, lymphoma can be excluded because untreated lymphomas do not calcify. Of the remaining two possibilities, the presence of fat points to a teratoma.
Final diagnosis: mediastinal teratoma (malignant)
This case is presented to discuss anterior mediastinal masses. As was mentioned in Diploma case #41, the mediastinum is divided into four compartments (anterior, middle, posterior and thoracic inlet). To facilitate the differential diagnosis, the anterior mediastinum is subdivided into two compartments (superior and inferior) by a horizontal line drawn at about the level of the hila (Fig. 2). In this presentation I will focus on masses in the anterior/superior mediastinum. Masses in the anterior/inferior mediastinum were analysed in a previous presentation (Diploma case #11).
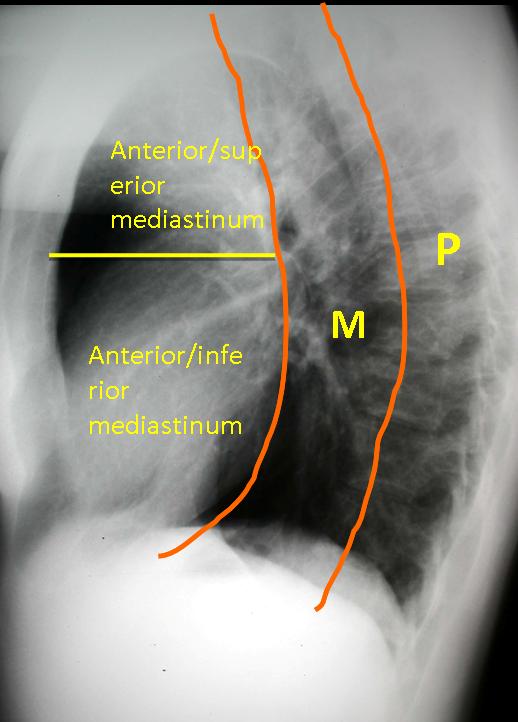
Fig. 2
For practical purposes, most masses in the anterior/superior mediastinum fall within the ‘three Ts’: thymoma, teratoma, and ‘terrible’ lymphoma. The main differential diagnosis resides in these three possibilities. There is a small percentage of less common tumours (carcinoid, carcinomas, etc.), which will not be discussed in this presentation. I would like to show you my personal approach to anterior/superior masses, based mainly on their CT density. In this approach, there are four possible CT densities to analyse: fat, fluid, soft-tissue and calcium.
FAT DENSITY
Discovering fat within a mass is important because it is an almost exclusive finding of teratomas, the most common type of mediastinal germ-cell tumours. Teratomas occur at any age, although they are more common in young adults. They are mainly located in the anterior/superior mediastinum, around 75% show areas of fat attenuation on CT (Fig. 3), and around 33% calcify.
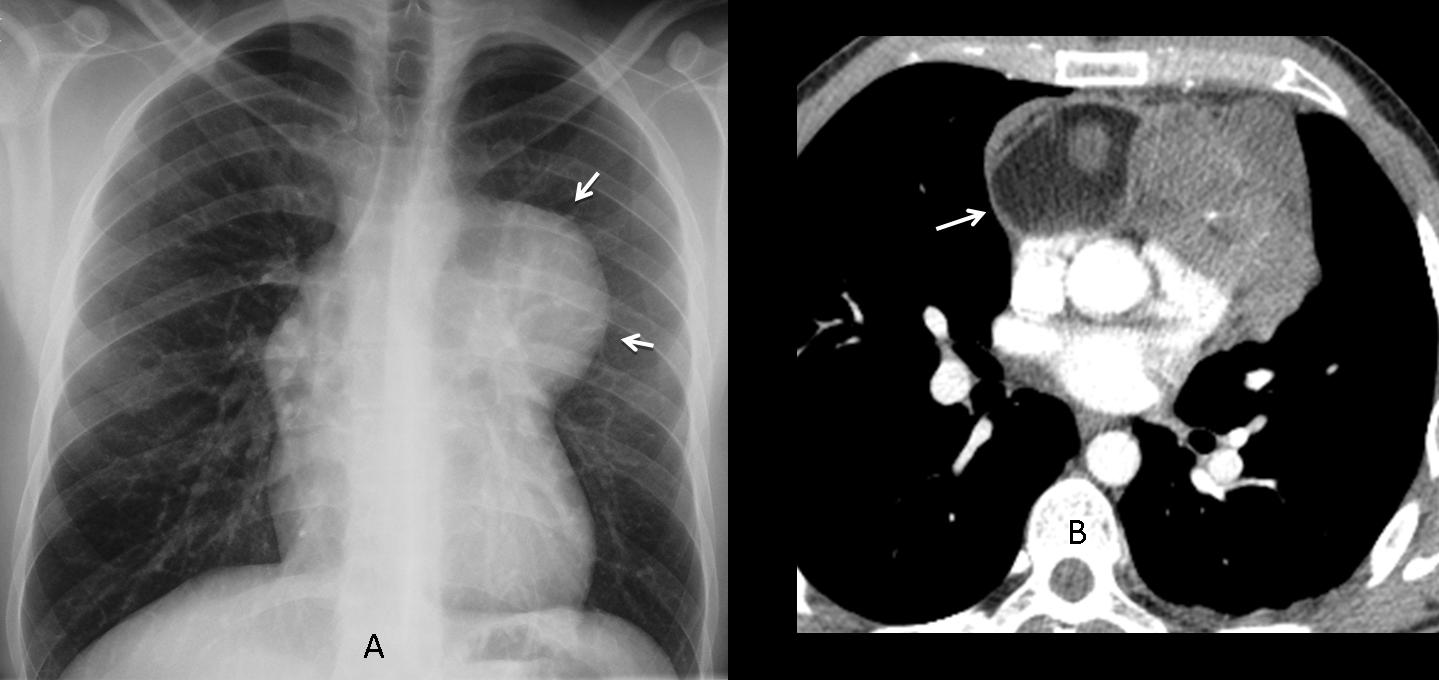
Fig. 3
Fig. 3 (above): teratoma in a 39-year-old man. PA chest film depicts an anterior mediastinal mass (A, arrows). CT shows a large area of fat within the mass (B, arrow).
What would your diagnosis be in this 52-year-old asymptomatic man (Fig. 4, below)?
1. Cardiomegaly
2. Pericardial effusion
3. Mediastinal tumour
4. None of the above
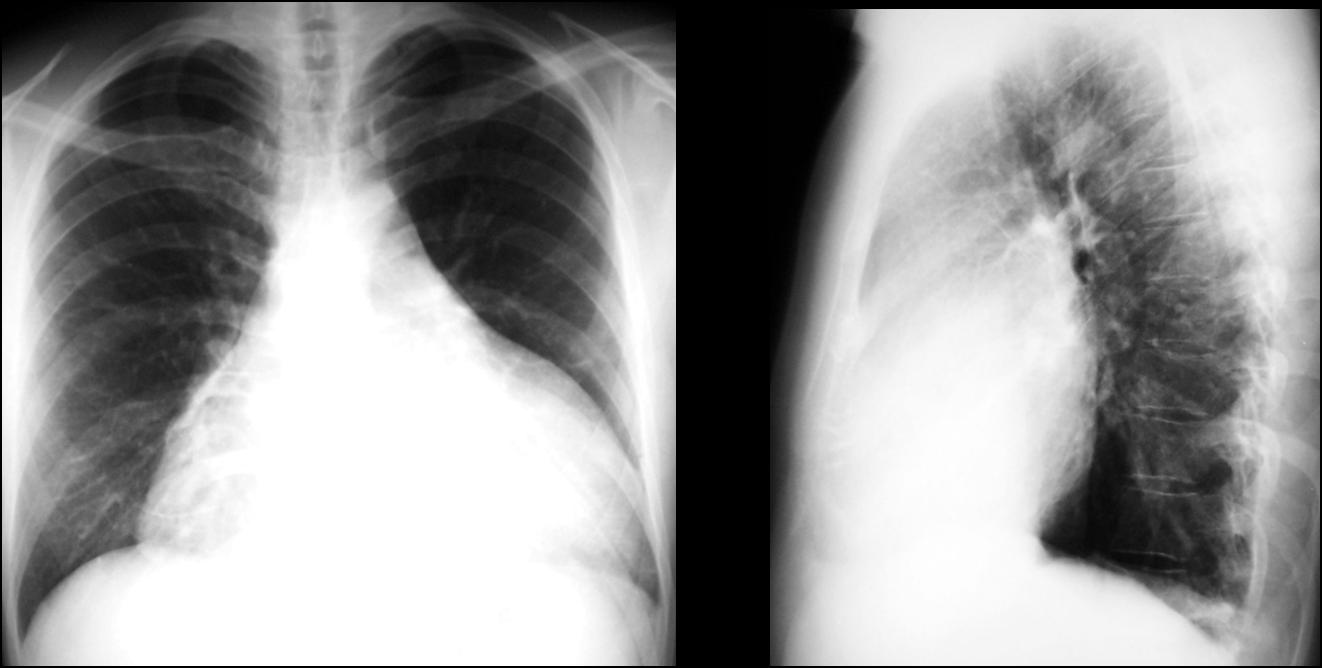
Fig. 4
Findings: chest radiographs show an apparently enlarged cardiac silhouette. However, in the lateral view, the heart is not enlarged and there is occupation of the anterior clear space, suggesting a mass originating in the anterior/superior mediastinum and wrapping itself around the heart. CT confirms the presence of a large fatty mass in the anterior mediastinum, extending downwards and surrounding the heart (Fig. 5 A-C, arrows). Diagnosis: thymolipoma>.
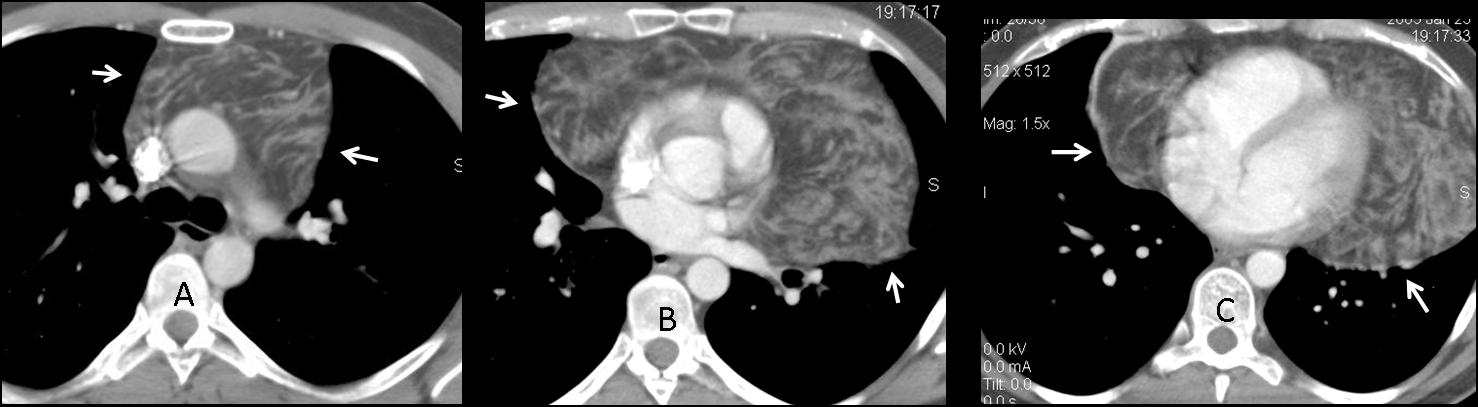
Fig. 5
Thymolipomas are uncommon thymic tumours, mainly comprised of fat. They are asymptomatic and usually grow to a large size before being discovered. They are soft and pliable, and can drape themselves around the heart and adjacent structures, simulating cardiac enlargement. CT typically shows a large tumour of mainly fat density.
FLUID DENSITY
This is the case of a 41-year-old man who arrived with signs and symptoms of acute mediastinitis. Enhanced CT was performed.
What would your diagnosis be?
1. Thymoma
2. Teratoma
3. Lymphoma
4. Congenital cyst
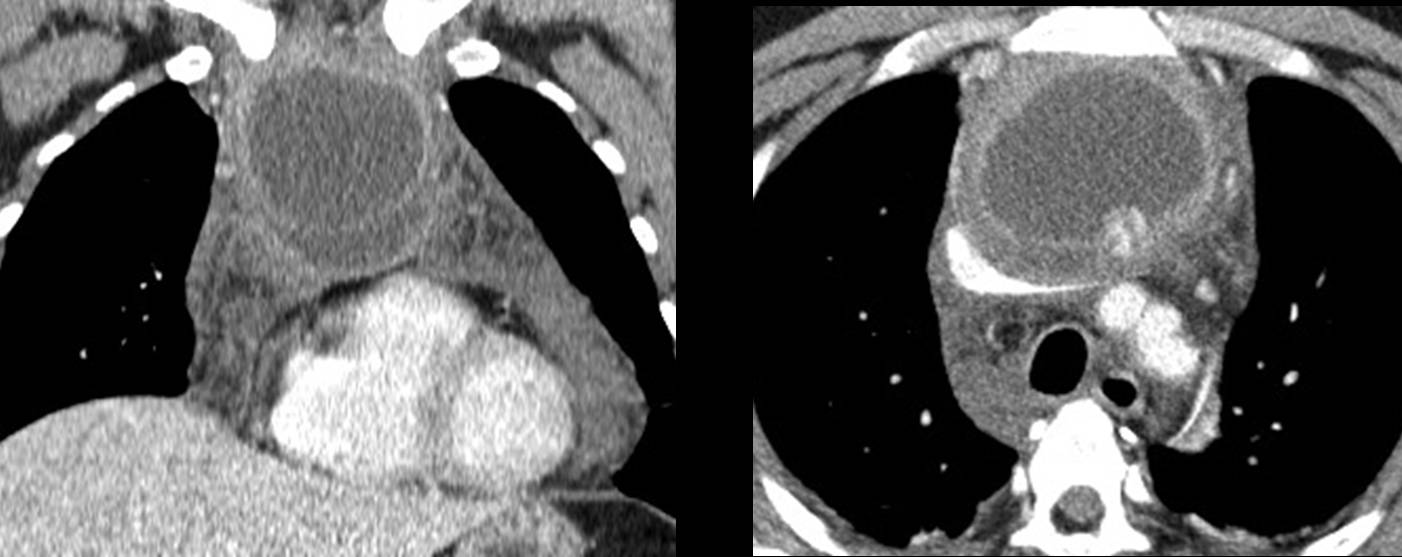
Fig. 6
Findings: axial and coronal enhanced CT images show extensive mediastinal involvement (Fig. 7 A,B, white arrows) and a cystic upper mediastinal mass (Fig. 7 A,B, red arrows). Surgery demonstrated an infected cystic teratoma as the cause of mediastinitis. The patient had an uneventful recovery (Fig. 7, C). We failed to identify the immature tooth (B, yellow arrow) which would have suggested the correct preoperative diagnosis.
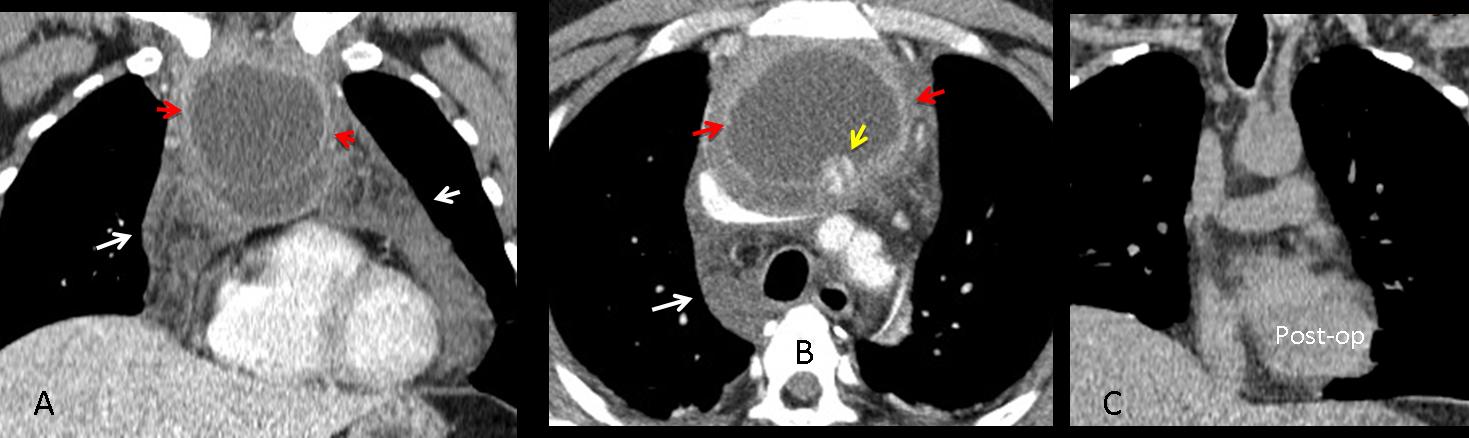
Fig. 7
Tumours with cystic areas may represent either teratomas or thymomas, and they cannot be differentiated on imaging findings alone. Lymphomas have areas of necrosis, but they usually do not have cystic areas. It is important to know that thymic cysts can occur after irradiation of mediastinal lymphomas.
SOFT-TISSUE SOLID MASSES
Below are images of a 43-year-old woman with marked anemia and a superior mediastinal mass (arrows).
Diagnosis:
1. Thymoma
2. Teratoma
3. Lymphoma
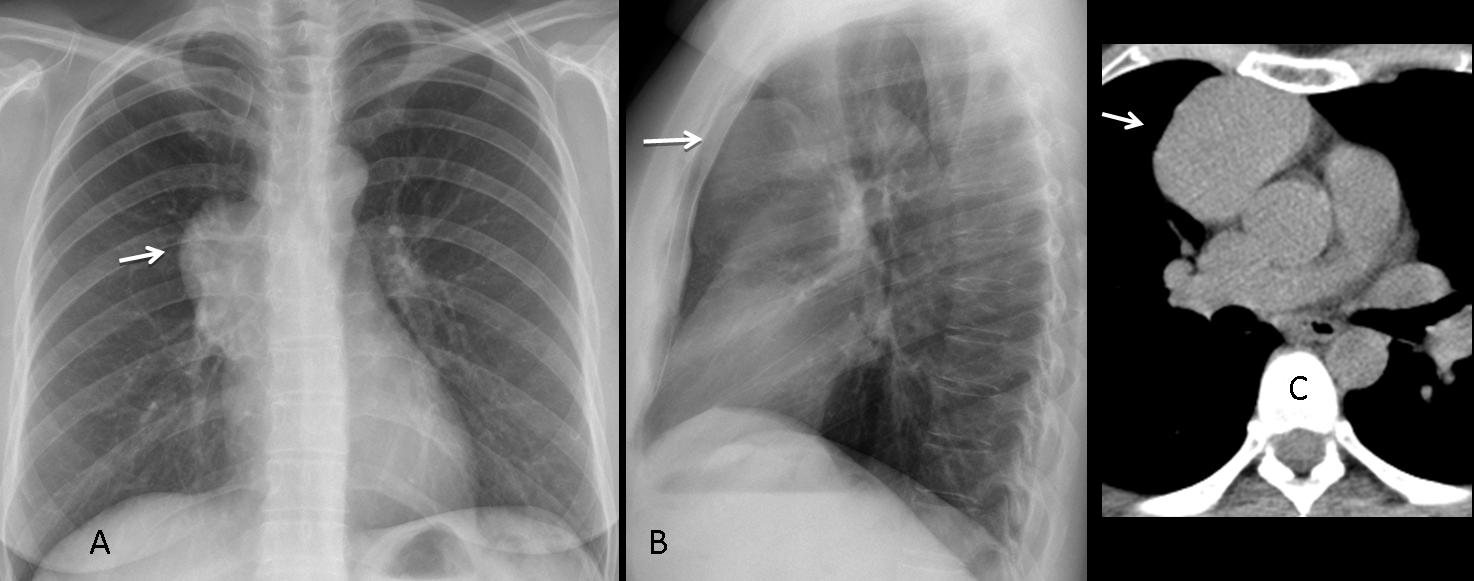
Fig. 8
Findings: chest radiographs and CT show a solid anterior mass with no specific imaging characteristics (A-C, arrows). Pure solid masses may correspond to any of the three ‘Ts’. In these cases, clinical findings may be of help. In this particular patient, the marked anemia could suggest the diagnosis of thymoma. About 5% of thymomas are associated with pure red cell aplasia, 10% hypogammaglobulinemia, and 40% myasthenia gravis.
Final diagnosis: thymoma with red cell aplasia.
Clinical findings also help to suggest the diagnosis of lymphoma. Most lymphomas occur in young patients with systemic symptoms. Hodgkin disease accounts for most mediastinal lymphomas. These tumours usually present as solid masses with areas of necrosis and are difficult to differentiate from other tumours (Fig. 9). Invasion of neighboring lung suggests lymphoma (Fig. 10).
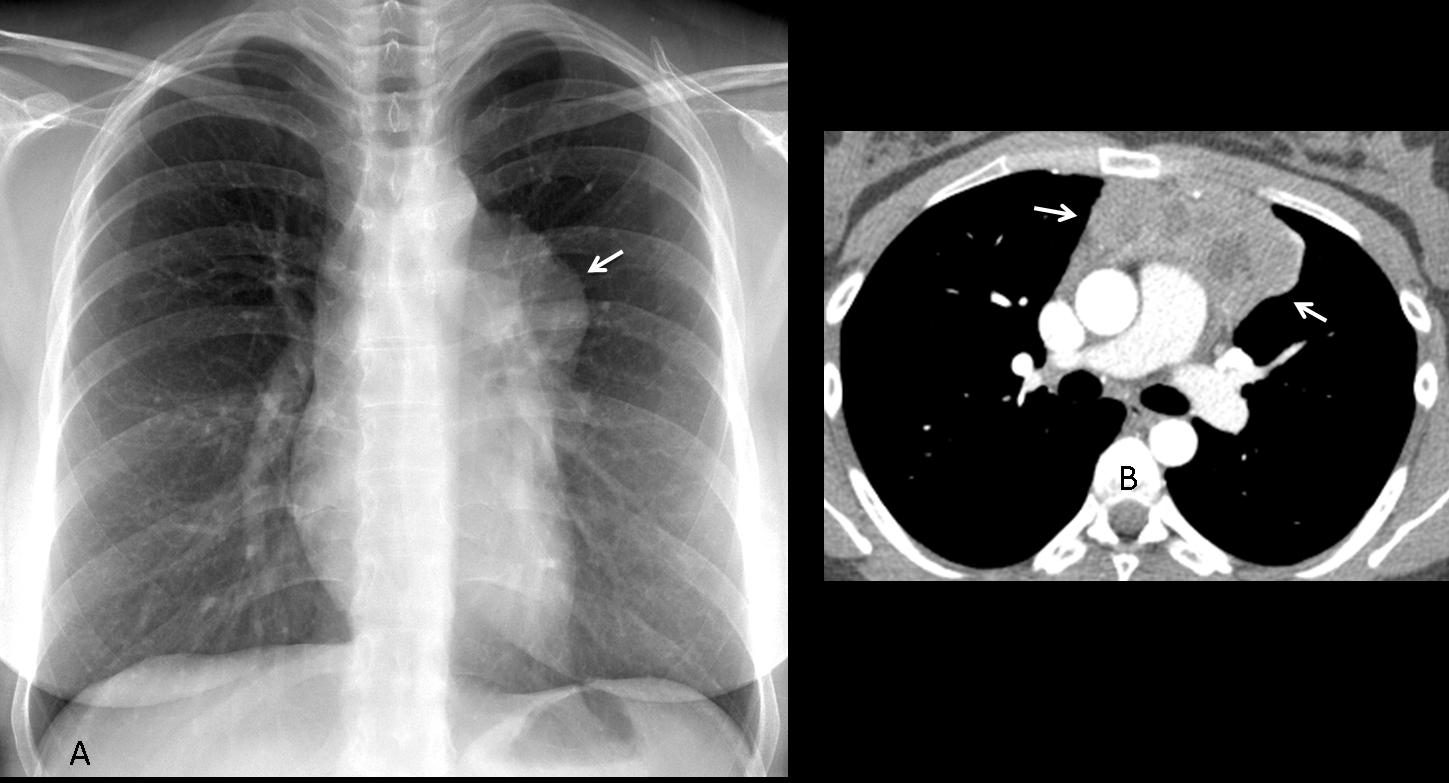
Fig. 9
Fig. 9 (above): 28-year-old woman with Hodgkin disease. Chest radiograph shows an anterior mediastinal mass (A, arrow) which on axial CT is irregular and shows areas of necrosis (B, arrows). The patient had lost weight and had fever and night sweats.
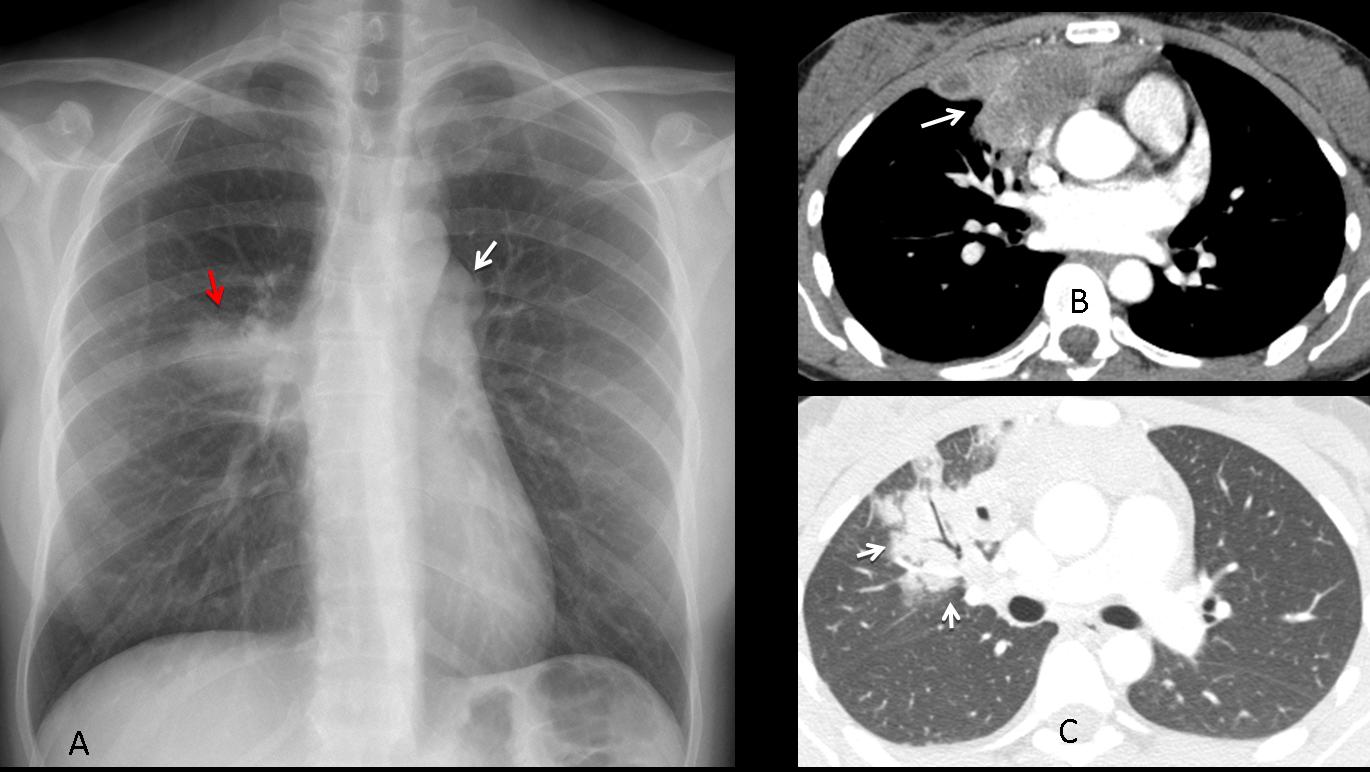
Fig. 10
Fig. 10 (above): 33-year-old woman with cough, fever and weight loss. PA radiograph shows an anterior mediastinal mass (A, white arrow) and a pulmonary infiltrate (A, red arrow). On axial CT a necrotic mass (B, arrow) is seen, with right lung invasion (C, arrows). Final diagnosis: Hodgkin disease.
CALCIUM
Two patients with calcified anterior mediastinal masses:
What is the least likely diagnosis?
1. Lymphoma
2. Teratoma
3. Thymoma
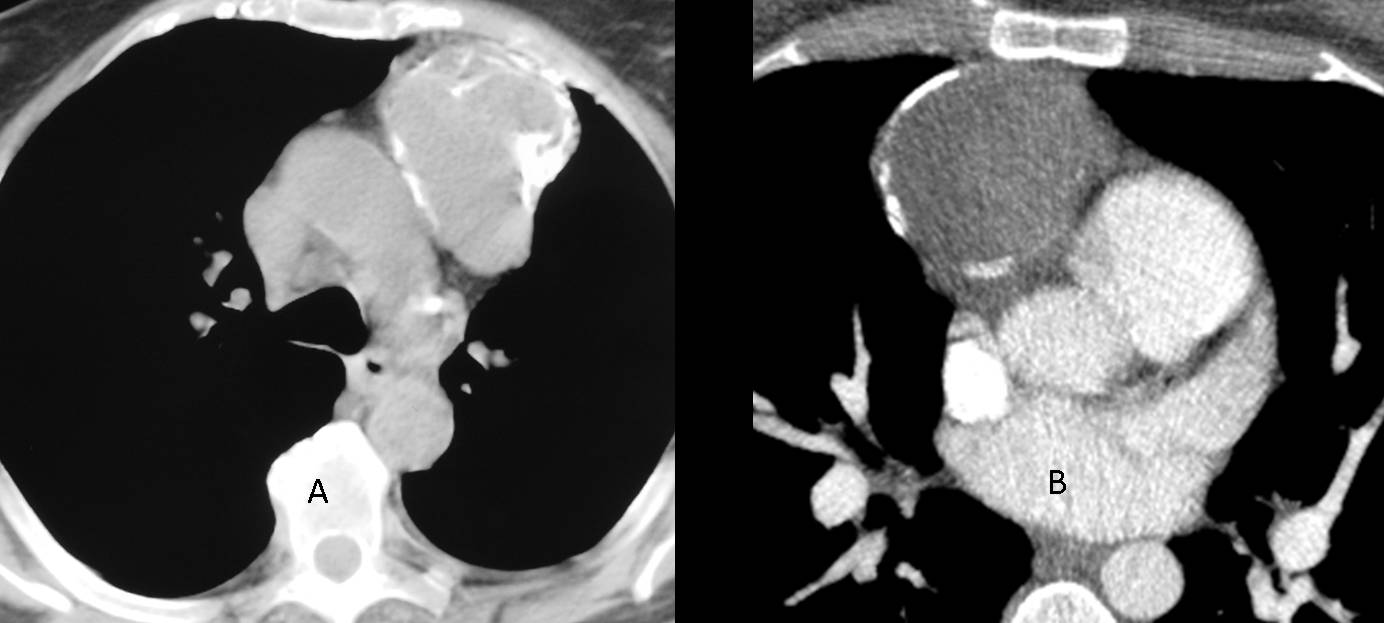
Fig. 11
Findings: axial CT images show anterior mediastinal masses with coarse calcifications (A) and a circular peripheral calcification (B). Since thymomas and teratomas may calcify and untreated lymphomas do so very rarely, the least likely diagnosis is mediastinal lymphoma. Both of these particular cases correspond to thymomas.
The incidence of calcification in thymomas varies from 10% to 40%. Circular peripheral calcification may occur in solid thymomas, simulating a cyst. Teratomas contain calcium in about 35% of cases (Fig. 12). About 5% of lymphomas show calcifications after radiation therapy.
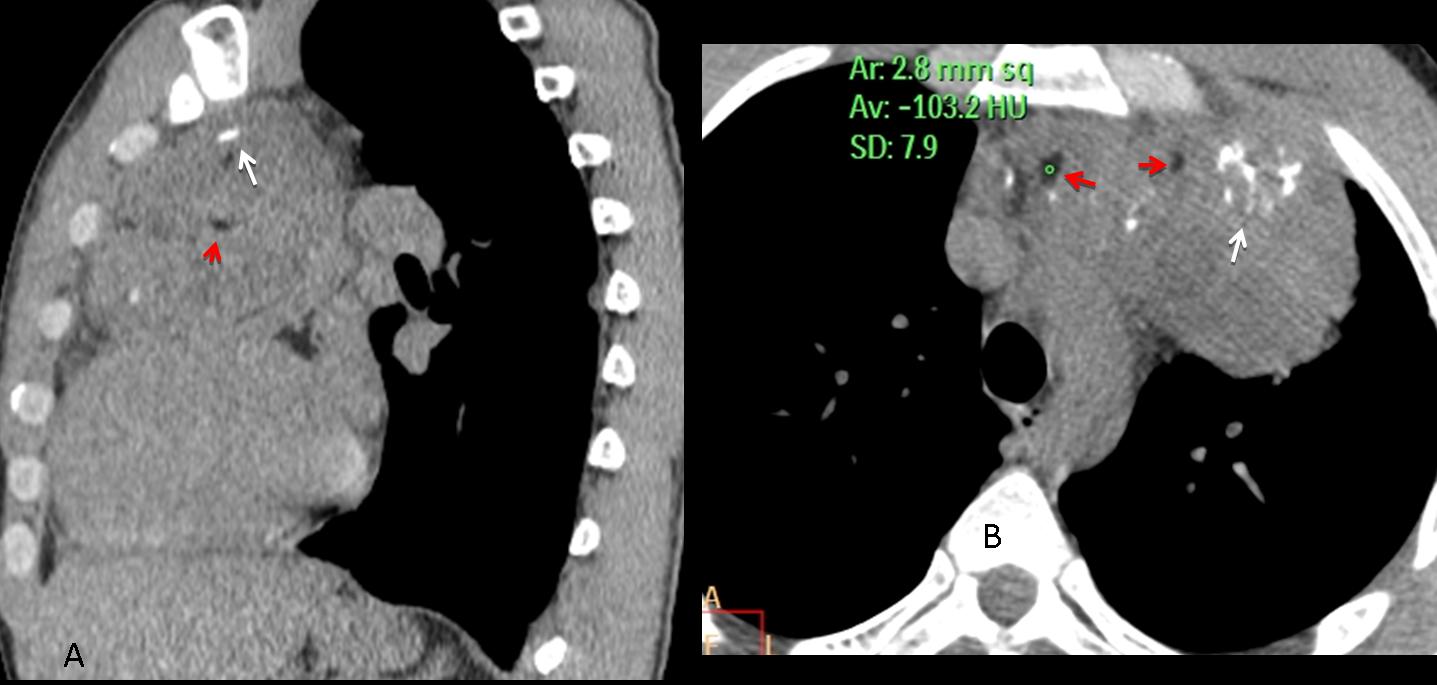
Fig. 12
Fig. 12 (above): 42-year-old man with a teratoma. Note the coarse calcifications (A,B, white arrows) and areas of fat attenuation, measuring -103 HU (A,B, red arrows).
MALIGNANCY
Lymphoma is the most common malignant process of the anterior mediastinum. It is difficult to determine whether a teratoma or thymoma is malignant unless obvious invasion of mediastinal structures occurs. Ipsilateral pleural nodules are indicative of metastases from thymoma (Fig. 13).
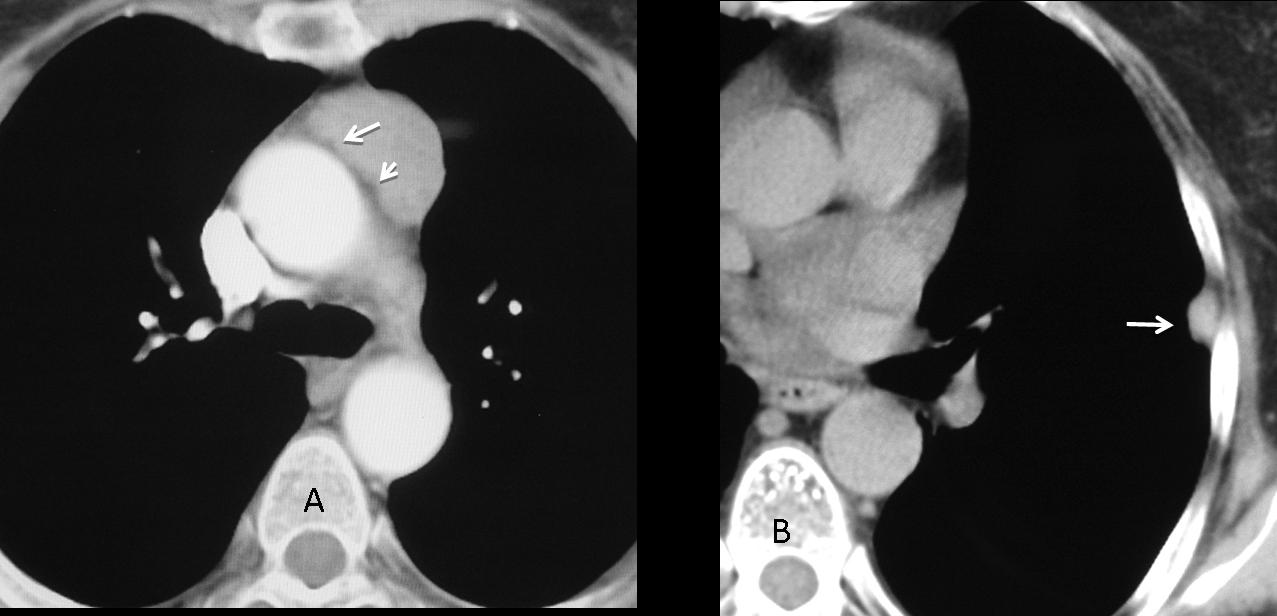
Fig. 13
Fig. 13 (above): thymoma with no signs of mediastinal fat invasion (A, arrows). One year after surgery, pleural metastasis was found (B, arrow).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice
1. Areas of fat attenuation are characteristic of teratomas, excluding the rare thymolipoma.
2. Untreated lymphomas do not calcify. An anterior mediastinal mass with calcium is probably a thymoma or a teratoma.
3. Lymphoma is the most common malignancy of the anterior mediastinum.
4. Clinical symptoms are useful:
– In a young patient with systemic symptoms, lymphoma is a likely diagnosis.
– About 40% of patients with thymoma have myasthenia gravis.


…e la LL?….Comunque bulky-linfoma
….scusa…la TC ?…
Sorry, they will correct the mistake promptly.
….la regola dell 4 T per le masse del mediastino anteriore…timo-t-linfoma-tiroide-tumore germinativo: la presenza delle calcificazioni depone per tumore germinale( a-f-p, innalzamento)….Prego correggere la primitiva diagnosi che non teneva conto delle calcificazioni visibili solo con la TAC….Scusami tanto professore!
…la “massa” nonostante le sue dimensioni, non infiltra le strutture circostanti ma le disloca e le comprime: se escludi la variante “matura” del teratoma, dovremmo indirizzarci verso una patologia “benigna”….Castleman’s disease?…
None of the above..
Definitive diagnosis of mediastinal mass can not be given by CXR only… Anterior mediastinal location of lesion can be seen as it is silhouting ascending aorta. D/D includes all above is plus ascending aortic aneurysms.
ROFL…. didnt realized there were CT images also..
CT demonstrates anterior mediastinal mass without lobulation and multiple hyperdense foci (i think calcification… though its CECT may be ??? vessels) and hypodense foci (likely fat) within the lesion.. so my first d/d would be Teratoma.
It looks more like a teratoma, but can be thymoma tumor.
I dont like RUL, is it mts?
No, RUL is OK.
CT demonstrates anterior mediastinal mass with multiple hyperdense foci (calcifications) and hypodense foci (likely fat) within the lesion…so I’m thinking teratoma (but it’s dificil to exclude thymoma).
Proffesor is very tricky!
It might be as well thymoma or teratoma. But as it is the young male and tumor seems to infiltrate aortic arch- so it is probably malignant. I vote for seminoma.
I can`t see the lymph nodes or are they enlarged?
I don´t believe you can evaluate aortic infiltration with just two views. It is difficult enough with the whole study!
This two views do not show any enlarged lymph nodes.
So maby it`s the mass growing from the heart or pericardium?
The patient has fever and malaise- I think it`s significant. Lymphoma don`t have calcifications unless they`re after radiotherapy.
Teratoma
Anterior Mediastinal Mass
we can use the 6 “T”s to help us remember the causes of anterior mediastinal masses.
•Thyroid lesions
•Thymic lesions (and parathyroid masses)
•Teratomas (and other germ cell tumors )
•”Terrible” lymphoma (Lymphadenopathy)
•Tortuous vessels (dissecting aorta, right arch)
•Trauma
is a dense solid mass with peripheral and internal calcifications in anterior-medial mediastinum ,smooth in contour ,with out faty or cystic elements in a 27-year-old male with fever and malaise.
-is not thyroid there is no conection (except of ectopic thyroid tissue)
-is not thymic lesion (thymomas which usually occur in 5th or 6th decade )
-is a young boy to has so many calcifications in a ascending aorta aneurism.
it remains to be seen lymphoma after therapy, Teratomas with other germ cell tumors and trauma.
teratoma
Sooo… First one to consider is teratoma (mature) because of lack of infiltrations (on the pictures posted) calcifications- cntral and rim like (which can be also seen in thymoma and treated lymphoma, areas of low (fat) attenuation- also the lesion is central more typical for teratoma.
DDX thymoma, less probable treated lymphoma.
The correct diagnosis is implied in your description. If the mass has areas of fat attenuation, the only tumor to consider is teratoma.
I call for a free point during EDiR exam ;]
Will pass your request to the Board ,-)
I vote for thymoma.
Seminoma
The first hypothesis for me it’s a seminoma. It’s in the anterior mediastinum, over the heart, the symptoms. The patient is a little bit younger, and the mass is ispected to be more heterogenes with thymoma. Limphoma has no calcification before treatment.
from the PA x – ray , I suggest it is a pulmonary aneurysm , axial sections of the CT will be helpfull
professor what is this calcified branch in posterior aspect of the mass on sagittal view?is partial volume effect?
It is an enhanced external vessel. When I selected the image I didn’t realize that this shadow could be misleading.
es un teratoma
There is an anterior mediastinal mass with well defined borders. There are calcifications and areas of low attenuation on TC that could correspond to fat (I would like to measure them with a ROI). With all this I would say Mature Teratoma.
CXR: large mass silhoutting mainly the right mediastinal border, causing an obtuse angle with the right lung.
CT: large, anterior mediastinal mass, with areas of calcifications and low attenuation spots (fat). Based on the above mentioned descriptions, I’m leaning towards Teratoma.
i think teratoma…
Because the Fat and calcified areas I would vote for a Germ cell tumor, like a Teratoma, followed by a Seminoma, both can have that appearance. Nevertheles it could not be so simple, It has to be something more…
A very, very, very wonderful lesson!!!!!!!!!!!!! Many thanks and congratulations dr Pepe!!!!!!!!! I mistaked only one case, because i’m Radiologist after 44 years, mu father was Radiologist and my grandfather soo………
Congratulations. Very glad to have you with us!