Dr. Pepe’s Diploma Casebook: Case 67 – SOLVED!
Dear Friends,
The last Diploma case of the year presents the scout film of a 76-year-old woman after cardiac surgery. Is there something not right? Examine the images below, leave your thoughts in the comments section and come back on Friday for the answer.
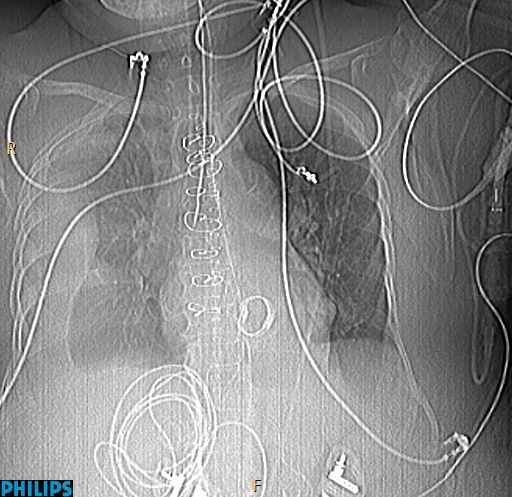
Findings: Portable chest radiography shows a right pleural effusion (A, white arrows). There is a prosthetic heart valve (A, yellow arrow) and numerous EKG leads projected over the chest. Metal sutures are seen in the sternum, and under them an endotracheal tube is visible, its tip located in the right main bronchus (A, red arrow). Coronal CT confirms the location of the distal endotracheal tube in the right main bronchus (B, arrow).
Final diagnosis: endotracheal tube in right main bronchus.
This case is presented to discuss erroneous positioning of chest catheters and tubes. Although discovering a malpositioned catheter may not seem as glamorous as diagnosing an obscure disease, it can be a great service to the patient, eliminating a potential (or present) harm. I will center the discussion on common complications of endotracheal tubes, intravenous lines, and pleural tubes.
Endotracheal tubes are placed to assure airway patency or provide assisted ventilation. The tip of the tube should be located 5 cm above the carina to avoid hitting this structure during respiration, which would result in erosion of the mucosa and bleeding. The tip should be at least 3 cm distal to the vocal cords to avoid injuring them with the inflated cuff.
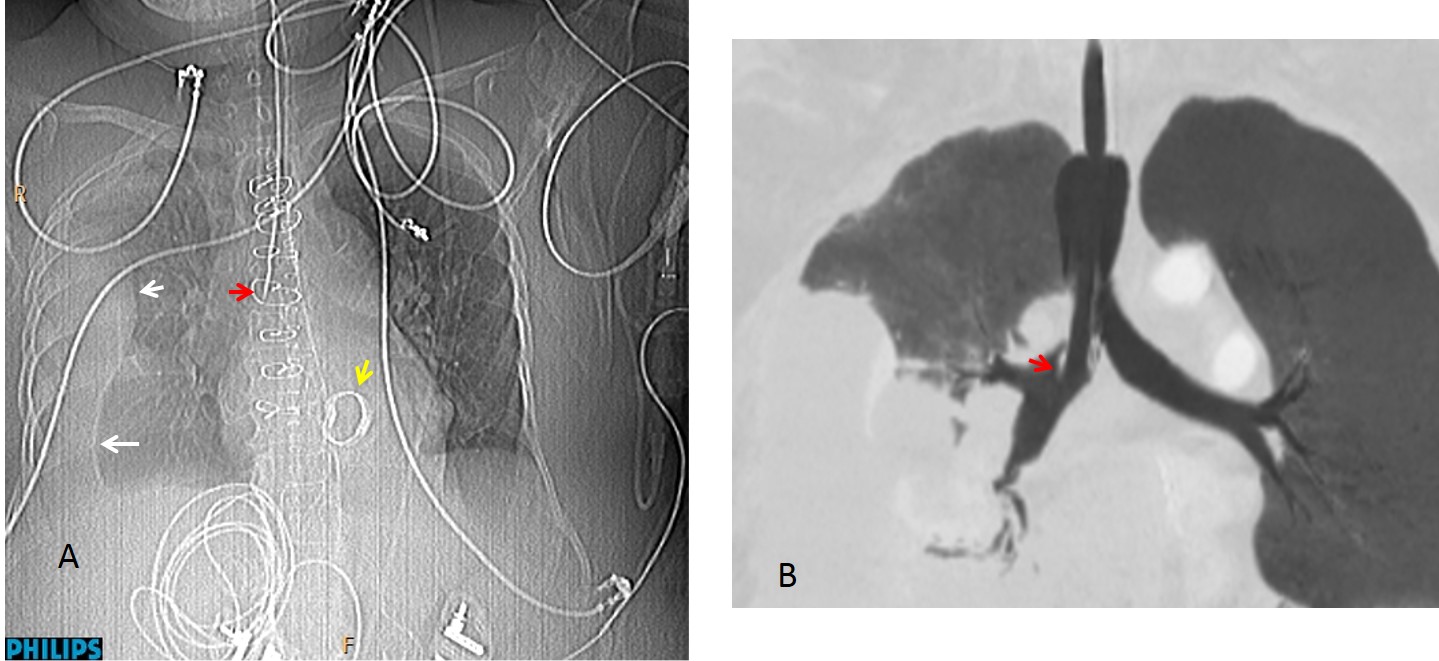
The most common acute complications of endotracheal tubes are: malpositioning and tracheal injury. About 10-15% of endotracheal tubes are erroneously positioned. In half the cases, the tube enters the oesophagus and in the other half, the tip is placed too low and often enters the right main bronchus, causing collapse of the contralateral lung (Fig. 1).
Fig. 1
Fig. 1: 67-year-old woman after brain surgery. The initial post-op chest film shows left lung collapse secondary to an endotracheal tube pushed into the right main bronchus (A, arrow). After the tube is repositioned (B, arrow), the collapse disappears.
Another complication occurs when the cuff is overinflated. A normal cuff should not expand the tracheal walls (Fig. 2). When cuff size exceeds 1.5 times the diameter of the trachea, complications occur, such as tracheal injury resulting in tracheal rupture (Fig. 3) or late stenosis.
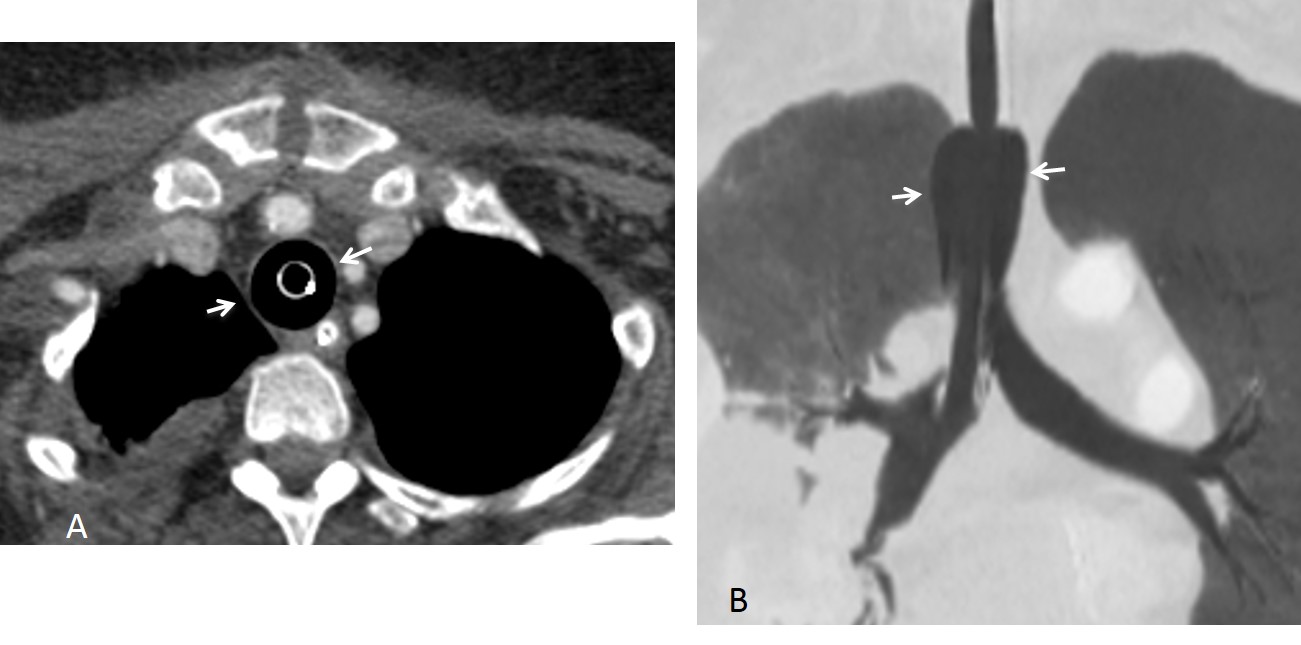
Fig. 2
Fig. 2: Overinflated cuff, visible on axial (A, arrows) and coronal (B, arrows) CT.
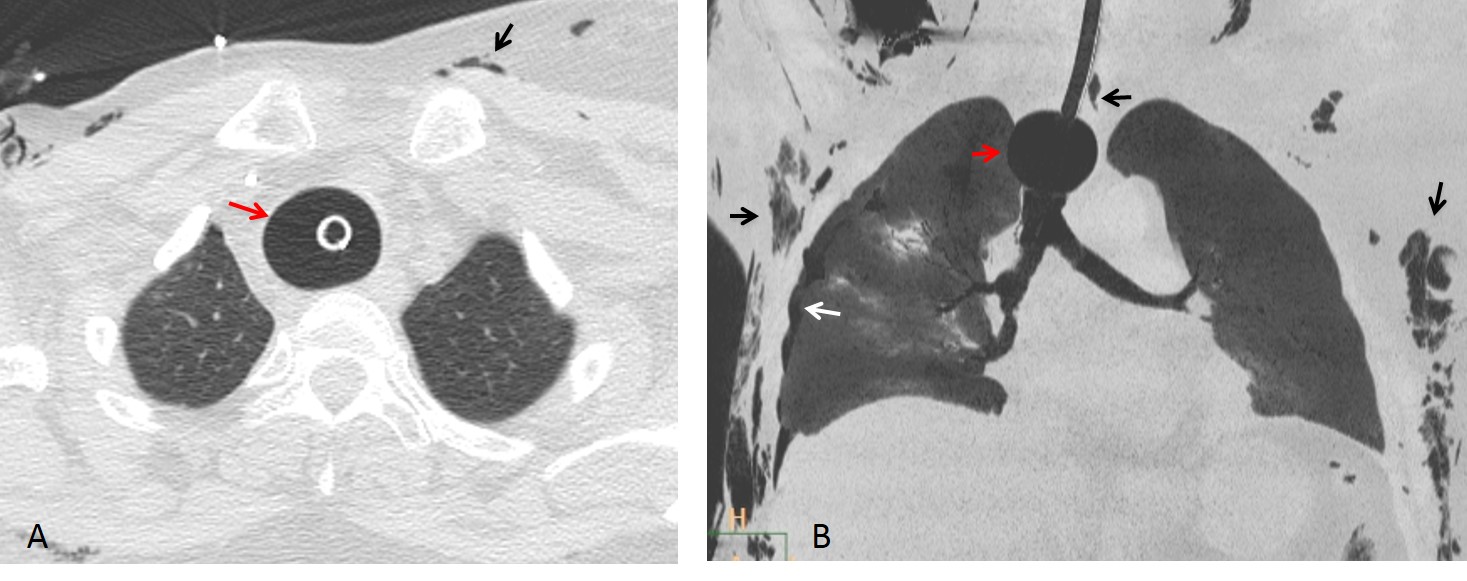
Fig. 3
Fig. 3: Axial and coronal CT show an overinflated cuff (A and B, red arrows) causing tracheal rupture with subcutaneous and mediastinal emphysema, pneumothorax, and pneumomediastinum (A and B, black and white arrows).
Pleural chest tubes are used to drain fluid or air from the pleural space. The tube tip is placed in the apex for draining a pneumothorax and in the base for fluid drainage. Failure of drainage indicates an incorrect tube position (Fig. 4).

Fig. 4
Fig. 4: chest tube that it is not properly draining a pneumothorax, likely because the tube is twisted in the pleural cavity and the tip does not reach the apex.
One common example of improper tube position is within the major fissure. These tubes may or may not function correctly. Malposition occurs more often when tubes are placed in haste. They are easily recognised in chest radiographs because of their oblique trajectory in both the PA and lateral views (Fig. 5 ).
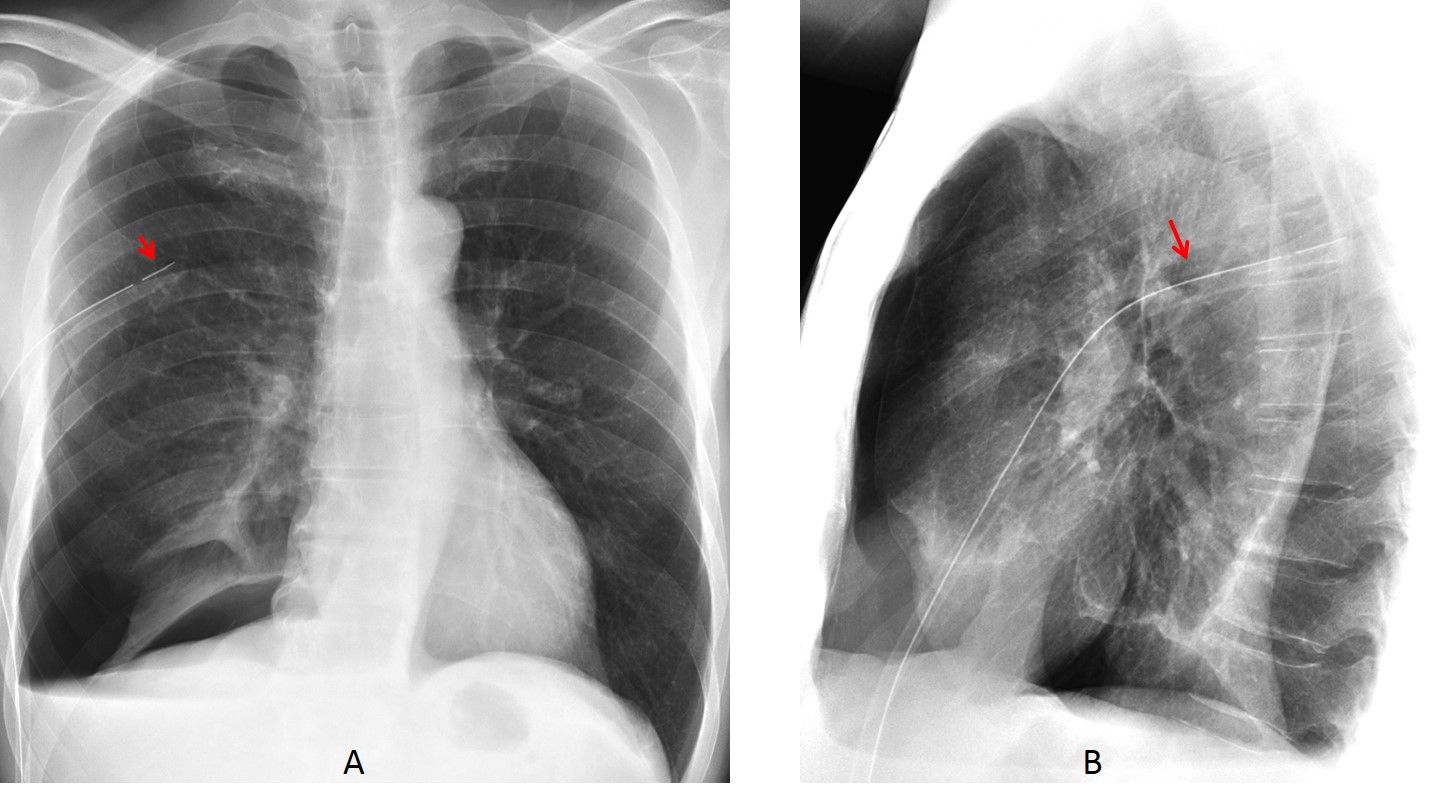
Fig. 5
Fig. 5: tube in the major fissure. The intrafissural location of the tube is obvious because it is seen within the chest in both projections (A and B, arrows). When the tube is properly located at the pleural surface, it should be seen at the periphery in one of the views.
Occasionally, the tube is placed within the lung parenchyma, causing pulmonary laceration and hemorrhage. CT study is necessary to evaluate this complication (Fig. 6).
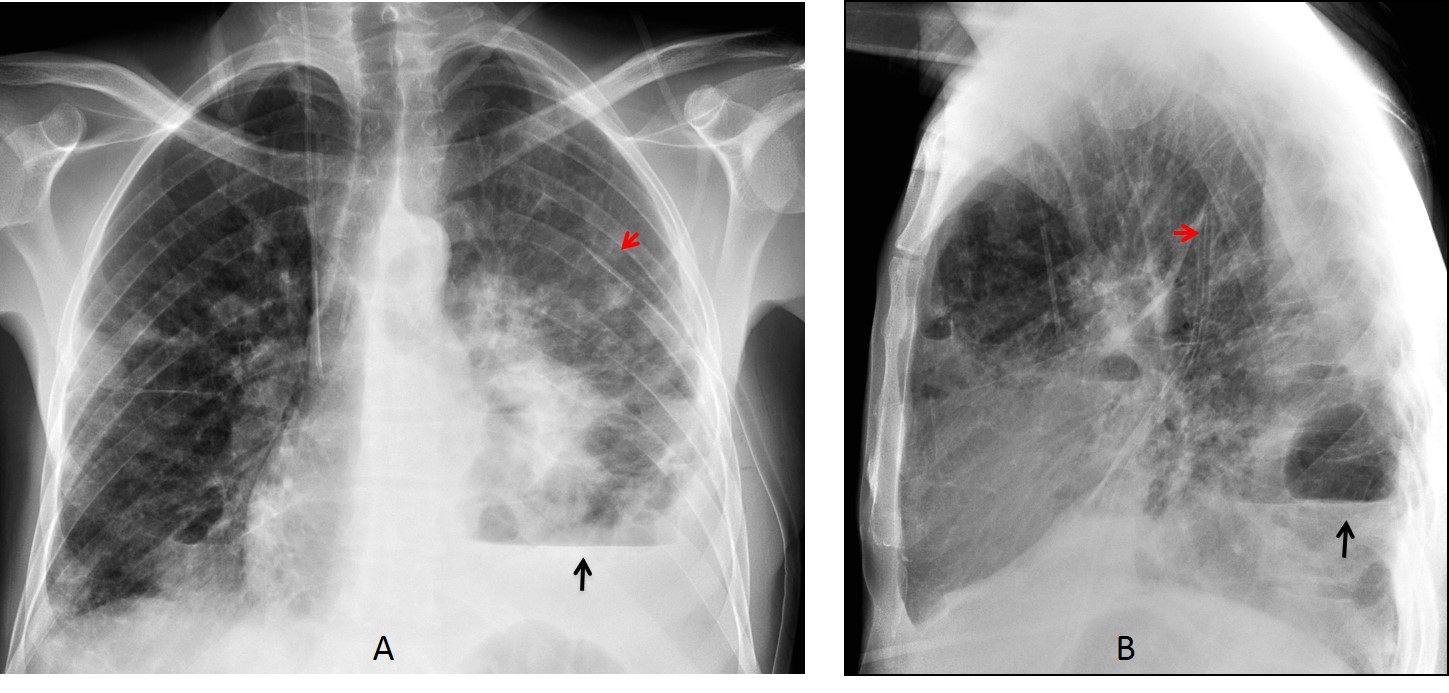
Fig. 6 A&B
Fig. 6: 43-year-old man with septic pulmonary emboli and a loculated basal pneumothorax (A and B, black arrows). The chest tube is visible inside the chest in both projections (A and B red arrows) indicating an intraparenchymal location.
Coronal and axial CT images show the chest tube perforating the lung parenchyma (C and D, arrows), with hemorrhage around the tube.
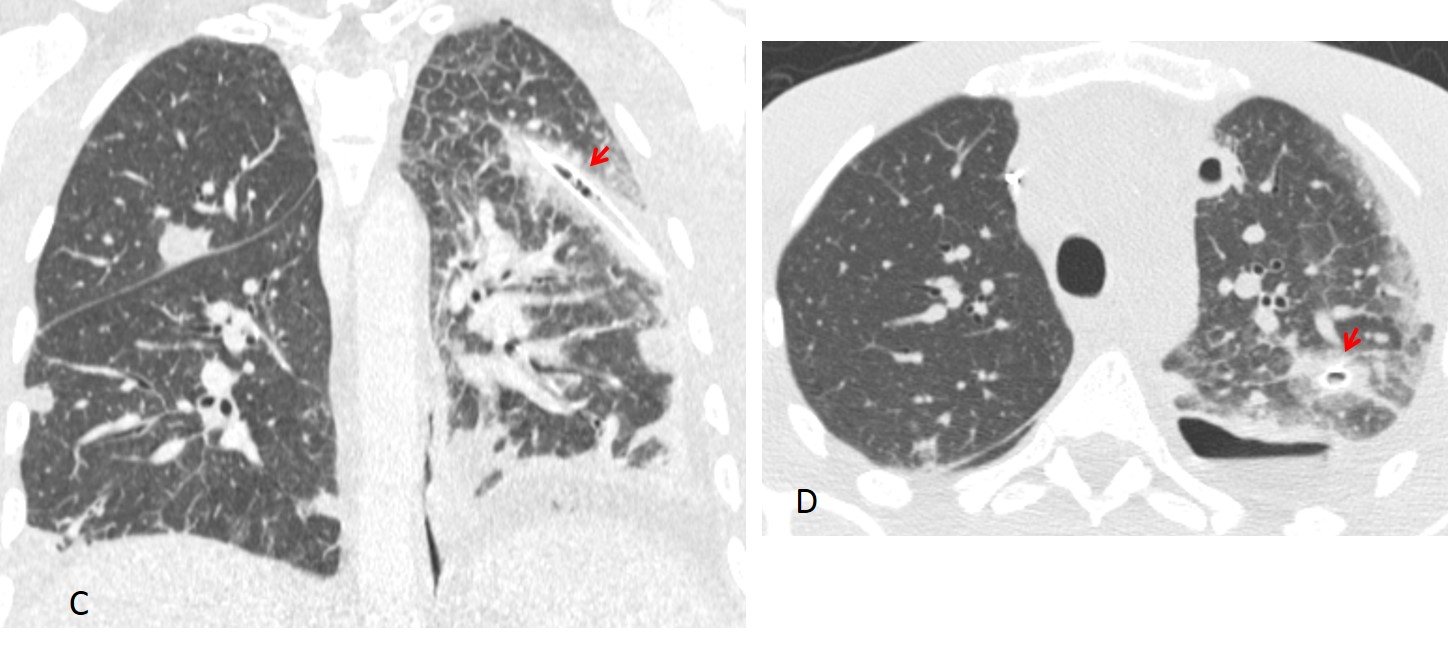
Fig. 6 C&D
A rare complication when placing basal tubes is perforation into the abdominal viscera, causing laceration of the spleen or liver (Fig. 7).
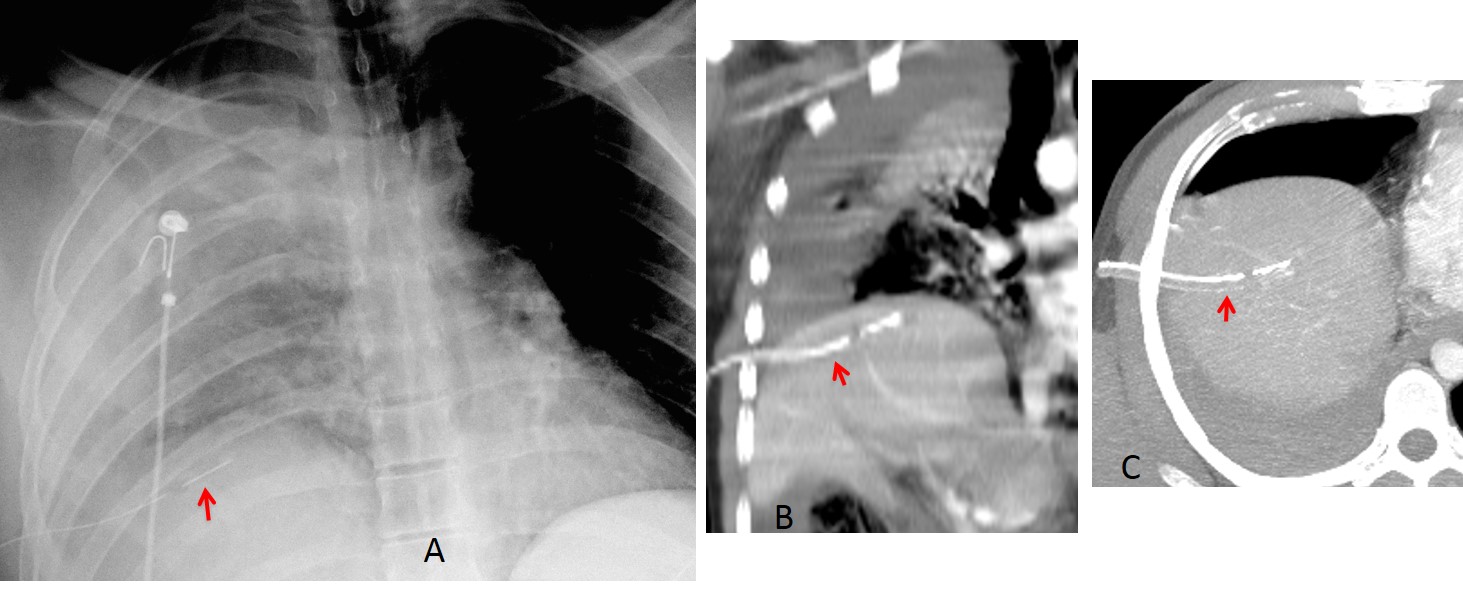
Fig. 7
Fig. 7: 28-year-old man after a car accident. Supine chest film shows right pleural fluid and pulmonary contusion. A tube has been placed at the right base (A, arrow). Coronal and axial CT show that the tube has entered the liver (B and C, arrows).
Venous catheters are used for administering medication or measuring central venous pressure. The optimal location of the catheter tip is within the SVC, above the right atrium. Placement in the right atrium increases the risk of arrhythmia and cardiac perforation.
Venous catheter malposition occurs in up to 40% of cases. Malposition interferes with CVP measurement and can lead to harmful effects when medication is deposited in the wrong location. The catheter may become looped inside the SVC, which may lead to formation of a knot and subsequent problems when removing the line (Fig. 8).
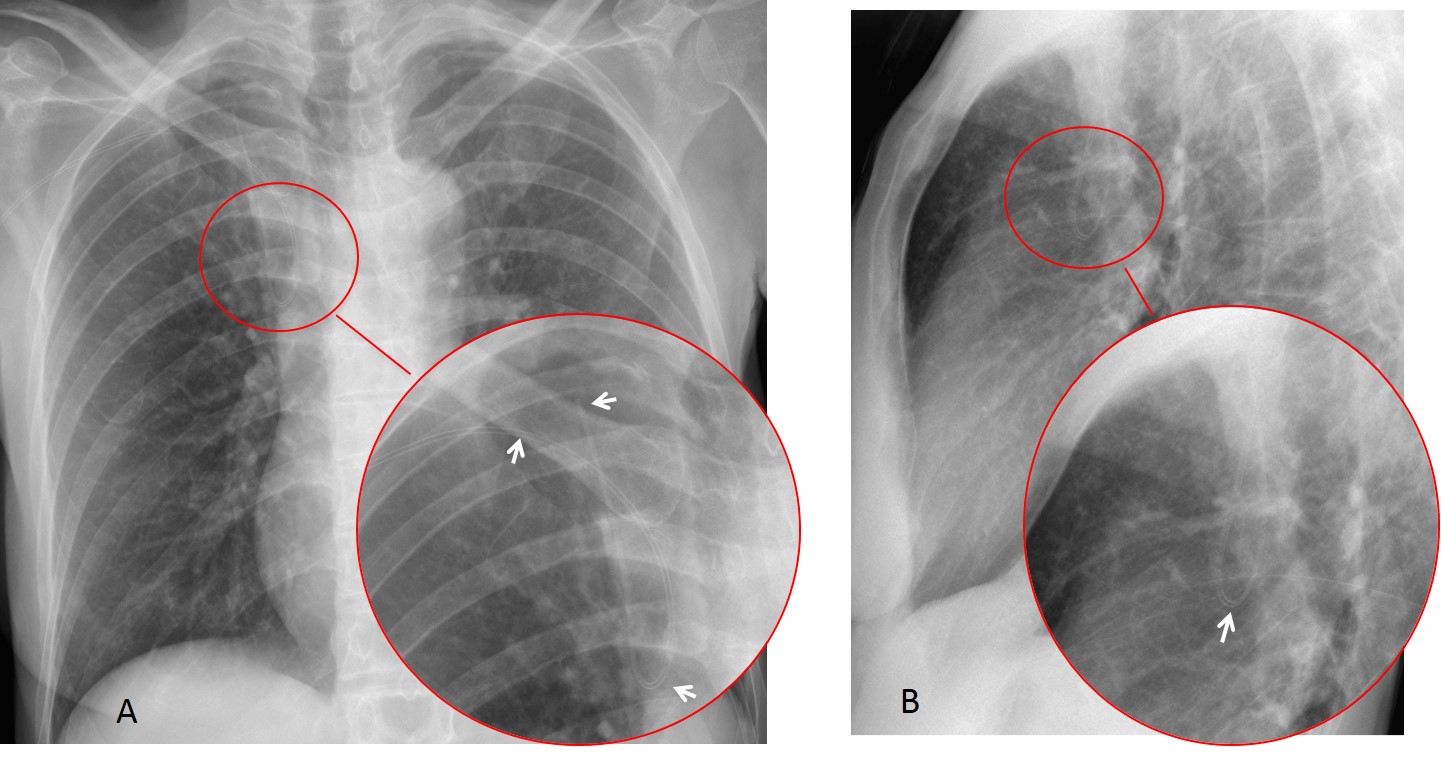
Fig. 8
Fig. 8: central venous catheter looped inside the SVC (A and B, arrows). This may lead to formation of a knot.
Misplaced catheters may end up in the wrong location, such as the jugular vein, azygos vein, or contralateral subclavian vein (Fig. 9). In addition, they may overreach their mark and end up in the inferior vena cava or suprahepatic veins, delivering medication inside the liver with undesirable effects (Fig. 10).
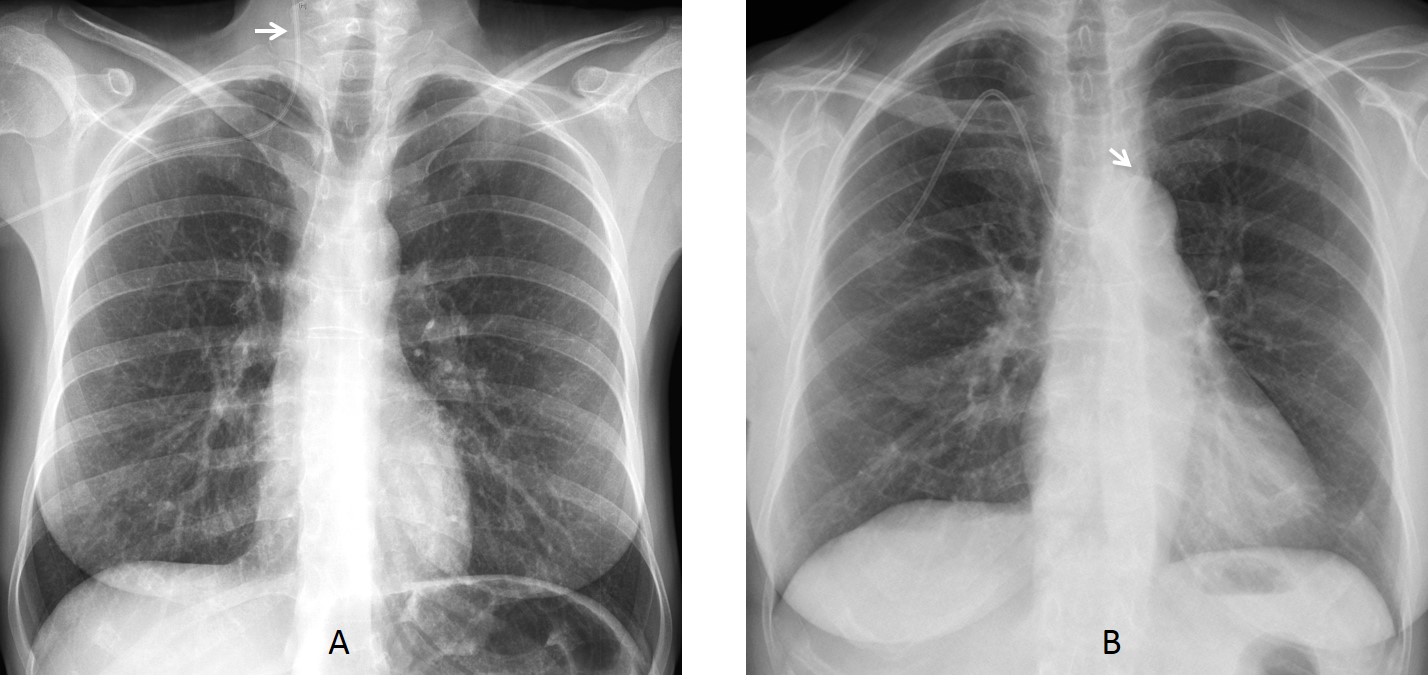
Fig. 9
Fig. 9: two patients with misplaced catheters. In the first one, the catheter has entered the jugular vein (A, arrow). In the second, the catheter has crossed the mediastinum and entered the left subclavian vein (B, arrow).
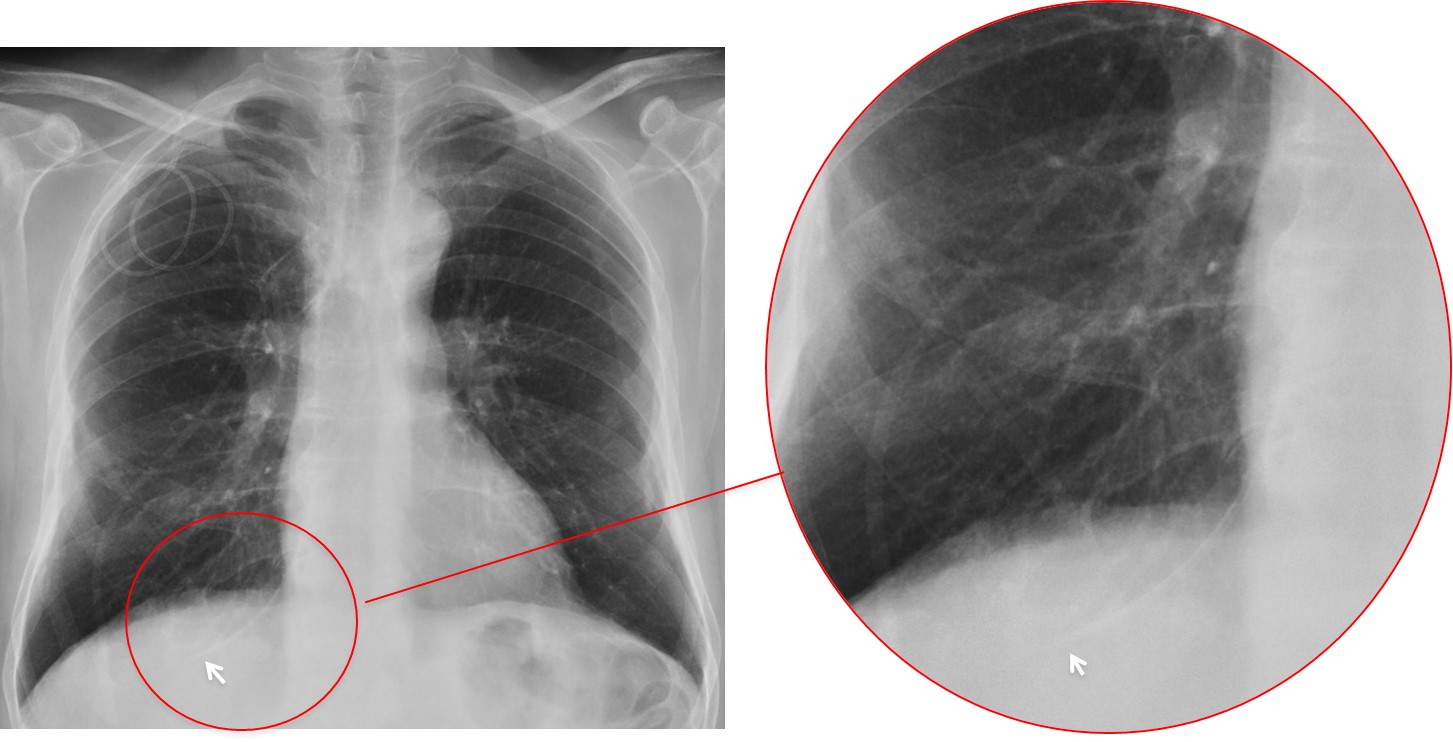
Fig. 10
Fig. 10: in this patient the central venous catheter has gone past the right atrium, and the tip is located in a suprahepatic vein (arrows).
Venous perforation is a rare complication of venous catheters. Perforation is suspected by the unusual location of the catheter tip, together with mediastinal widening and pleural hemothorax (Fig. 11).
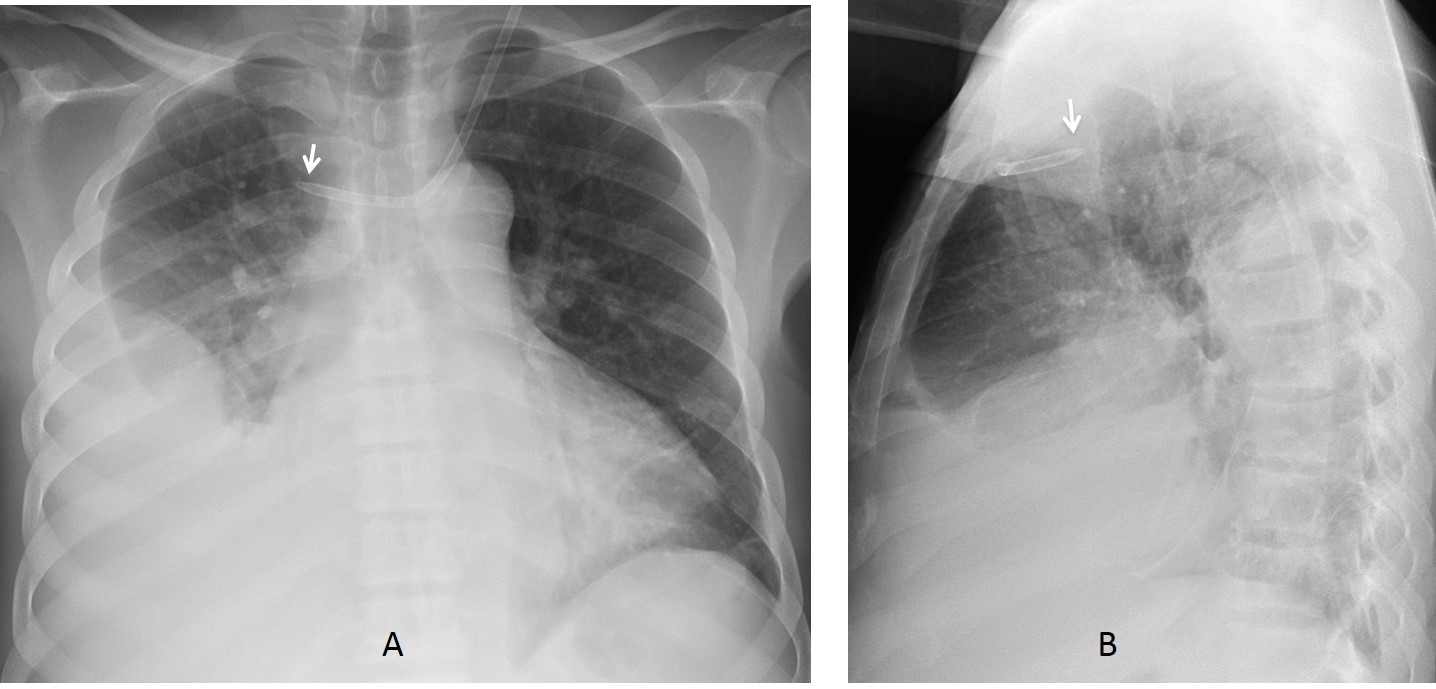
Fig. 11
Fig. 11: catheter perforation of the SVC. The catheter tip is pointing in the wrong direction (A and B, arrows). There is an accompanying pleural effusion.

Follow Dr.Pepe’s Advice:
1. The most common acute complication of endotracheal tubes is placement within the right main bronchus.
2. Placement of pleural tubes in the major fissure is also relatively frequent and easily diagnosed on PA and lateral radiographs.
3. Misplacement of venous lines occurs in up to 40% of patients with these devices.


Thickend pleura…
Pleural fluid on the right is kind of obvious- pleural adhesions possible…
the tracheal tube is too low in the right main bronchus…
i agree
Completely agree
Congratulations for your accurate diagnosis!
CT scout of the chest of a an ill patient with history of thoracotomy and metallic valve replacement.
Multiple Monitor wires and low lined ETT reaching the right lower lobe bronchus.
Also the distal end of the NGT couldn’t be assessed.
Increased density of the right hemithorax due to pleural effusion with possible loculation.
Widening of the superior mediastinum.
….intervento di sostituzione di valvola mitralica con protesi metallica….cuore “mitralico”….sternotomia mediana con “device” di assistenza cardio-respirattoria…..versamento pleurico da ritardata riespansione polmonare dx, come complicanza della intubazione tracheale….il versamento pleurico non è da scompenso del piccolo circolo…..
The scout film of a 76-year-old woman after cardiac surgery reveals right sided pleural effusion. The tip of the endotracheal tube is too low i.e. in the right main bronchus. The tip of the nasogastric tube is in the lower esophagus. There is unfolding of arch of aorta. Multiple sternal sutures and ECG leads are seen in place. Prosthetic Mitral valve is seen.
Very nice description of findings. Thank you.
[…] of a catheter is not very glamorous, but it can avoid significant complications to the patient (see Diploma cases 67 and […]